
Abstract
Background:
Although the minimal invasiveness of arthroscopic ankle lateral ligament repair (ALLR) means that an early return to sporting activities can be anticipated, studies have described postoperative cast immobilization and the avoidance of weightbearing for a certain period. Accelerated rehabilitation may be helpful for an early return to sport.
Purpose:
To investigate clinical outcomes of ALLR and accelerated rehabilitation with a minimum duration of postoperative ankle immobilization and proactive early weightbearing.
Study Design:
Case series; Level of evidence, 4.
Methods:
This study investigated 23 ankles of 22 patients (11 men, 11 women; mean age, 38.7 years) who underwent ALLR for chronic lateral ankle instability. Postoperative management included the avoidance of weightbearing until postoperative day 3, after which full weightbearing walking with a brace was permitted. The objective was to return to competitive sport 8 weeks after surgery. The following were evaluated: pre- and postoperative instability and pain symptoms, ankle range of motion, anterior drawer distance on stress radiograph, anterior translation measured with a capacitance-type strain sensor, the Ankle-Hindfoot Scale from the Japanese Society for Surgery of the Foot, and the SAFE-Q (Self-Administered Foot Evaluation Questionnaire).
Results:
Two male patients dropped out and were excluded from analysis. Postoperatively, instability and pain resolved or improved in all patients. There was no significant postoperative change in range of motion. There were significant pre- to postoperative improvements in talar tilt angle (from 12.2°-5.6°, P < .01), anterior drawer distance (8.2-4.4 mm, P < .01), and anterior translation (10.5-4.6 mm, P < .01) as well as the Ankle-Hindfoot Scale score (68.8-96.8, P < .01) and all subscales of the SAFE-Q (P ≤ .01 for all). Complete return to sport was achieved by 75% of the patients at 8 weeks postoperatively.
Conclusion:
When accelerated rehabilitation with proactive weightbearing exercises was implemented from postoperative day 3 without ankle immobilization after ALLR, there were significant improvements in objective assessments of ankle stability and clinical scores, and as many as 75% of the patients were able to make a complete return to sport within 8 weeks.
Keywords
An ankle sprain is one of the most common injuries in athletes, typically involving the lateral ankle ligaments. 6,15,19,32 In most cases, lateral ankle ligament injuries respond well to nonoperative therapies such as external immobilization and physical therapy, which provide satisfactory therapeutic outcomes. 11,14 However, approximately 20% of patients develop chronic lateral ankle instability (CLAI), leading to repeated sprains and, in some cases, the development of osteoarthritis. 7,9,17,21,25,30 Surgical treatment is indicated for athletes whose performance is adversely affected by CLAI and patients who experience severe instability in the conduct of daily activities. Anatomic open repair of the anterior talofibular ligament (ATFL) has long been the standard procedure, 4 but the recent development of effective devices and increasing demand for minimally invasive surgery have led to the more frequent use of arthroscopic ankle lateral ligament repair (ALLR). Biomechanical studies using cadavers have demonstrated that adequate repair can be achieved by arthroscopic surgery, with no difference between ALLR and traditional open repair in terms of the strength of the repaired ligament. 8 Stable clinical results for ALLR have been reported, with good clinical scores and few complications. 1,2,5,18,20,28,31
Although the minimally invasive nature of ALLR means that an early return to daily life or sporting activities can be anticipated, many reports have described postoperative cast immobilization and nonweightbearing for a certain period. 13 However, accelerated rehabilitation (AR) that minimizes the duration of postoperative ankle immobilization and actively implements early weightbearing exercises may be effective in enabling athletes who have undergone surgery to make an early return to sport. The effect of early weightbearing and range of motion (ROM) exercises on the healing process after ankle ligament repair remains unknown. Since early weightbearing exercises after ankle sprain have been reported to exert a beneficial impact on improving ankle function, 3 AR after ALLR may also have a good clinical effect.
The purpose of this study was to investigate the therapeutic outcomes of ALLR with AR, including the minimum duration of postoperative ankle immobilization and proactive early weightbearing. We hypothesized that ALLR in combination with AR would improve objective ankle stability and clinical scores and enable an early return to competitive sport.
Methods
The protocol for this study was approved by our hospital’s institutional review board. We reviewed the records of 22 patients (23 ankles) who underwent ALLR at our institution for CLAI. Consecutive patients who visited our hospital between 2017 and 2020 were included. The patients were 11 men and 11 women with a mean age of 38.7 years (range, 16-61 years). Their mean height was 166.0 cm (range, 157-186 cm), mean weight was 69.2 kg (range, 52-110 kg), and mean body mass index was 24.9 kg/m2 (range, 18.7-38.1 kg/m2). CLAI was diagnosed and surgery indicated if 4 criteria were met: (1) previous ankle sprain and chief complaint of instability, (2) laxity confirmed by manual investigation or stress radiographs, (3) persistent instability to ≥3 months of nonoperative therapy, and (4) presence of the ATFL on ultrasonography or magnetic resonance imaging. Patients were excluded if they had previously undergone ankle surgery, had a concomitant fracture, had inflammatory joint disease or connective tissue disease, and did not have at least 12 months of follow-up data.
ALLR Procedure and AR Protocol
Surgery was conducted with the patient in the supine position using a thigh tourniquet. Traction was applied with a thigh holder and a noninvasive ankle joint distractor. An ankle arthroscope (2.7-mm diameter) was inserted via a medial midline portal or an anteromedial portal. The medial midline portal was created at the talocrural joint level just lateral to the tibialis anterior tendon. An accessory anterolateral portal was also created as a working portal. This accessory anterolateral portal was created approximately 1 cm anterior to the lateral malleolus, with the proximal margin of the ATFL as its target. Synovectomy was conducted around the ATFL to secure the field of vision, after which the drill guide for a DEX FiberTak anchor (Arthrex) was placed against the proximal fibular obscure tubercle via the accessory anterolateral portal, and drilling was performed. An all-suture anchor, including nonabsorbable suture tape (1.3 mm wide) as the anchor thread, was inserted into the drill hole. After a microsuture lasso was inserted percutaneously into the confluent fibers of the ATFL and the calcaneofibular ligament according to the method of Kanzaki et al, 13 a suture relay was performed, and the suture anchor was passed through the remaining ATFL tissue and the articular capsule together. The traction was released, and the suture anchor was tied off 4 times with the ankle dorsiflexed and everted (Figure 1).

Surgical procedure for the right ankle joint. (A) The anchor drill guide is placed on the proximal fibular obscure tubercle via the accessory anterolateral portal, and drilling is conducted (inset: arthroscopic view). (B) All-suture anchor insertion. (C) Percutaneous insertion of a microsuture lasso into the confluent fibers of the anterior talofibular ligament (ATFL) and the calcaneofibular ligament (inset: arthroscopic view). (D) Suture relay is performed, and the suture anchor is passed through the remaining ATFL tissue and the articular capsule together. (E) The suture anchor is tied off, and the ATFL is tightened.
Postoperative management included the avoidance of weightbearing until postoperative day 3 to prevent swelling, with the ankle immobilized in the neutral position with a fiberglass back slab. From day 3 on, full weightbearing walking with a brace was permitted, and the ankle was immobilized with a fiberglass back slab only at night to prevent plantarflexion. The brace was constructed of neoprene, allowing dorsi- and plantarflexion of the ankle, but with plastic supports on the medial and lateral sides, thus limiting inversion and eversion (Figure 2).

Walking brace.
The splint was an L-shaped glass fiber material that was removable. The night splints were worn for 3 weeks after surgery. Up to 3 weeks after the operation, walking, squats, training of the intrinsic muscles of the foot, and dorsiflexion of the ankle were performed. At 3 to 4 weeks, plantarflexion of the ankle was allowed, and dorsi- and plantarflexion strengthening exercises were commenced. Patients were allowed to start jogging at 4 weeks and specific training for competitive sport at 6 weeks, with the goal of returning to competitive sport at 8 weeks after surgery. Before allowing the athlete to return to sports, we confirmed that laxity and pain disappeared, there was no ROM limitation, sufficient strength and balance were obtained, and the competition-specific movements were fully gained.
Outcome Measures and Statistical Analysis
Instability and pain were measured pre- and 12 months postoperatively, and postoperative ankle ROM was evaluated using a goniometer. As objective assessments of ankle stability, the pre- and postoperative anterior drawer distance and talar tilt angle were measured on stress radiographs (Figure 3), and anterior translation (AT) was measured by a capacitance-type strain sensor. 29
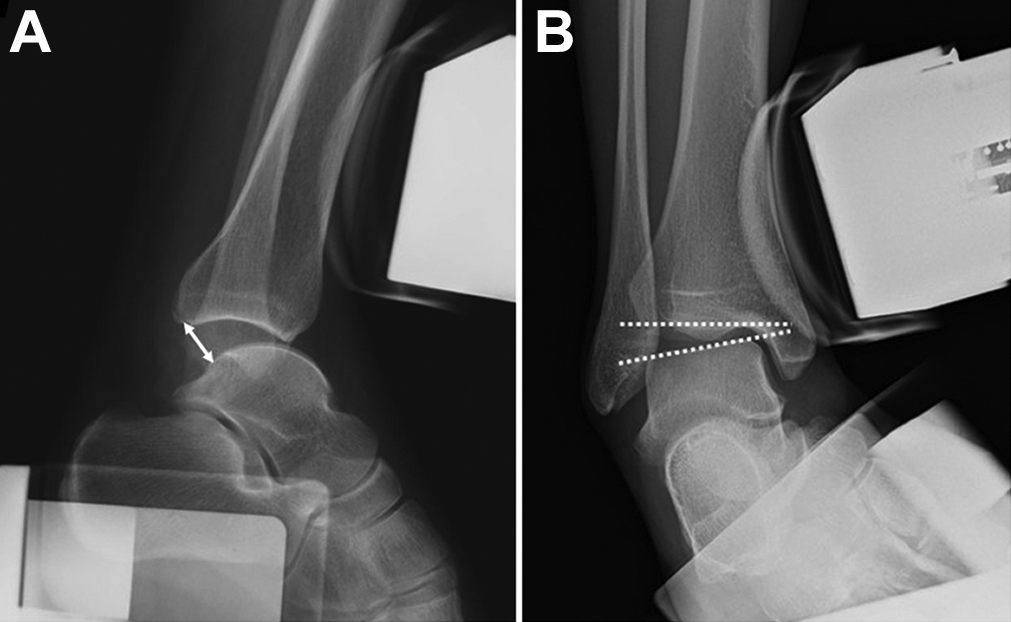
Measurement of the (A) anterior drawer distance (double-sided arrow) and (B) talar tile angle (dotted lines) on radiograph.
As an objective clinical score, patients completed the Japanese Society for Surgery of the Foot (JSSF) Ankle-Hindfoot Scale pre- and postoperatively. The JSSF scale has a maximum score of 100 points (40 points for pain, 50 for function, and 10 for alignment). As a subjective patient assessment, pre- and postoperative scores on the Self-Administered Foot Evaluation Questionnaire (SAFE-Q) were evaluated. The SAFE-Q consists of 34 questions divided among 5 subscales: Pain and Pain Related, Physical Functioning and Daily Living, Social Functioning, Shoe Related, and General Health and Well-being. It has 9 additional questions on sporting activity. These are each scored out of a possible high score of 100 points. 22,23 Finally, we evaluated whether patients had been able to return to sport at 8 weeks after surgery.
All outcome data were compared preoperatively and at a minimum 12 months postoperatively using a paired t test. P < .05 was regarded as significant. All data analysis was performed using Excel (Microsoft).
Results
Two male patients dropped out of the study 2 months after surgery; thus, the analysis population comprised 21 ankles from 20 patients with a minimum follow-up of 12 months. The mean duration of follow-up was 17.1 months (range, 12-26 months), and comorbidities were present in 16 patients (76.2%), including osteoarthritis, osteochondral lesion, loose body, posterior ankle impingement syndrome, and tibialis posterior tenosynovitis. Concurrent surgery was performed in 16 patients (76.2%), including osteophytectomy, synovectomy, microfracture, loose body removal, os trigonum excision, and tenosynovectomy (Table 1).
Comorbidities and Concurrent Procedures (21 Ankles, 20 Patients)

The surgical time ranged from a minimum of 37 minutes to a maximum of 159 minutes, and it was affected by the concurrent surgery. The only complication was residual skin irritation symptoms caused by a knot in 1 patient, which were treated by suture removal in a follow-up operation. In all patients, instability and pain resolved or improved postoperatively (Table 2).
Postoperative Patient Symptoms

There was no significant pre- to postoperative change in ROM. There were significant pre- to postoperative improvements in mean talar tilt angle (from 12.2°-5.6°, P < .01), mean anterior drawer distance on stress radiographs (8.2-4.4 mm, P < .01), and mean AT (10.5-4.6 mm, P < .01). The JSSF score improved significantly from 68.8 to 96.8 (P < .01), and the SAFE-Q score improved significantly on all subscales (Table 3).
Pre- and Postoperative SAFE-Q Subscale Scores a

a Each P value indicates a statistically significant pre- to postoperative difference (P < .05). SAFE-Q, Self-Administered Foot Evaluation Questionnaire.
Eight weeks after the operation, 9 of 12 (75%) patients were able to fully return to sports, and 2 (17%) returned partially. Of the 3 patients who could not fully return in 8 weeks, 2 were able to return to sports in 15 weeks (Table 4).
Sports to Which the Patients Returned (12 Patients)

a Patient underwent wrist surgery.
Discussion
An important finding of this study is that objective assessments of ankle stability and clinical scores improved significantly after ALLR in combination with AR. It was also found that most patients were able to make a complete return to sport within 8 weeks.
ALLR is frequently performed because of its minimally invasive nature and the recent development of numerous specialist arthroscopic devices for use in the ankle. In most cases, ALLR involves repairing the lateral ligament by inserting 1 or 2 suture anchors into the fibula. There is thus concern about the strength of the repair in the immediate postoperative period. In most cases, the ankle is immobilized in a cast for a certain period postoperatively. Kanzaki et al, 13 whose surgical procedure is similar to ours, immobilized the ankle in a cast for 3 weeks with the goal of returning to sport within 3 months after surgery. Jo et al 12 added inferior extensor retinacular reinforcement to ALLR and put patients in nonweightbearing splints for 2 weeks. Results of a prospective randomized study comparing patients who did and did not undergo additional extensor retinacular reinforcement indicated that, 1 year after surgery, the therapeutic outcomes in both groups were good, with no significant difference between them. In another study that used internal brace augmentation, which is believed to further increase the strength of the repair, the patient was put into a plaster shell for 1 week, and weightbearing was avoided. 24 Postoperative immobilization in a cast and avoidance of weightbearing for a certain period after ALLR may help stabilize the ligament repair, but its temporary effects include reduced joint ROM and muscle strength around the ankle, as well as diminished proprioceptive sensory input, potentially delaying athletes’ return to competitive sport. Ideally, proactive postoperative care should be provided that avoids placing the repaired ligament and the anchor under strain.
In a cadaveric study in which a single all-suture anchor was used for the arthroscopic repair of a completely ruptured ATFL, its rupture strength was 27.9 N. 16 Haraguchi et al 10 analyzed computer gait simulations and calculated the load on the ATFL during the gait cycle. They found that the maximum load was 11.3 N at toe-off and that at all other points in the gait cycle, the load on the ATFL was <10 N. This suggests that as long as load bearing in the plantarflexed position can be avoided, the load on the ATFL during normal walking is small. Robotics research using cadavers has shown that the increased load on the ATFL is <10 N as a result of ankle plantar- and dorsiflexion movements. 26 This suggests that early weightbearing exercises implemented after ALLR without cast fixation should not impose a major load on the repaired ligament.
Only a single previous study has investigated the effects of early weightbearing on ankle ligament repair. Takao et al 27 conducted arthroscopic ATFL repair using a modified lasso-loop technique and carried out AR in which patients started walking the day after surgery wearing an elastic bandage. The authors stated that patient-reported subjective assessments were extremely good and that patients were permitted to return to sport 5 weeks after surgery. This may therefore be a useful method of treatment for athletes wishing to make an early return to sport and patients undergoing surgery on both ankles at the same time. In the present study, not only did patient-reported subjective assessments improve, but significant improvements were evident in objective assessments of ankle stability. Objective assessments were made by evaluating stress radiographs as well as AT measured with a capacitance-type strain sensor. 29 Because measurement of AT enables the anterior drawer distance during the manual anterior drawer test to be evaluated quantitatively, it is extremely useful as an objective assessment of stability before and after ALLR.
Limitations
A limitation of this study is its nature as a retrospective case series rather than a comparative study. A comparison with a group who underwent the same procedure followed by immobilization in a cast and the avoidance of weightbearing would provide clearer evidence for the effectiveness of AR in ALLR. Two other issues include the small number of patients and the fact that all of the patients belonged to the same ethnic group, meaning that the effects of physique and similar variables could not be eliminated. Yet, the present data appear to be sufficiently reliable because it was possible to confirm postoperative stability and the absence of recurrence by objective assessments of ankle stability as well as subjective patient-reported assessments. A further limitation is that the patients did not all participate in the same type of sport and that their competitive levels varied. A final limitation is the short duration of postoperative follow-up, from 1 to 2 years. Because the goal of treatment was an early postoperative return to sport, almost all of the athletes achieved this therapeutic goal. However, longer-term follow-up is required to investigate the quality of performance and the incidence of recurrence.
Conclusion
AR following ALLR not only improved instability and pain but also resulted in significant improvements in objective assessments of ankle instability and clinical scores. Patients were able to make an early return to sporting activities, and no case of recurrence was observed, suggesting that arthroscopic ligament repair followed by AR may be an effective treatment method for athletes.
Footnotes
Final revision submitted June 16, 2022; accepted July 6, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by JSPS KAKENHI (grant JP21K09208). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Sapporo Medical University (No. 312-80).