
Abstract
Background:
To our knowledge, there have been no previous efforts to evaluate the prevalence of Kaplan fiber (KF) injury in skeletally immature patients with an acute anterior cruciate ligament (ACL) tear on magnetic resonance imaging (MRI) nor has there been any comparison of the reliability of previously described KF diagnostic criteria in this cohort.
Purpose:
To define the prevalence of KF injury in the setting of acute ACL tears using MRI performed within 90 days of injury among skeletally immature patients, and to compare the reliability of MRI in detecting KF injuries using 2 previously described diagnostic criteria.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Skeletally immature patients with an acute ACL tear confirmed using MRI within 90 days of injury were assessed. Two fellowship-trained musculoskeletal radiologists independently interpreted each MRI scan twice. KF injury was first assessed using the Van Dyck scheme (grade 0, normal; grade 1, periligamentous; grade 2, partial tear; and grade 3, complete tear). MRI scans were then reviewed again using the KF injury criteria proposed by Batty. Discrepancies in KF injury schemes were adjudicated by a third musculoskeletal radiologist. Interrater agreement for both methods was determined using Cohen κ.
Results:
Included were 45 patients (33 male, 12 female) with a mean age of 13.2 ± 1.6 years. KF injuries were identified in 17 of 45 (37.7%) knees of using the traditional Van Dyck grading scheme (interrater agreement κ = 0.40). The Batty diagnostic criteria identified KF injury in 5 of 45 (11.1%) (interrater agreement κ = 0.45); 17 (37.8%) MRI scans required a third reviewer adjudication for the Van Dyck scheme, while 4 (8.9%) required a third reviewer using the Batty criteria.
Conclusion:
The Batty diagnostic criteria detected a lower KF injury prevalence than previously reported in the adult population, while the Van Dyck prevalence was similar to rates in adult populations. Both grading criteria had poor interrater reliability in diagnosing a KF injury.
Failure of primary anterior cruciate ligament (ACL) reconstruction remains unacceptably high, with reoperation rates ranging from 6.5% to 34%. 6 Lower patient age at the time of primary ACL reconstruction is a significant risk factor for revision surgery, with the pediatric and adolescent patient populations at a particularly elevated risk. 10,13,14 The contributing factors to this phenomenon are likely multifactorial and could involve the known limitations of certain graft options, errors in surgical technique, and/or the desire to return to certain pivoting sports that have been associated with high rates of reinjury. 9,14 Failure to reestablish rotational stability after ACL reconstruction has been linked to poor patient-reported outcomes and increased risk of graft failure. 2,20,21 As a result, there has been a significant focus on defining the secondary stabilizers of rotatory knee stability. Furthermore, it has been theorized that unaddressed injury to these structures in particular may contribute to higher graft failures and poor patient-reported outcomes. 1
The anterolateral complex of the knee plays a critical role in conferring anterolateral rotatory stability in the setting of an ACL tear. 1,8,9 Two-year outcome data from the STABILITY trial indicate that younger patients at higher risk for failed primary ACL reconstruction may benefit from the addition of a lateral extra-articular tenodesis. 9 These findings suggest that surgically addressing the anterolateral knee during primary reconstruction in at-risk patients decreases ACL reconstruction failure rates. In an attempt to reach a consensus defining the anterolateral structures of the knee, the International Anterolateral Complex Consensus Group defined the components of the anterolateral complex to include the anterolateral ligament, the superficial iliotibial band, and the deep iliotibial band with the Kaplan fiber (KF) system. The KF system consists of 2 discrete bundles that run from the deep iliotibial band to the posterolateral metadiaphyseal region of the distal femur, attaching at 6.8 and 4.8 cm proximal to the distal femoral joint line. 1,11,12,16 Biomechanical testing of the KF system has demonstrated that it plays a role in conferring resistance to internal tibial rotation as the knee goes through flexion in an ACL-deficient knee. 7 A clearer understanding of the prevalence of KF injuries will aid in better defining the role KF plays in knee stability and potentially aid in identifying patients that may benefit from additional anterolateral knee augmentation procedures at the time of index primary ACL reconstruction.
There have been multiple studies using novel diagnostic criteria to define the prevalence of KF injury on magnetic resonance imaging (MRI) scans in the setting of acute ACL tears among skeletally mature patients, and reported rates have ranged from 23% to as high as 71% depending on the criteria. 4,17,18,22 To date, there has been no investigation to our knowledge into the incidence of KF injuries in skeletally immature patients with ACL tears nor has there been a study comparing KF injury rates and interrater reliabilities among the different diagnostic criteria.
The primary objective of the current study was to determine the prevalence of KF injury in skeletally immature patients with acute primary ACL tears using the 2 most commonly cited MRI-based diagnostic criteria. 4,22 A secondary objective was to report the interrater agreement between the fellowship-trained musculoskeletal radiologists so as to characterize the diagnostic utility of these injury criteria. We hypothesized that the observed prevalence for each diagnostic criteria would match those reported in the original studies in which they were described, and that both criteria would demonstrate interrater reliabilities that substantiate their routine use in diagnosing KF injuries. 19
Methods
Patient Population
Institutional review board approval was obtained before undertaking this retrospective review. All patients aged under 18 years who underwent primary ACL reconstruction between 2006 and 2020 were identified from a database of ACL injuries presenting to a tertiary referral center. A database of these patients was created and the medical record, knee radiographs, and knee MRI scans were reviewed. Inclusion criteria for the study included open distal femoral and proximal tibial physes on plain radiographs, complete tear of the ACL on MRI, and MRI performed within 90 days of the date of injury. Exclusion criteria included history of previous ipsilateral ACL injury, multiligamentous knee injury, grade 3 medial collateral ligament (MCL) tear, and failure to image the knee within 90 days of the date of stated injury. If plain radiographs showed partial closure of either the distal femoral or proximal tibial physes, the knee was excluded from the study.
MRI Review
Included MRI examinations were performed in multiple radiology centers throughout the local region with 3.0-T or 1.5-T magnets. Standard imaging protocols were used, with slice thickness cuts of 3 mm and 4 mm. All examinations were noncontrast and used 3-plane imaging to include axial, coronal, and sagittal views. Protocols incorporated a combination of T1, fat-suppressed T2, proton density, and fat-suppressed proton-density sequences. The variation of sequencing and formatting observed is representative of that seen by a clinician practicing in the United States.
Following screening of eligible patients, 2 fellowship-trained musculoskeletal radiologists (D.B., J.M.B.) independently reviewed knee MRI scans at 2 different times in a sequential manner with approximately 1 month between each sequence of MRI scan reads. On each review, the proximal and distal KF bundles were assessed on axial, coronal, and sagittal sequences. Previously described anatomic landmarks were used to localize the KF complex. The proximal and distal KF bundles attached on the posterolateral metadiaphyseal region of the distal femur at 6.8 cm and 4.8 cm, respectively, from the distal femoral joint line with superior lateral geniculate artery running just distal to the distal KF bundle. 11 On the first MRI scan review, the KFs were assessed using the KF grading scheme first described by Van Dyck et al. 22 This injury scheme features a traditional grade 0 through grade 3 scheme (Table 1). Grade 0 (Figure 1) is consistent with no injury, grade 1 injury is defined as periligamentous edema about the KF, grade 2 is a partial disruption or irregular contour with ligamentous edema, and grade 3 is complete disruption of the KF at the midsubstance or a femoral avulsion. 22
Grading Schemes for KF Injury a
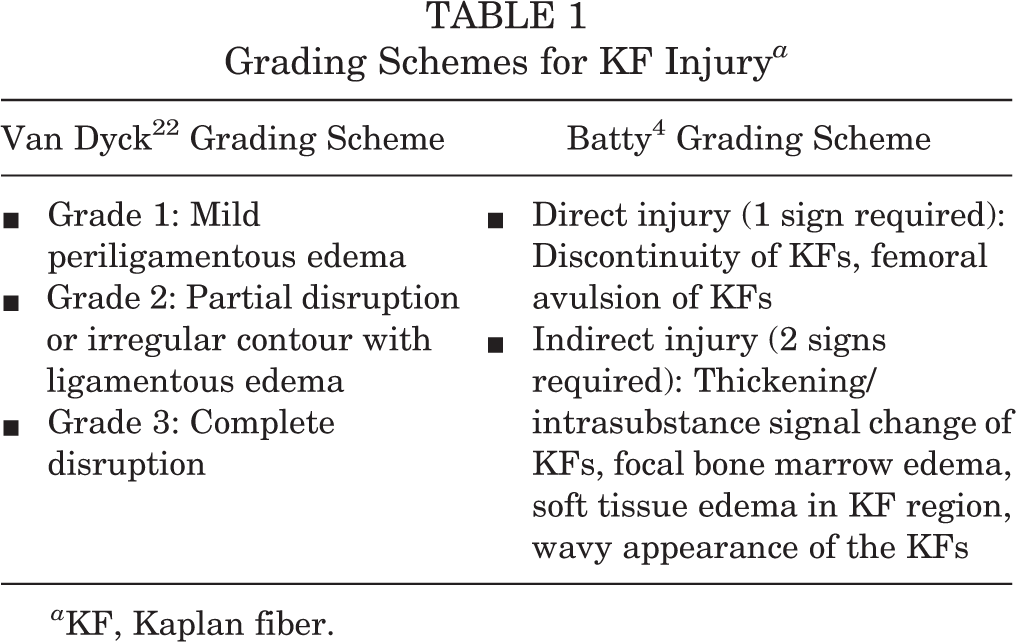
a KF, Kaplan fiber.

A 3.0-T coronal proton-density magnetic resonance image of a right knee demonstrating intact KF complex (arrows) pointing to the proximal and distal KF bundles. KF, Kaplan fiber.
On the second MRI review, KF injury was assessed using the diagnostic criteria proposed by Batty et al. 3,4 This criteria required 1 sign of direct injury or 2 signs of indirect injury to the KF complex to constitute a KF injury. 4 Discontinuity of the KFs or femoral avulsion both constitute a KF injury (Figure 2). Indirect injury criteria include thickening or intersubstance signal change of the KF, focal bone marrow edema at the KF femoral insertion, soft tissue edema in the region of the KFs, or a wavy appearance to the KFs. For both criteria, if the KFs could not be observed in their described anatomic location and there was an absence of edema in this region it was determined there was no KF injury.
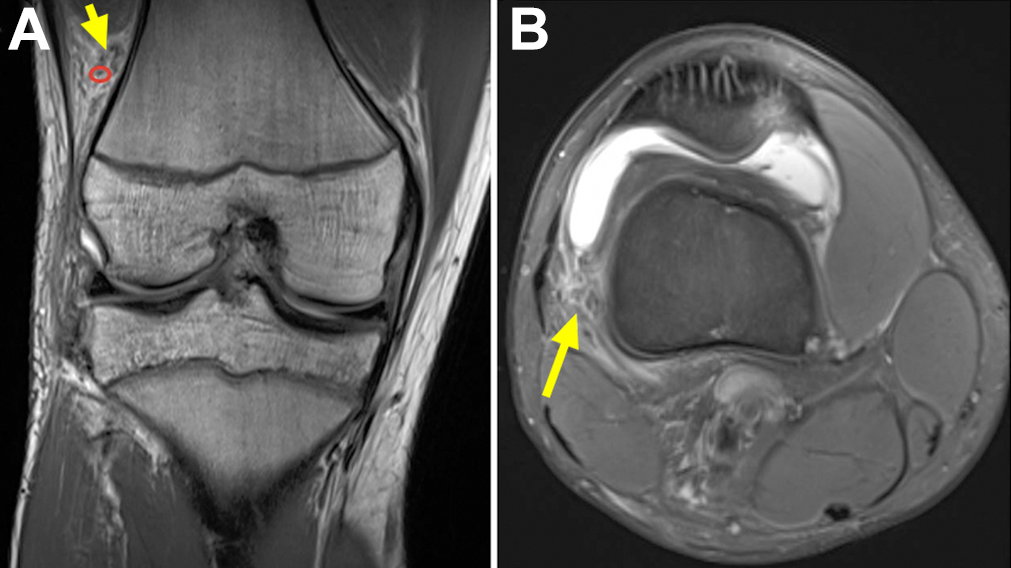
(A) Coronal and (B) axial 3.0-T proton-density magnetic resonance images of a right knee demonstrating complete discontinuity of the Kaplan fiber complex (arrows) and nearby superior geniculate artery (red circle).
Statistical Analysis
All data were collected in Microsoft Excel. Descriptive statistics were performed for all demographic variables. The interrater reliability of each grading scheme was defined using the Cohen kappa coefficient (κ). The calculated κ values were categorized as having slight (0-0.20), fair (0.21-0.40), moderate (0.41-0.60), substantial (0.61-0.80), and excellent (0.81-1.00) agreement. 15 A κ value greater than 0.8 was used as a threshold constituting acceptable diagnostic utility. 19 After third-reviewer (N.D.C.) adjudication for both sets of graded MRI scans was complete, the KF injury prevalence was calculated as a percentage. For the Van Dyck et al 22 grading scheme, grades 1 to 3 were all counted as injuries, which is consistent with the originally published study. Associations for age, sex, meniscal tear, Segond fracture, and magnet strength were tested for both sets of results from the 2 grading schemes using an independent t test, chi square test, or Fisher exact test.
Results
A total of 45 patients with knee MRI scans in the setting of acute, complete ACL tears met inclusion criteria. The mean patient age was 13.2 ± 1.6 years (range, 8-16 years) with 33 men (73.3%) and 12 women (26.7%). The median time from injury to MRI was 11 days. A total of 33 (73.3%) MRI examinations were performed on a 1.5-T MRI machine, while the remaining 12 (26.7%) were performed on a 3.0-T scanner. There were 8 (17.8%) MRIs with a concomitant medial meniscal tear present, and 8 (17.8%) cases with a concomitant lateral meniscal tear present. In 4 (8.9%) patients, Segond fractures were observed, and grade 1 or 2 MCL injuries were present in 13 (28.9%) of the included MRI scans.
Using the Van Dyck injury grading scheme, KF injury was detected in 17 of 45 MRI scans (37.7%; 95% confidence interval [CI], 23.6%-51.9%). The Batty KF injury diagnostic criteria detected KF injury in 5 of 45 MRI scans reviewed (11.1%; 95% CI, 1.9%-20.2%). Table 2 details the interrater agreement for both KF injury criteria. In 3 of the 45 reviewed MRI scans, 1 of the reviewers was unable to identify the KF complex in the described anatomic location with the absence of edema. These 3 reads were marked as no KF injury in both criteria.
Interrater Agreement a
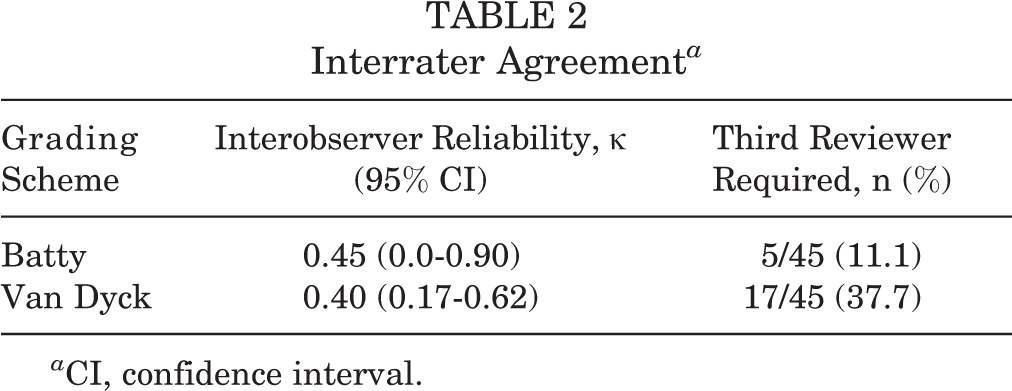
a CI, confidence interval.
Age was the only variable that was associated with the presence of a KF injury using the Van Dyck scheme. Those diagnosed with KF injury using the Van Dyck scheme averaged 14.1 ± 1.2 years compared with those who did not have a KF injury, with an average age of 12.7 ± 1.6 years (P < .0039). Table 3 details all variables analyzed for significance with KF injury.
Variable Associations with KF Injury Based on Grading Scheme a

a Values given are mean ± SD or count (column percentage). Boldface P value indicates significant association (P < .05). KF, Kaplan Fiber.
Discussion
The main findings of this study were that the prevalence of KF injury in acute skeletally immature ACL tears are detected less frequently than in the adult population using the Batty et al 4 diagnostic criteria, while KF injuries occur at the same rate using the Van Dyck et al 22 grading scheme. Therefore, our primary hypothesis was partially disproven, with only 1 of the 2 criteria detecting a skeletally immature KF injury prevalence at the same rate as the adult population. 4,17,22 Of equal importance, neither diagnostic criteria reliably detected KF injuries when applied by independent musculoskeletal radiologist reviewers. Thus, the secondary hypothesis was disproven, as both injury diagnostic criteria failed to meet a sufficient kappa for clinical utility. The findings of the present work indicate that MRI-based KF injury diagnostic criteria are unreliable and are of marginal benefit in furthering understanding of the role the anterolateral complex plays in the setting of acute ACL tear.
The prevalence of KF injury in acute ACL tear among adults has been reported to be between 23% and 71% using various KF injury criteria. 4,5,17,18,22 The published criteria of Batty et al 4 reported an acute KF injury rate of 23.7%. The present study found a KF injury rate of 11.1% (95% CI, 1.9%-20.2%), which suggests that KF injury may be less common in the skeletally immature patient population or that the Batty et al 4 KF diagnostic criteria are less reliable in the pediatric population. The 37.7% incidence of KF injury found among the present cohort using the Van Dyck et al 22 grading scheme is similar to previous studies looking at an adult population, with reported rates of 33% to 39%. 17,22 The observed difference in prevalence between the 2 injury criteria can be explained by the fact that isolated periligamentous edema is not considered a KF injury in the Batty scheme. In addition, the Batty group showed that the incidence of KF injury detected on MRI scans outside of the first 90 days from the date of injury was roughly a quarter of the initial rate at 6.4%. 4 The findings of the present study suggest that these structures are not concomitantly injured in the setting of an acute ACL tear at a higher rate than those in the adult population, and, as such, are not likely to be a contributing factor to the higher rate of primary ACL reconstruction failure in younger patients.
The interrater reliability for both KF diagnostic criteria in the present study failed to meet the minimally accepted agreement for use as a clinical diagnostic tool (κ ≥ 0.8). 19 Use of the Batty et al 4 criteria yielded an interrater agreement among blinded fellowship-trained musculoskeletal radiologists of κ = 0.45, which is considered moderate interrater agreement, but lacks reproducibility for clinical use by modern medical diagnostic standards. 19 The original Batty et al 4 study applied this criteria to an adult population with ACL tears but did not calculate a κ statistic for interrater agreement in diagnosing KF injury. Furthermore, the study examined interrater agreement for the various characteristics within the scheme and yielded an agreement of 75% to 99% between reviewers; however, agreement-percentage calculations are prone to overestimate the true agreement of reviewers. 4,19 Similarly, use of the Van Dyck grading scheme in the present study had an interrater agreement of κ = 0.40, which is substantially less than the 0.92 kappa reported in the original publication. 22 These findings suggest that both of these schemes may have limitations that preclude routine use in subsequent efforts to better understand the nature of KF injuries. Standardized MRI scan sequence protocols that establish a requisite quality of imaging required for KF injury analysis may be beneficial in improving interrater agreement, as slice thickness, sequence type, and field of view can all be variable from scan to scan. Future investigations may consider a modification of the Van Dyck et al 22 grading scheme where type 1 edema is not considered an injury to the KF system.
The only significant association found between the presence of KF injury and other examined variables was in relation to age with the Van Dyck group. The average age of a patient with a KF injury was 14.1 years versus those who did not have a KF injury, with an average age of 12.7 years (P = .0039); however, this finding was not replicated in the Batty group. Given the small size of the present study, these findings would need to be validated in a larger series. Sex, magnet strength, the presence of a medial or lateral meniscal tear, a Segond fracture, and grade 1 or 2 MCL tear were not associated with KF injury. These findings are in contrast to those of the study by Batty et al, 4 in which lateral meniscal tears, posteromedial tibial edema, lateral collateral ligament injury, and MCL injury were all associated with the presence of KF injury meeting the Batty KF injury criteria.
Limitations
This retrospective study has a number of limitations. The conclusions of the current study are diminished by the small number of patients in the series, lack of correlating clinical data on patient laxity and pivot shift testing, and lack of surgical confirmation of KF injury in those diagnosed on MRI scans. However, this is the first analysis of the reliability of MRI to detect KF injuries in skeletally immature patients. In addition, the time from injury to MRI in the original Van Dyck study was 6 weeks, whereas in the present study all MRI scans performed within 90 days of the date of injury were included to match the delineation made for an acute MRI scan following ACL injury in the Batty et al 4 study. 22 Finally, for both criteria employed in the present study, in cases where the KFs were not identified and there was an absence of boney and soft tissue edema at the anatomic location of the KF system, the examination was read as no injury. This assumption potentially underestimates the rate of KF injury.
Conclusion
The Batty diagnostic criteria detected a lower KF injury prevalence than reported previously in the adult population, while the Van Dyck prevalence was similar to rates reported in adult populations. Both criteria had relatively poor interrater reliability in diagnosing a KF injury. Future studies focused on developing more reliable MRI KF injury diagnostic criteria may yield a clinical tool that permits surgeons to better study the clinical implications of KF injuries on the clinical outcomes of ACL injuries.
Footnotes
Final revision submitted July 14, 2022; accepted July 27, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.B.L., E.R.S., and D.C. have received education payments from MedInc of Texas. V.M. has received consulting fees from Smith & Nephew. M.R.S. has received education payments from Arthrex and hospitality payments from Stryker. A.J.S. has received grant support from Arthrex and education payments from Arthrex and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Brooke Army Medical Center (reference No. C.2013.134d/391024).