
Abstract
Background:
Glenohumeral arthropathy after surgery for traumatic shoulder instability is a condition whose etiology and long-term course are still unknown.
Purpose:
To evaluate the risk factors for the onset of arthropathy and to assess the relationship between the degree of arthropathy and final outcomes.
Study Design:
Case series; Level of evidence, 4.
Methods:
We included patients who underwent surgery for a shoulder instability at a single institution between 2000 and 2004. The following variables were studied for relationship with functional outcomes: sex, age, body mass index, smoking at the time of surgery, number of episodes of shoulder dislocation, and time from first dislocation to surgery. The number of anchors used and their position were also evaluated. Functional outcomes were assessed using the Constant-Murley, Western Ontario Shoulder Instability Index, and Rowe scores, and results were compared with the onset of arthropathy according to Buscayret classification. Spearman and Pearson correlations were performed for the association between glenohumeral arthritis (Buscayret grade) and the study variables, the Mann-Whitney U test and Student t test were used to compare outcome scores with the study variables, and the Kruskal-Wallis test was used to compare Buscayret grade and outcome scores.
Results:
A total of 26 shoulders in 25 patients were analyzed, finding a high rate (54%) of arthropathy at a minimum follow-up of 16 years. Patients with Buscayret grade 4 had the worst functional results (P = .007). However, 80% of patients with Buscayret grade ≤3 had excellent Constant-Murley scores. A significant relationship was found between degree of arthropathy and patients who were smokers before surgery (P < .01). No relationship was found between the onset of arthropathy and the other variables analyzed.
Conclusion:
Postinstability glenohumeral arthropathy was not correlated with functional outcomes except in those patients with advanced arthroplasty (Buscayret grade 4). A direct relationship was found between smoking before surgery and the onset of glenohumeral arthropathy.
The risk of sustaining a glenohumeral dislocation is between 0.08 and 0.24 cases per 1000 people per year in developed countries. 21 This injury can lead to the development of an anterior instability, with multiple episodes of dislocation in more than a third of cases. 16 Many studies in the literature speak about management, new techniques, and modifications for the treatment of shoulder instability. However, the long-term complications of this condition and, specifically, postinstability arthropathy, are not well defined.
Glenohumeral arthropathy was first described by Neer et al 14 in patients who underwent surgery for shoulder instability. Subsequently, postinstability arthropathy was formally defined as degenerative joint changes after at least 1 episode of dislocation, regardless of whether the patient has undergone surgery. 19 Overtightening of the capsule and/or subscapularis, use of metallic nonabsorbable anchors, their number or prominent placement, and malposition knots have been established as predisposing factors for onset of arthropathy. 21
Arthroscopic treatment of Bankart lesion is highly widespread and its short-term results reported widely in the literature. However, it is difficult to find studies that analyze the long-term results, especially in relation to the development of postinstability arthropathy. The few cases published about this topic use different types of anchors and have a follow-up time ranging from 8 to 13 years. 5,6,13,17
The aim of this work was to evaluate the incidence of postinstability arthropathy in patients who underwent surgery for arthroscopic repair of Bankart lesion with a minimum follow-up time of 16 years as well as to determine the factors predisposing its onset. In addition, the long-term clinical results of this technique were analyzed in terms of recurrence of dislocation and functional scores.
Methods
A search was performed in our prospective database of all patients who underwent an arthroscopic Bankart procedure at our institution between 2000 and 2004 for unilateral traumatic shoulder instability. Patients with multidirectional instability, glenoid bone defects, superior labral anterior posterior lesions, severe lesions in the labrum contraindicating the repair procedure, associated rotator cuff tears, and degenerative signs before surgery were excluded. Informed consent was obtained from all subjects or, if subjects were aged under 18 years, from parents or legal guardian. This study was approved by the ethics and clinical trials committee of our center, and all methods were carried out in accordance with relevant guidelines and regulations.
Surgical Technique
Surgery was performed in all cases by the same senior surgeon (A.I.F.), who has more than 10 years of experience. The procedure was carried out under general anesthesia and with the patient placed in lateral decubitus. The repair was performed through 3 portals: posterior viewing, anteromedial working, and accessory anterosuperior working and viewing. After detachment of the labrum, the glenoid bed was prepared using an arthroscopic shaver blade. Reinsertion of the labrum was performed using pigtail suture passing devices (Spectrum; ConMed) and, in all cases, one to four 2.3-mm knotless metallic anchors (Knotless Suture Anchor; Mitek Products) were placed, starting at the 5-o’clock position for right shoulders or 7-o’clock position for left shoulders and progressing proximally.
After surgery, patients used a sling for 4 weeks, allowing flexion and extension of the elbow in that period. Subsequently, a 3-phase rehabilitation program was started: first, recovery of passive movement; second, recovery of active movement; and finally, strengthening exercises. Practice of contact sports was delayed until the sixth month following surgery, when the patient was discharged.
Outcomes Assessment
Patients were re-evaluated during 2020 for the purpose of this study; thus, all patients had a minimum of 16 years of follow-up. We collected data on the variables considered to potentially influence the final results: sex, age, body mass index (BMI), smoking status (before surgery and current), number of episodes of dislocation, and time from first episode to surgery. Postoperative complications and relapses were also recorded. The functional outcomes were evaluated using the Constant-Murley (CM), 4 Western Ontario Shoulder Instability Index (WOSI), 12 and Rowe tests. 18
Standard radiographs were taken in 2 planes: anteroposterior and axillary. An independent radiologist specializing in musculoskeletal disease analyzed the result of these radiographs and classified the patients into 5 groups based on the degree of arthropathy according to Buscayret 1 classification (Figure 1) in both the preoperative and postoperative period.

Radiographs showing the different Buscayret grades for glenohumeral arthropathy. Grade 0, no arthropathy; grade 1, presence of humeral osteophyte with a maximum diameter of <3 mm; grade 2, humeral osteophyte between 3 and 7 mm; grade 3, humeral osteophyte ≥8 mm; grade 4, complete obliteration of the glenohumeral joint space.
Statistical Analysis
SPSS statistical software (v 25; IBM) was used for analysis of the data obtained. An initial descriptive analysis of the variables was carried out. Normality was proven using the Shapiro-Wilk test. To evaluate the correlation between glenohumeral arthritis and the different variables (sex, age, BMI, number of previous dislocations, time to surgery, smoking status), the Spearman or Pearson correlation tests were performed. For the comparison between functional outcomes (CM, WOSI, and Rowe scores) and these variables, the Mann-Whitney U test or Student t test was performed. The Kruskal-Wallis test was used to compare functional outcomes with degree of arthropathy. Differences were considered statistically significant at P < .05.
Results
From our database, 32 patients (34 shoulders) met the inclusion criteria; of these patients, 7 were lost to follow-up, 4 due to change of address and 3 who could not be located. Thus, 26 shoulders in 25 patients (20 male, 5 female) were ultimately included. The mean age at first dislocation episode was 22.12 years (range, 14-40 years), the average number of dislocations before surgery was 9.35 (range, 2-19), and the mean age at time of surgery was 28.05 years (range, 18-42 years). The mean time of follow-up for patients was 17.65 years (range, 16-20 years). At latest follow-up, the mean CM score was 82.49 (range, 25.6-99); the mean Rowe sore was 81.35 (range, 50-100); and on the WOSI scale, specific for instability, the mean score was 66.24 (range, 22.3-96.7) (Table 1).
Patient Demographic Data and Clinical Outcomes a
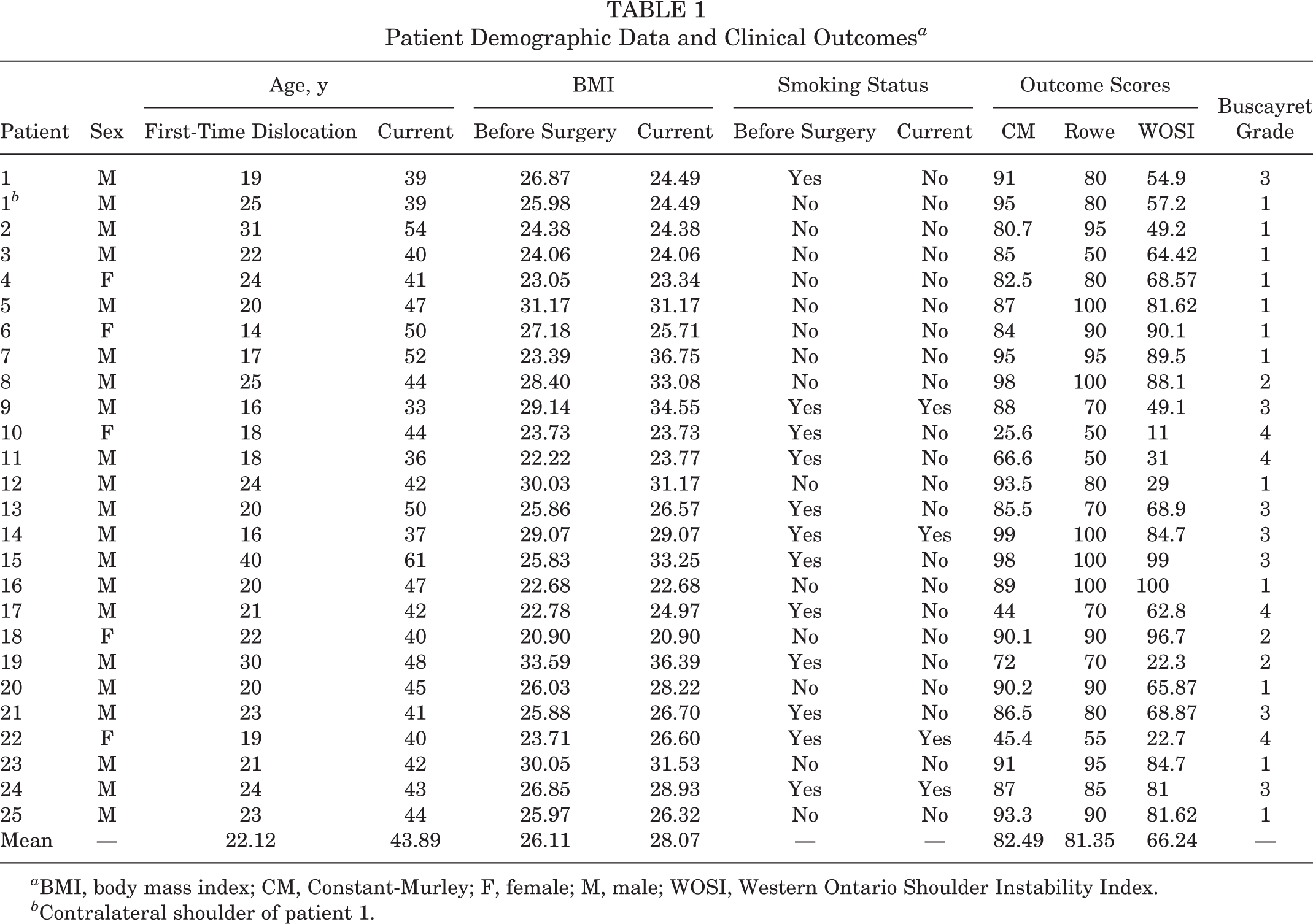
a BMI, body mass index; CM, Constant-Murley; F, female; M, male; WOSI, Western Ontario Shoulder Instability Index.
b Contralateral shoulder of patient 1.
In terms of the degree of arthropathy (Buscayret grade), before surgery, all patients started from grade 0. When evaluated for the study, 12 patients were grade 0 or 1 (46.1%), 3 were grade 2 (11.5%), 7 were grade 3 (26.9%), and 4 were grade 4 (15.3%). Thus, 54% of the patients had some degree of postoperative glenohumeral arthropathy (grade 2, 3, or 4).
The functional outcome according to CM score was excellent in 80% of the patients with Buscayret grades 1 to 3. However, the function decreased when glenohumeral arthropathy was severe (grade 4), with these patients having the worst scores (mean, 45.4 [range, 25.6-66.6]; P = .007) (Table 2).
Functional Outcome Scores by Buscayret grade a

a Data are reported as mean (range). CM, Constant-Murley; WOSI, Western Ontario Shoulder Instability Index.
No statistically significant differences were found in relation to BMI, age of first dislocation, or the total number of episodes of dislocation with respect to outcome scores or degree of arthropathy. When analyzing smoking before surgery, a significant relationship was found with the degree of arthropathy (P < .01). All patients who smoked regularly before surgery had developed some degree of glenohumeral arthropathy (Figure 2). The degree of arthropathy was more severe (grades 3 and 4) compared with the arthroplasty in nonsmoking patients (grades 0-2).

Relationship between arthropathy and smoking. Nonsmoking patients did not surpass grade 2 of glenohumeral arthropathy, while patients who smoked before surgery developed more severe grades of arthropathy (Buscayret grades 3 and 4).
Two patients had an episode of dislocation after the surgery, which is a recurrence rate of 7.7%. In the first case, the dislocation occurred 4 years after the surgery following a sports accident. The patient has not sustained any new episodes of glenohumeral dislocation but has discontinued the sport activity. In the second case, the dislocation occurred 11 years after the surgical procedure. The patient decided to undergo another surgery and has not sustained any new episodes of dislocation to date.
Discussion
The major findings of this study are that the rate of arthropathy in patients who undergo surgery for anterior shoulder instability is high (54%). However, other than grade 4, all grades of arthropathy do not correlate with the functional result, and most patients have an excellent functional score after more than 16 years of follow-up. Moreover, a relationship between smoking before surgery and the onset of glenohumeral arthropathy (P < .01) was found.
Postinstability glenohumeral arthropathy was first described by Samilson and Prieto 19 in 1983 as dislocation arthropathy. Some authors subsequently identified this finding in various procedures, such as Putti-Platt, Magnuson-Stack, Latarjet, Max Lange, Bankart, or Bristow, among others, giving rise to the term capsulorrhaphy arthropathy. 2 Currently, dislocation arthropathy or postinstability arthropathy describes degenerative changes of the glenohumeral joint after at least 1 dislocation with or without surgery for instability. 20
This condition appears predominantly in a young population; its symptoms start with progressive pain and limitation of movement, especially in external rotation (not to mention the history of previous surgery). 20 Other symptoms may include decreased strength of the subscapularis or pain on the posterior side of the shoulder, and posterior subluxation is sometimes identified. Most of these conditions are progressive in nature, ultimately associated with functional limitation of the limb. 8
Samilson and Prieto 19 described the first radiographic classification of this condition based on the joint space and size of the osteophytes. In 2004, Buscayret 1 proposed a modification to that classification, which is currently the version most used.
Since the first reports of glenohumeral arthropathy due to instability were primarily in patients who had undergone surgery, it was initially assumed that the osteoarthritis was a result of the surgery. 17 However, it has been reported that the risk of developing arthritis after a shoulder dislocation, regardless of the treatment, can be up to 20-fold higher compared with the general population. 9
After a first episode of shoulder dislocation receiving conservative treatment, rates of glenohumeral arthropathy of up to 56% have been reported. 8 It is also common after surgery (regardless of whether it is open surgery or arthroscopic and the type of technique used), the incidence ranging from 12% to 62% depending on the case series; those with longer follow-up (more than 10 years) demonstrate a greater rate of arthropathy. 3,8,11,15,17 Perhaps the most exact figures are those of Hovelius et al, 8,9 who estimates postoperative arthropathy at around 56% at 25 years of follow-up. In our study, the percentages of arthropathy are similar (54%).
The results published in the literature show good results regardless of the technique used. 2,8 In our case, a Bankart arthroscopic surgery was performed with metallic anchors with a recurrence rate of 7.7% after a follow-up of more than 16 years, which is, to our knowledge, the case series with the longest follow-up in patients who have undergone surgery with the same technique and same implants. According to the CM score, the result was excellent (score above 80) in 22 shoulders (84.6%); 2 shoulders (7.7%) had good results (score between 66 and 79) and the other 3 (11.5%) had scores below 50, considered poor results.
As indicated in Table 2, if we divide the results according to arthropathy grade, the worst CM scores correspond to patients with Buscayret grade 4, while a high percentage of patients have an excellent functional result regardless of their arthropathy grade (0-3). These results show that, although the rate of arthropathy was high (54%), arthropathy grade ≤3 did not correlate with outcomes scores, and most patients had excellent functional scores at a minimum of 16 years of follow-up. Therefore, we believe that the long-term results of this technique are good despite the high rate of arthropathy.
Some factors, such as the type of instability symptoms (dislocation, subluxation, pain, etc), the level of sport practiced (competitive, recreational, etc), sex, or hand dominance, do not seem to influence the development of arthropathy. 1 Postoperative recurrence (dislocation and/or subluxation) was also not a determining factor. There is also no correlation between the type of surgical technique used and the incidence of arthritis. 10 Although it may be thought that, in the natural history of instability, the number of episodes of dislocation before surgery may influence arthropathy, the only author to find a relationship was Plath et al. 17 In our study, we found that BMI was not related to the onset of arthropathy.
Likewise, some factors that may promote the incidence of arthritis, such as age at first episode, time from first episode of instability to surgery, age at time of surgery, number of implants used, or associated lesions (cuff, associated glenoid cavity or Hill-Sachs lesions), have been reported. 7,8,17 After surgery, it has been demonstrated that the use of metallic implants, protrusion of the implants, knots in the glenohumeral friction area, or excessive anterior plication promote the onset of glenohumeral arthritis. 1,20 In our study, which ranks among the studies with the longest follow-up in the literature, we found a relationship between smoking before surgery and the onset of glenohumeral arthropathy (P < .01).
Limitations
Our study has some limitations in that, being mostly retrospective, it lacks information about the mechanism of dislocation. In addition, no true anteroposterior view (Grashey view) was obtained in radiographs, and the sample is small for obtaining solid recommendations regarding this matter. However, the strengths of the study are the length of the follow-up, the fact that all patients were operated with the same technique and had the same surgeon, and that it is the first study to examine the relationship between arthropathy and smoking.
Conclusion
The incidence of postinstability arthropathy at 16-year follow-up was high (54% of patients with Buscayret grade ≥2); however, there was no clinical correlation except in patients with advanced stage (grade 4). A direct relationship was found between smoking before surgery and the onset of glenohumeral arthropathy. Our findings increase the information available about postinstability glenohumeral arthropathy. Future studies should delve more into this topic.
Footnotes
Acknowledgment
Los autores desean agradecer profundamente a la Sociedad Andaluza de Traumatología y Ortopedia (SATO) por su continuo apoyo científico. Como siempre muchas gracias a Maite Urbano Luque, María de los Ángeles Miñarro del Moral y Juan Carlos Díaz Alcaide por su ayuda y apoyo incondicionales. La vida es mejor gracias a ellos.
(All the authors would like to deeply thank the Andalusian Society of Traumatology and Orthopedics (SATO) for their continuous scientific support. And as always, many thanks to Maite Urbano Luque, María de los Ángeles Miñarro del Moral and Juan Carlos Díaz Alcaide for their unconditional help and support. Life is better because of them.)
Final revision submitted May 1, 2022; accepted August 2, 2022.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University Hospital Reina Sofía (reference No. 279/3954).