
Abstract
Background:
Femoroacetabular impingement (FAI) is primarily caused by bony impingement between the acetabulum and femoral neck during hip motion. Increasing posterior pelvic tilt improves hip range of motion in patients with FAI.
Purpose:
To use computer simulation analysis to compare the effects of 3-dimensional (3D) changes in pelvic tilt (sagittal tilt [St], axial rotation, and coronal tilt) with changes in a single plane (St), with the aim of improving range of motion in patients with FAI.
Study Design:
Controlled laboratory study.
Methods:
We evaluated 43 patients with FAI treated by arthroscopic cam resection. A 3D simulation was used to construct the following pelvic models: a 5° and 10° increase posteriorly in St (St5° and St10°) and a combined 5° change in St, axial rotation, and coronal tilt (Complex5°) from the baseline of the anterior pelvic plane. Improvements in maximum internal rotation (MIR) at 45°, 70°, and 90° of hip flexion and improvements in maximum flexion with no internal rotation were compared among the St5°, St10°, and Complex5° models. The pelvic models of each single-plane change of 5° and 10° were evaluated in the same simulation.
Results:
At 90° and 70°, there was a significant difference between the Complex5° and St10° models with respect to improvement in MIR (P = .004 at 90° of flexion; P = .017 at 70° of flexion). There was no significant difference in MIR at 45° of flexion (P = .71) or in maximum flexion (P = .42).
Conclusion:
At 70° and 90° of hip flexion, a combined change in 3D pelvic alignment of 5° (ie, St, axial rotation, and coronal tilt) was more effective in improving hip MIR than a 10° change in St only.
Clinical Relevance:
Effective physical therapy for FAI should address pelvic motion in all 3 planes rather than in a single plane.
Femoroacetabular impingement (FAI) is a bony impingement between the acetabulum and femoral neck during hip motion, particularly flexion and internal rotation, which is the anterior impingement position. Repeated mechanical interference results in labral tears, chondral damage, and ultimately osteoarthritis in some patients. 11,17 One of the primary goals of treatment is to avoid/prevent bony impingement. In this regard, arthroscopic cam resection and labral repair can resolve the bony impingement directly, with favorable outcomes at least in midterm follow-up. 25,28,32 Yet, we must consider the possibility of nonoperative treatment, mainly physical therapy, before surgical treatment. Indeed, some evidence shows that physical therapy is effective to avoid surgery for FAI. 9,12,13,40 For instance, trunk stabilization exercises improve clinical outcomes for FAI. 2 Similarly, changing pelvic position suitably may contribute to resolution of FAI 16,27 ; however, it is difficult to measure mobility, particularly in 3 dimensions.
A previous study showed that computer simulation can be used to examine the effect of changes in pelvic tilt on FAI. 33 In addition, a change in posterior sagittal pelvic tilt of 10° is as effective at improving range of motion (ROM) as cam resection, at least in a computer simulation setting. 16 However, in such cases, a large change in tilt in only a single plane (ie, the sagittal plane in the case of posterior tilt) may be limited and unnatural in terms of pelvic anatomic mobility. 41 It may be difficult to change the pelvic tilt by 10° through physical therapy alone. With respect to the pelvis and lower lumbar spine, mobility in all 3 dimensions should be considered. 31
The clinical question arising here was “Should physical therapy that considers 3-dimensional (3D) complex mobility rather than just sagittal mobility be performed in patients with FAI?” The purpose of this study was to use simulation analysis to examine and compare the effect of 3D changes versus a single-plane change (ie, sagittal tilt [St]) in pelvic movement on hip ROM in patients with FAI. Because the effect of sagittal posterior tilt on improving hip ROM has been well demonstrated, 16,33,37 we focused on the comparison between complex 3D change and sagittal posterior tilt change. We hypothesized that the combination of 3D planar mobility (ie, St, axial rotation [Ar], and coronal tilt [Ct]) would lead to more effective resolution of biomechanical impingement, with small changes (5°) in 3D motion rather than a large change (10°) in a single direction (ie, sagittal).
Methods
Study Population
The protocol for this study was approved by our institutional review board. We reviewed 149 consecutive patients (154 hips) treated with arthroscopic cam resection surgery for FAI. All procedures occurred between April 2014 and December 2020 and were performed by 1 of 2 surgeons (N.K. and Y.Y.). A total of 111 hips were excluded: 10 had no available preoperative computed tomography (CT) data; 11 had a history of surgery on the same joint (ie, osteotomy, total hip arthroplasty, or primary arthroscopic surgery); and 90 had concomitant pathologies (ie, osteoarthritis, osteonecrosis, borderline dysplasia, synovial osteochondromatosis, or a labral tear after trauma) and had undergone hip arthroscopy for a diagnosis other than FAI. A total of 43 cases met our final inclusion criteria (36 male and 7 female; mean age, 39 years; range, 14-64 years) (Figure 1).

Flowchart of patient exclusion and inclusion criteria. CT, computed tomography; FAI, femoroacetabular impingement.
The following radiographic and CT definitions of FAI were used: pincer-type FAI was defined as a lateral center-edge angle (LCEA) ≥40° on the anteroposterior pelvic view or ≥25° on the anteroposterior pelvic view and acetabulum retroversion on axial CT scan; cam-type FAI was defined as an LCEA ≥25° on the anteroposterior pelvic view and an alpha angle ≥55° on the Dunn 45° view (flexion, 45° and external rotation, 45°) or cross-table lateral view 20 ; and combined-type FAI was defined as the presence of pincer and cam deformities. Hips with an LCEA of 20° to 25° were excluded as having borderline dysplasia.
Of the 43 included hips, there were 37 with cam-type FAI and 6 with combined-type FAI. All cam-type hips and 4 combined-type hips underwent arthroscopic labral repair on the pelvic side and cam resection on the femoral side. The other 2 combined-type hips underwent additional arthroscopic pincer resection on the pelvic side.
Measurements From Computer Simulations
A 3D dynamic computer simulation analysis was performed using Zed Hip 14.0.0 software (LEXI Co, Ltd). In this software, the hip joint could be moved arbitrarily until the acetabulum and femur came into contact, and ROM simulation automatically stopped at the point of bony contact. First, segmentation and reconstruction of 3D bone models of the pelvis and femur were constructed from CT data in Digital Imaging and Communications in Medicine format.
In this study, the anterior pelvic plane (APP), defined by the 2 anterosuperior iliac spines and the pubic symphysis, was used as the baseline pelvic plane to simplify the assessment of the FAI mechanism. For the femoral plane, reference points around the femoral head on the axial and sagittal planes were used to define the femoral head center. The axis was set using 2 reference points: the head center and the midpoint between the medial and lateral epicondyles. The axis was matched to the APP in the sagittal plane as the position of the femur at baseline. Next, a coordinate system was reconstructed in which the pelvis was virtually changed with respect to the baseline APP as follows: 5° tilt in the sagittal plane (St5°), 10° tilt in the sagittal plane (St10°), 5° rotation in the axial plane (Ar5°), 10° rotation in the axial plane (Ar10°), 5° tilt in the coronal plane (Ct5°), 10° tilt in the coronal plane (Ct10°), and combined St5° + Ar5° + Ct5° (Complex5°). In this study, an St of the pelvis was defined as a posterior tilt in the sagittal plane; an Ar of the pelvis was defined as an internal rotation relative to the femur of the symptomatic side in the axial plane; and a Ct was defined as upward tilt relative to the femur of the symptomatic side in the coronal plane (Figure 2).

Representative images from the virtual pelvic tilt model: right side. (A) The anterior pelvic plane was used as the baseline (yellow lines), with the anterosuperior iliac spine and pubic joint as reference points. (B) A 10° sagittal tilt (St10°) and (C) a combined 5° St, axial rotation, and coronal tilt (Complex5°) were defined relative to the baseline plane.
Maximum flexion (MF) and maximum internal rotation (MIR) causing impingement automatically in the simulation at 45°, 70°, and 90° of flexion were evaluated for each pelvic position and compared with the improvement in angle from the baseline simulation (St5° vs St10° vs Complex5°, St5° vs Ar5° vs Ct5°, and St10° vs Ar10° vs Ct10°). A distinction was made between angle and ROM in that angle refers to the degree of pelvic tilt and ROM refers to the amount of hip joint movement in a certain position.
Statistical Analysis
The improvements in MF and MIR were analyzed first using the paired Student t test; then, the Bonferroni test for multiple comparisons was used to assess the mean improvement in MF and MIR at 45°, 70°, and 90° of flexion in the St5°, St10°, and Complex5° groups. The differences in improvement in MF and MIR at each flexion angle in each single-dimensional change (St, Ar, and Ct) of 5° or 10° were also assessed using the paired Student t test and the Bonferroni test. P < .05 was considered statistically significant. All statistical analyses were performed using JMP PRO 15.0.0 software (SAS Institute Inc).
A post hoc power analysis with an effect size of 0.5 was performed as described by Cohen 6 ; the inclusion of 43 hips indicated a power of 0.74 with α = .05, which was considered a suitable sample size. The posterior power was calculated using G*Power, Version 3.1.9.6. 10
Results
The demographic characteristics of the study patients are shown in Table 1.
Patient Characteristics (N = 43) a

a Data are reported as mean ± SD unless otherwise indicated. APP, anterior pelvic plane; FPP, functional pelvic plane.
Under all conditions, there were no patients with impingement before 90° of flexion. Regarding MIR, at 90° of flexion there was a significant difference between the Complex5° and St10° groups (9.60° ± 3.7° vs 6.65° ± 4.4°; P = .004). At 70° of flexion, we also found a significant difference between the Complex5° and St10° groups (11.5° ± 4.2° vs 8.23° ± 6.3°; P = .017). However, there was no significant difference in MIR at 45° of flexion between Complex5° and St10° (13.8 ± 6.2° vs 12.0° ± 7.6°; P = .71) and no significant difference in MF between Complex5° and St10° (8.67° ± 7.4° vs 10.4° ± 2.3°; P = .42). Improvement in mean ROM was greater in the Complex5° model versus the St10° model. In all positions, improvement in the St5° group was inferior when compared with the other groups. Figure 3 shows improvements in MF and MIR at 45°, 70°, and 90° of flexion among the St5°, St10°, and Complex5° groups.
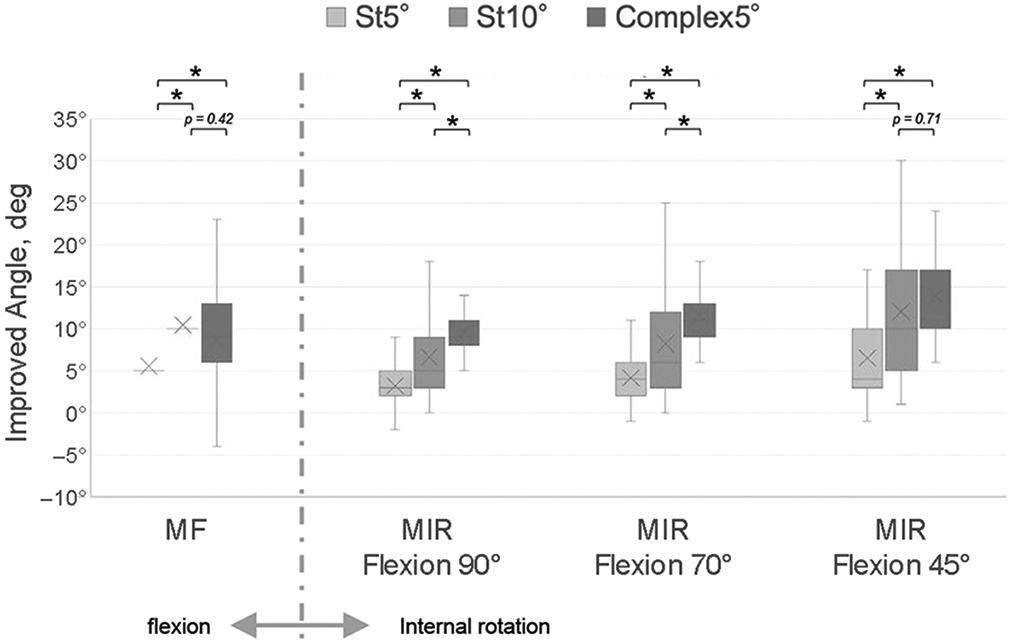
Effect of St5°, St10°, and Complex5° models in improving the MF and MIR angles at 45°, 70°, and 90° of flexion. For MIR at 90° and 70° of flexion, the improvement shown in Complex5° was significantly (3°) higher when compared with St10°. However, there was no significant difference in MF and MIR at 45° of flexion. In all positions, there was a significant difference between the Complex5° and St5° models and between the St10° and St5° models. Shaded boxes, interquartile range; middle line, median; ×, mean; whiskers, range. *Statistically significant difference (P < .05). Complex5°, combined 5° sagittal tilt, axial rotation, and coronal tilt; MF, maximum flexion; MIR, maximum internal rotation; St, sagittal tilt.
The same ROM simulation was performed for each single-plane change of 5° and 10°. With respect to MIR at 90° of flexion, there were significant differences among the 3 pelvic planes of 5° and 10° (P < .05). The improved angle decreased as the flexion angle increased with changes in Ar and St. Yet, the improved angle increased as the flexion angle increased with change in Ct. Figure 4 shows the results of comparing single-plane changes among groups.

The effect of each single-plane change in pelvic tilt of 5° and 10° at different positions of the femur. There were different effects among the 3 pelvic planes. Shaded boxes, interquartile range; middle line, median; ×, mean; whiskers, range. *Statistically significant difference (P < .05). Ar, axial rotation; Ct, coronal tilt; MF, maximum flexion; MIR, maximum internal rotation; St, sagittal tilt.
In these simulations, we observed various influences on improvements in ROM, depending on which pelvic plane was changed. Figure 5 shows a representative case of cam-type FAI.
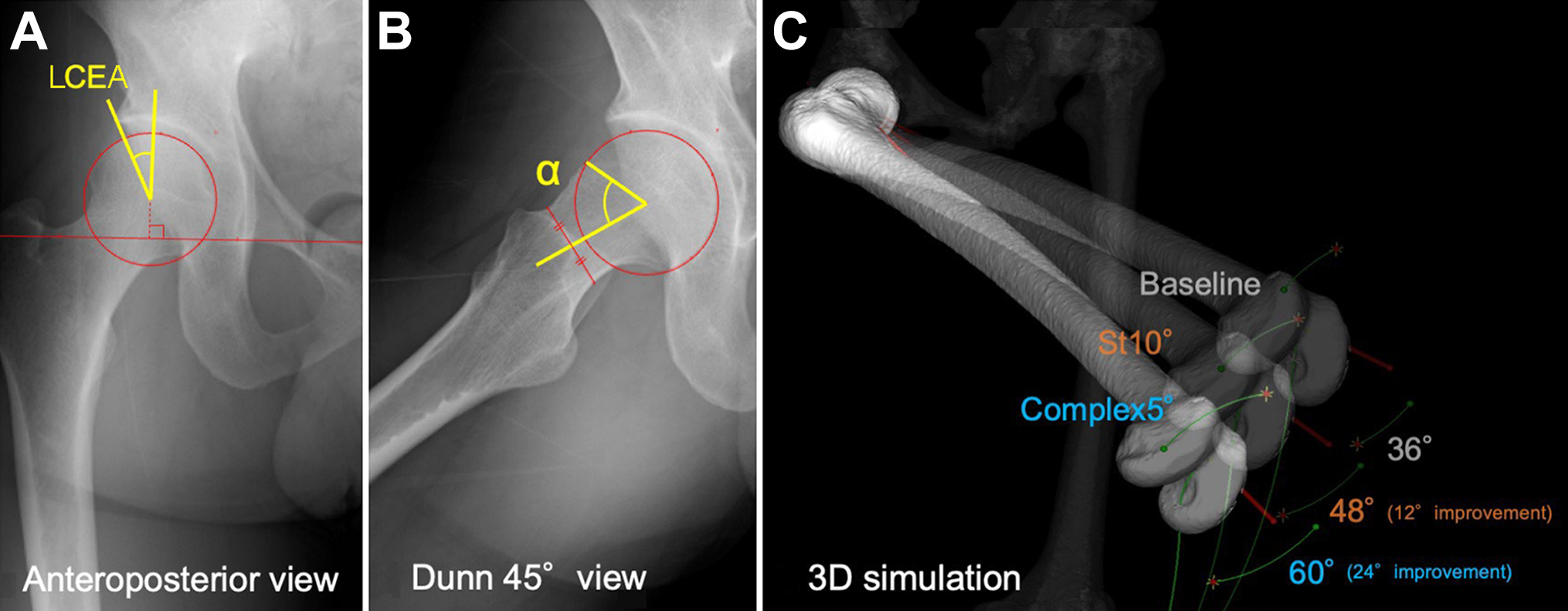
A representative case of cam-type femoroacetabular impingement. (A) Anteroposterior pelvic view. The lateral center-edge angle (LCEA) was 30°. (B) Dunn 45° view (flexion, 45° and external rotation, 45°). The alpha angle (α) was 68°. (C) Maximum internal rotation at 90° of flexion. The 3 patterns of the pelvis (baseline, St10°, Complex5°) are superimposed to make it easier to visually understand the difference in maximum internal rotation. The Complex5° model resulted in a 24° improvement over baseline and a 12° improvement over St10°. Complex5°, combined 5° St, axial rotation, and coronal tilt; St, sagittal tilt. 3D, 3-dimensional.
Discussion
The findings of the current study indicated that a combination of pelvic mobility in 3 planes improves hip ROM in simulation with an FAI model. Although there was no significant difference in MF and MIR at 45° of flexion, changing 3D pelvic mobility by 5° in 3 planes was more effective at increasing MIR at 70° and 90° of flexion than changing it by 10° in just St. The clinical implications of this finding are that we should try to improve 3D complex pelvic mobility in cases of FAI rather than movement only in the sagittal plane (ie, posterior St).
To date, studies of FAI have focused on the relationship between ROM and pelvic tilt in the sagittal plane. A computer simulation analysis of FAI by Ross et al 33 showed that dynamic anterior pelvic tilt caused earlier occurrence of anterior impingement in the arc of motion, whereas dynamic posterior pelvic tilt caused later occurrence. Also, Swärd Aminoff et al 37 showed that there was a significant increase in internal hip rotation when the participants sat with a flexed posture with maximum posterior pelvic tilt.
Specifically, Ross et al 33 demonstrated that 10° of posterior pelvic tilt increased MIR at 90° of flexion by about 5° (32.0° to 37.1°; P < .0001) and that 10° of anterior pelvic tilt reduced MIR at 90° of flexion by about 6° (32.0° to 26.1°; P < .0001). Given these results, we examined the effects of a 10° change in pelvic tilt. In a previous study, we conducted a dynamic simulation analysis to compare improvements in ROM (ie, MIR) between cam resection models and models of a 10° change in St. 16 Cam resection models were based on postoperative CT scans (cam resection surgery). We showed that a change in posterior St of 10° was as effective as cam resection at reducing impingement; however, a change of only 5° was not as effective as cam resection. Based on this, our current results possibly indicate that 3D changes in pelvic alignment would lead to favorable outcomes in improving ROM as much as cam resection, even if the change in each plane is small. Because the focus of this study was to compare the effect between the 3D complex state and posterior St that was well reported in previous studies, Ar and Ct were not compared with the complex state. Data regarding 3D mobility of the pelvis in healthy participants during activity should be collected and assessed. Indeed, pelvic rotation during walking is limited in FAI cases as compared with healthy ones. 30
In most femoral positions, pelvic changes in St were more influential than changes in Ar (Figure 4). In MIR at 90° of flexion, Ct in the frontal plane had the most influence among the 3 pelvic planes. Based on these results, changes in a single dimension had different effects on ROM at different femoral positions. Because there is a difference in the center of rotation between the pelvis and femur, it is not possible to find a 1:1 change of angle between pelvis and femur in the same plane (ie, Ar5° does not always improve internal rotation at 5°). A previous study suggested that MIR impingement in FAI with cam morphology may be more common at 70° of flexion than at 90°. 23 We often need to flex the hip joint by >90°, for example, when standing up from the floor or a chair and putting on/taking off shoes. 14
Thus, the hip joint must adopt different positions during occupational or sporting activities. To avoid pain or impingement, we tend to adopt the best pelvic position automatically. 3,9 Sporting activities require a range of hip mobility, particularly impact sports such as basketball, ice hockey, and soccer. Athletes competing in these sports report high rates of groin pain and are at increased risk of a cam deformity 1,15,19,29,35,36 owing to the large flexion, adduction, abduction, and internal rotation angles required for sports. 21,39 Depending on the type of sporting activity, St, Ar, or Ct of the pelvis may be different and have differing effects on the hip joint. For instance, the grand battement dance movements (eg, devant, à la seconde, derrière) require a variety of 3D pelvic movements. 5
In terms of physical therapy, feasible methods to improve pelvic mobility in 3 planes need to be developed, as suggested by our computer simulation. A previous study showed an 11.5° increase in anterior pelvic tilt when sitting with the pelvis forward maximally and arching the lumbar spine and a 10.5° increase in posterior pelvic tilt when sitting with the pelvis backward maximally and flexing the lumbar spine when compared with a neutral posture. 37 Also, the anterior pelvic tilt decreased significantly from 10° ± 2° to 3° ± 1° (approximately 7°) in prone hip extension with an abdominal drawing-in maneuver. 22 Moreover, the angle of anterior pelvic tilt improved by around 4° during active prone knee flexion after a motor control exercise using an abdominal drawing-in maneuver. 26 Thus, changes in posterior pelvic tilt of least around 5° may be feasible in the clinic. Yet, the clinical relevance of an ∼3° difference of improvement in MIR has not been verified, although there was a statistically significant difference. We believe that a change of 5° in multiple planes may be more realistic than a change of 10° in a single plane and that the changes in multiple planes may improve hip ROM in FAI. 24
Diamond et al 8 suggested that patients with FAI exhibit greater pelvic Ct (∼3°) on the symptomatic side in the frontal plane during step ascent than healthy controls. The authors also found that 5/6 symptomatic FAI patients rose the pelvis >7° on the FAI side in the frontal plane during the single leg support phase of step ascent. Moreover, they reported that individuals with FAI placed the hip in a 5° more adducted/less abducted position in the coronal plane during the contact phase of walking, although there were no alterations in the sagittal or axial plane. These changes in pelvic rise and femoral adduction in the frontal plane make sense from the perspective of avoiding pain and impingement in the frontal plane. 4 Thus, it is important to combine several kinds of exercise, with the intention of increasing 3D pelvic mobility. For instance, a combination of transverse abdominis exercises 38 and lateral tilt trunk-leaning exercises 18 might be effective in obtaining more coordinated 3D pelvic mobility. We may also need to consider the effect of pelvic tilt on hamstrings and quadriceps. 7 Regarding the influence of the contralateral hip, the pelvic motion for the one side certainly makes an opposite effect for the other side. Yet, it is rare in activities of daily living to move both hips in the same direction at the same time. Therefore, the influence of 3D pelvic motion for the contralateral hip was not assessed in this study.
Limitations
This study has several limitations. First and foremost, the 3D pelvic adaptations are only theoretical and may not be generalizable because many of these adaptations were dynamic and this study examined pelvic tilt as a static entity. A fundamental limitation of CT-based simulation is that it does not consider the influence of soft tissues, including the joint capsule and labrum; in addition, the difference in pelvic tilt between the supine and standing positions was not considered because all CT scans were taken in the supine position. During standing, the posterior pelvic tilt is greater than that in the supine position, although there is a marked difference among individuals. 34 Therefore, to reduce the influence of individual differences as far as possible, we used the APP as the baseline setting.
Conclusion
A combined change in 3D pelvic alignment of 5° (ie, St, Ar, and Ct) was more effective in improving hip MIR than a 10° change in St only, at least at 70° and 90° of hip flexion in computer simulation.
Footnotes
Acknowledgment
The authors are grateful to Haruna Kitayama for creating part of the 3D bone model.
Final revision submitted June 20, 2022; accepted July 6, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Yokohama City University.