
Abstract
Background:
The syndesmotic screw (SS) and suture button (SB) fixation methods are both widely used for the reduction of ankle syndesmotic injury, with varying outcomes.
Purpose:
To review recently published randomized controlled trials (RCTs) to assess the outcomes between SS and SB fixation for ankle syndesmotic injury.
Study Design:
Systematic review; Level of evidence, 1.
Methods:
The PubMed, Embase, ClinicalTrials.gov, and Cochrane databases were searched for relevant RCTs published between 1966 and 2021 according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Eligible studies were RCTs comparing SS and SB fixation for ankle syndesmotic injury. The risk of bias was evaluated using the Cochrane Risk of Bias tool. Primary outcomes included complications, malreduction, and unplanned reoperation, and secondary outcomes were the American Orthopaedic Foot & Ankle Society (AOFAS) score, Olerud-Molander ankle score (OMAS), and EuroQol-5 Domain (EQ-5D) score. The mean difference (MD) and risk ratio (RR) were calculated for continuous and dichotomous outcomes, respectively. Random- or fixed-effects model was applied according to heterogeneity.
Results:
Of 389 studies, 8 RCTs involving 512 patients were included. Overall, 257 patients received SS fixation and 255 patients received SB fixation. The 2 groups did not differ significantly in malreduction (RR, –0.06; 95% CI, –0.18 to 0.07) or EQ-5D (MD, 0.01; 95% CI, –0.01 to 0.03). However, the SB group showed significant advantages over the SS group in complications (RR, 0.42; 95% CI, 0.26 to 0.66), unplanned reoperation (RR, 0.62; 95% CI, 0.43 to 0.89), AOFAS score (MD, 3.04; 95% CI, 1.77 to 4.31), and OMAS (MD, 4.51; 95% CI, 1.54 to 7.48). The risk of bias of the included studies was acceptable.
Conclusion:
The results showed that there were no significant differences between the SS and SB groups in malreduction and EQ-5D scores. However, the SB group had significantly better local irritation rates, unplanned reoperation rates, AOFAS scores, and OMASs.
The syndesmosis is a micromovement joint composed of the distal fibula, tibia, and a complex of 4 ligaments, which is important to maintain ankle stability. 4,17,28 Syndesmotic injuries account for 5% to 10% of ankle sprains and 20% of ankle fractures, 16,31,33 typically caused by supraphysiologic ankle external rotation. 13,38 Syndesmotic injury accompanied with ankle fracture usually requires surgery and correct reduction of the syndesmosis, which is critical to prevent further deterioration of the ankle joint, such as osteoarthritis, and sustainable chronic pain. 3,7,36
The gold standard of fixation for syndesmotic injury is syndesmotic screw (SS) fixation. 25,41 The disadvantages of SSs include screw breakage, local irritation, syndesmosis malreduction, nonanatomic reduction, the need for removal, unclear screw size and number, and an unspecific number of cortices penetrated. 12,23,25 The suture button (SB) was introduced to address these problems. The SB is known for promoting early healing and anatomic reduction and does not require regular removal. 9,35,40 Moreover, the SB has demonstrated similar or better biomechanical results and equivalent strength compared with the SS. 1,8
Several studies have compared the advantages and disadvantages of SSs and SBs; however, it remains unclear whether the SB is preferable to the SS. 2,5,14,15 In addition, numerous systematic reviews and meta-analyses, both randomized controlled trials (RCTs) 9,27,34 and mixed RCTs and non-RCTs, 21,39,40 have been conducted to find out the best approach, but their evidence and results have varied. In the first group of reviews, 9,27,34 the included RCTs were not the latest ones, and their outcomes were insufficient; in the second group, 21,39,40 the quality of evidence was limited by the included studies.
The purpose of the current study was to conduct a meta-analysis of the latest RCTs to assess complication rate, malreduction, unplanned reoperation, and functional outcomes between SS and SB fixation methods for syndesmotic injury.
Methods
Study Selection
From 1966 to September 2021, we searched for relevant studies published from 1966 to September 2021 from the Embase, PubMed, ClinicalTrials.gov, and Cochrane databases. Search terms for PubMed included “endobutton,” “button?,” “endo-button,” “tightrope,” “suture button,” “flexible fix*,” “syndesmo*,” “distal tibiofibular syndesmosis,” “syndesmotic injury,” “screw?,” “syndesmo* screw?,” and “rigid fix*,” and we also searched within the reference lists of other articles. 9,21,27,34,39,40
All the RCT studies were included if they compared the outcomes of SBs and SSs in patients with syndesmotic injury. Exclusion criteria included (1) non-English studies, (2) cadaveric studies, (3) the same follow-up group of patients at different follow-up times, and (4) duplicate studies.
Two authors (B.X. and S.W.) independently reviewed the titles and abstracts of all the studies to exclude unrelated studies; the remaining studies were evaluated by reading the full text. Any disagreements were addressed by discussion or by involving a third author (W.C.).
Data Extraction
We retrieved baseline study information, including publication year, sample size, mean age, interventions, fracture types, follow-up, and percentage of patients analyzed. The primary outcomes were complications (local irritation, implant failure, and infection), malreduction (side-to-side difference in syndesmotic width of ≥2 mm between normal and injured ankles 18,24 ), and unplanned reoperation for accidental reasons (eg, local irritation and infection). The secondary outcomes were functional scores, including the American Orthopaedic Foot & Ankle Society (AOFAS) score, Olerud-Molander ankle score (OMAS), and EuroQol-5 Domain (EQ-5D) score. Two authors (B.X. and S.W.) extracted the data independently and then compared the final results, and any discrepancies were addressed by discussion.
Quality Assessment
The methodological quality of the included RCTs was evaluated by 2 independent investigators (J.T. and S.W.). The RCTs were assessed with the Cochrane Risk of Bias tool, which includes 7 biases: (1) random sequence generation, (2) allocation concealment, (3) blinding of participant and personnel, (4) blinding of outcome assessment, (5) incomplete outcome data, (6) selective reporting, and (7) other bias. Each part was classified as low risk, high risk, or unclear. Any disagreements were addressed via discussion or by the senior investigator (K.T.).
Data Analysis
Dichotomous data were analyzed using risk ratios (RRs) and 95% CIs, and continuous variables were analyzed using mean differences (MDs) and 95% CIs (if an RCT provided median values, then the P value, interquartile range, and mean ± SD would be calculated according to corresponding statistical methods). 22,37 Acceptable heterogeneity between the included studies was defined as I 2 ≤ 50% and P > .1. Under this circumstance, a fixed-effects model was applied; otherwise, a random-effects model was applied. All calculations were performed using Revman (Version 5.4; Cochrane). A funnel plot was made to evaluate the publication bias, and sensitivity analysis was performed to provide a robust result.
Results
Search Findings and Study Characteristics
A total of 389 studies were yielded after the electronic search. After duplicates were removed, the remaining studies were first screened by title and abstract, and then by full text. Ultimately, 8 RCTs, 5,6,18 –20,29,30,32 all published between 2009 and 2021, were included in this meta-analysis. The study retrieval process is shown in Figure 1. We included 2 studies 18,20 whose follow-up patients were the same because their results were reported at different times.

Flowchart of study screening and selection using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. RCT, randomized controlled trial.
The 8 included RCTs 5,6,18 –20,29,30,32 involved 512 patients with syndesmotic injuries, 255 of whom received SB and 257 of whom received SS fixation. The average follow-up was 33.7 months and the average age was 42.5 years. According to the available information, there were 59 patients with Maisonneuve fractures, 31 with Weber C, 11 with Weber B, 274 with AO-44C, and 10 with AO-44B fractures; 7 studies 5,6,18 –20,29,32 used TightRope as an SB, 1 study 30 used Ziptight, 5 studies 6,18,20,30,32 used tricortical screws, 3 studies 5,19,29 used quadricortical screws, 6 studies 6,18 –20,30,32 used 3.5-mm SSs, 1 study 29 used 4.5-mm SSs, and 1 study 5 used SSs from 3.5 to 6 mm (Table 1).
Characteristics of the Included Studies a

a NA, not available; AO, ; SB, suture button; SS, syndesmotic screw.
Quality Assessment and Risk of Bias
Overall, the quality of included studies was acceptable; 50% showed an unclear or high risk of performance bias, and 75% showed a unclear or high risk of detection bias, and 25% had a high risk of detection bias, and 12.5% had a high risk of reporting bias. (Figure 2).

Primary Outcomes
Complications
All studies reported complications: 7 studies 5,6,18 –20,30,32 reported local irritation and infection (deep or superficial), and 6 studies 6,18 –20,29,30 reported implant failure. This calculation did not show much heterogeneity (I 2 = 15%; P = .27), and the SS group showed significantly higher risk of complication (RR, 0.42; 95% CI, 0.26-0.66). There was no significant difference in the subgroups of infection (RR, 1.69; 95% CI, 0.62-4.59) and implant failure (RR, 0.39; 95% CI, 0.14-1.09). The main significant difference, however, was observed in the local irritation section (RR, 0.23; 95% CI, 0.11-0.46) (Figure 3).

Malreduction
Five studies 18,20,29,30,32 reported data on malreduction. Studies that did not use the defined standard for malreduction (ie, side-to-side difference in syndesmotic width of ≥2 mm) were excluded from the meta-analysis. Across all the studies, there was no significant difference between the SB and SS groups (RR, –0.06; 95% CI, –0.18 to 0.07). The heterogeneity was a little higher than the standard (I 2 = 52%; P = .08) (Figure 4).

Unplanned Reoperation
Eight studies 5,6,18 –20,29,30,32 reported the date of unplanned reoperation after the primary surgery, and a significant difference was observed between the SB and SS groups (RR, 0.62; 95% CI, 0.43-0.89; I 2 = 38%; P = .13) (Figure 5).

Secondary Outcomes
AOFAS Score
Five studies 5,6,19,29,30 reported the AOFAS score at different follow-up times. The data showed acceptable heterogeneity (I 2 = 42%; P = .03), and a significant difference was found between the 2 groups (MD, 3.04; 95% CI, 1.77 to 4.31). There was no significant difference 2 years after the surgery (MD, 2.46; 95% CI, –0.26 to 5.18), but a significant difference was observed at follow-up periods of ≤3 months (MD, 3.21; 95% CI, 0.13 to 6.29), 6 months (MD, 2.91; 95% CI, 0.33 to 5.49), 12 months (MD, 2.76; 95% CI, 0.37 to 5.15), and 5 years (MD, 5.40; 95% CI, 1.09 to 9.71) (Figure 6).

Olerud-Molander Ankle Score
Six studies 6,19,20,29,30,32 reported OMAS data and evident heterogeneity was found (I 2 = 62%, P = .0004). The total effects favored the SB group (MD, 4.51; 95% CI, 1.54-7.48); only 1 subgroup (1 year after the surgery) showed a significant difference (MD, 4.40; 95% CI, 1.48-7.33). Subgroups of ≤3 months (MD, 5.27; 95% CI, –0.9 to 11.45), 6 months (MD, 6.49; 95% CI, –2.20 to 15.17), 24 months (MD, 2.17; 95% CI, –13.31 to 17.65), and more than 36 months (MD, 0.16; 95% CI, –17.56 to 17.87) showed no difference between the 2 groups (Figure 7).

EQ-5D Score
Three studies 29,30,32 reported the EQ-5D score. The data showed no significant difference between the SB and SS groups. The heterogeneity was acceptable (MD, 0.01; 95% CI, –0.01 to 0.03; I 2 = 44%; P = .05), and similar results were found at follow-up periods of ≤3 months (MD, 0.05; 95% CI, –0.01 to 0.1), 6 months (MD, 0.04; 95% CI, 0.00 to 0.07), 12 months (MD, 0.01; 95% CI, –0.03 to 0.04), 24 months (MD, –0.03; 95% CI, –0.08 to 0.02), and 5 years (MD, 0.00; 95% CI, –0.07 to 0.07) (Figure 8).

Publication Bias
The funnel plot of studies reporting data on unplanned reoperation was asymmetric, indicating a potential risk of publication bias (Figure 9).
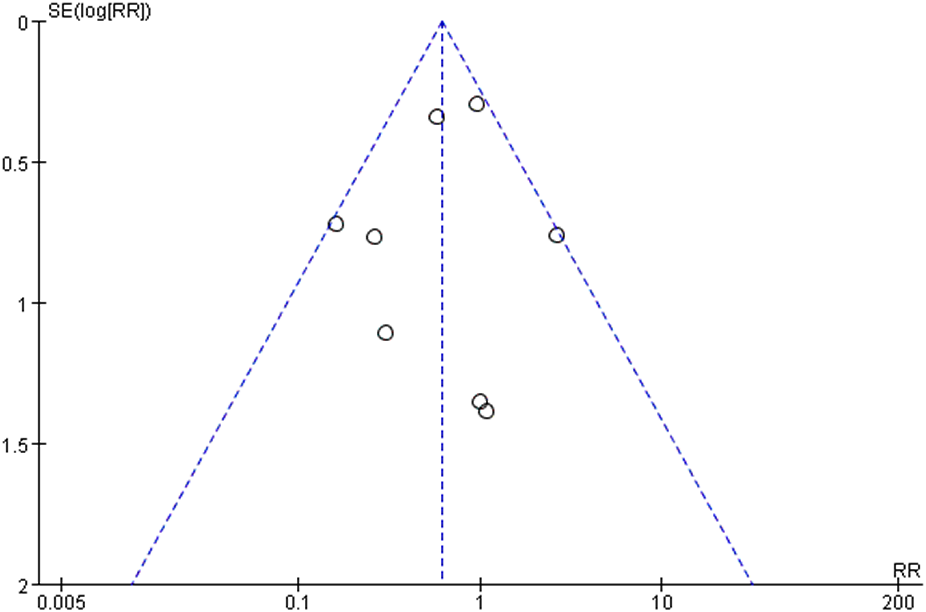
Funnel plot of data on unplanned reoperation between the suture button and syndesmotic screw groups. RR, risk ratio.
Discussion
Overall, our study results indicated that SB fixation has lower complication rates and equivalent or better functional results than SS fixation. Six outcomes were adopted in our study to evaluate the performance between SB and SS fixation, of which 4 outcomes—AOFAS score (MD, 3.04; 95% CI, 1.77 to 4.31), OMAS (MD, 4.51; 95% CI, 1.54 to 7.48), complications (RR, 0.42; 95% CI, 0.26 to 0.66), and unplanned reoperation (RR, 0.62; 95% CI, 0.43 to 0.89)—indicated advantages for the SB group over the SS group. For the remaining outcomes, the EQ-5D score (MD, 0.01; 95% CI, –0.01 to 0.03) and malreduction (RR, –0.06; 95% CI, –0.18 to 0.07) were similar between the SB and SS groups.
Our primary outcomes consisted of malreduction, unplanned reoperation, and complications. After analyzing 5 studies, 18,20,29,30,32 we found that the SB group had similar results for malreduction to the SS group, with the heterogeneity being a little higher (I 2 = 52%; P = .08) than the acceptable standard (I 2 ≤ 50%; P > .1). Two previously published meta-analyses 34,40 also reported the pooled results of malreduction, with their results showing that the SB group had a significantly lower rate in malreduction (odds ratio [OR], 0.4; 95% CI, 0.21-0.76 for Xu et al 40 ; RR, 0.15; 95% CI, 0.04-0.56 for Shimozono et al 34 ). After the comparison, the most evident difference we found was that these author groups included 2 articles that we did not, because we thought those studies failed to meet our eligibility criteria for malreduction. Laflamme et al 19 reported on loss of reduction as evaluated by lateral tibiofibular clear space with a normal value of <6 mm. Colcuc et al 6 reported that no postoperative malreduction occurred.
Unplanned reoperation is important in the aspects of patient satisfaction and cost-effectiveness. Our result also favors the SB group. Most patients underwent surgery due to local irritation of the screw; we thus included more RCTs than other published articles 9,27 to obtain more precise results. Moreover, Ramsey and Friess 31 investigated the cost-effectiveness of SS versus SB fixation. In terms of the health care system, they used a decision-tree model to examine the outcomes of syndesmosis repair surgery and found that the screw removal rate (SRR) and the number of devices applied had an impact on cost-effectiveness, with the SB being more cost-effective when the SRR was ≥17.5%, whereas the SS was more cost-effective when the SRR was ≤13.7%.
As for complications, we observed that the SS group demonstrated significantly more complications than the SB group. We analyzed 3 types of complication (local irritation, implant failure, and infection), of which only local irritation showed a significant difference between the groups, which is why the total effect favored the SB group. Local irritation might be an innate disadvantage for the screws, according to the literature 10,27 ; it is often caused by the prominence of the screw head due to a lack of soft tissues around the surgery site. The SB was well-designed and there were some surgical modifications to help reduce local irritation caused by the SB. 11,26 Therefore, as mentioned above, many patients underwent unplanned reoperations, which caused significant complications.
The AOFAS, OMAS, and EQ-5D results were extracted as secondary outcomes. Some studies also reported range of motion 5,18,19,29,30 and Manchester Oxford Foot Questionnaire 30 and Foot and Ankle Disability Index results, 6,32 but these data were not pooled because of limited related studies and different measuring methods. These functional scales are commonly adopted to assess ankle function.
In our research, the SB group had a significantly higher AOFAS score than the SS group at the 3- to 12-month follow-up periods after surgery, which may be attributed to the reported advantages, such as allowing physiological movement, earlier rehabilitation, earlier weightbearing, and earlier return to sports. 18,19 The AOFAS score, however, was similar at the 24-month follow-up. According to other published meta-analyses, 24 months was the longest follow-up period pooled. Nevertheless, we pooled the data AOFAS scores for 60 months, and they showed significant improvement in the SB group. The results varied in different studies. Xu et al 40 found a significant difference only at 3 months and 24 months. The other 2 studies 27,34 only analyzed the results at 12 months and were accompanied by high heterogeneity (I 2 = 86% and 82%, respectively). At the 12-month follow-up, the SB group showed significant improvement in OMAS; most articles showed similar results in this regard. Interestingly, 1 study 27 misused the original data and indicated nonsignificant differences, although the result was actually significantly different after recalculation. The EQ-5D can be used for assessing pain, activities, anxiety, and depression, which showed similar results between the 2 groups. Moreover, the overall higher functional scores are also supported by an experimental biomechanical study, 1 which indicated that the SB technique could produce better physiologic micromotion of the tibiofibular joint.
Limitations
Our study has several limitations. First, performance and detection bias remained unclear or at high risk among the included RCTs, which may have affected the results of the functional scores. Second, the number of SSs and the number of cortices penetrated were not consistent, and we did not study these variables in our study. Third, 2 outcomes (OMAS and malreduction) showed a slightly higher heterogeneity, which might be due to different surgical methods, fracture types, and varying radiological evaluation methods. It is worth mentioning, however, that there are various fracture patterns, and their treatments also vary, which may affect postoperative outcomes. To provide more precise data, future RCTs could break down their results by fracture type.
Conclusion
Our results showed there were no significant differences between the SB group and the SS group in malreduction and EQ-5D scores. However, compared with SS fixation, SB fixation demonstrated a statistically lower local irritation rate and unplanned reoperation rate, and the functional AOFAS score and OMAS were improved.
Footnotes
Final revision submitted May 10, 2022; accepted August 2, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: Support for this study was received from the Innovation Group of Sports Injury Repair and Reconstruction (cstc2020jcyj-cxttX0004), the Innovation Team of Sports Injury Repair and Reconstruction (41CZDH), and the National Science Foundation for Young Scientists of China (grant No. 81601943). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.