
Abstract
Background:
Despite advances in surgical management of acromioclavicular (AC) joint reconstruction, many patients fail to maintain sustained anatomic reduction postoperatively.
Purpose:
To determine the biomechanical support of the deltoid and trapezius on AC joint stability, focusing on the rotational stability provided by the muscles to posterior and anterior clavicular rotation. A novel technique was attempted to repair the deltoid and trapezius anatomically.
Study Design:
Controlled laboratory study.
Methods:
Twelve human cadaveric shoulders (mean ± SD age, 60.25 ± 10.25 years) underwent servohydraulic testing. Shoulders were randomly assigned to undergo serial defects to either the deltoid or trapezius surrounding the AC joint capsule, followed by a combined deltotrapezial muscle defect. Deltotrapezial defects were repaired with an all-suture anchor using an anatomic technique. The torque (N·m) required to rotate the clavicle 20° anterior and 20° posterior was recorded for the following conditions: intact (native), deltoid defect, trapezius defect, combined deltotrapezial defect, and repair.
Results:
When compared with the native condition, the deltoid defect decreased the torque required to rotate the clavicle 20° posteriorly by 7.1% (P = .206) and 20° anteriorly by 6.1% (P = .002); the trapezial defect decreased the amount of rotational torque posteriorly by 5.3% (P = .079) and anteriorly by 4.9% (P = .032); and the combined deltotrapezial defect decreased the amount of rotational torque posteriorly by 9.9% (P = .002) and anteriorly by 9.4% (P < .001). Anatomic deltotrapezial repair increased posterior rotational torque by 5.3% posteriorly as compared with the combined deltotrapezial defect (P = .001) but failed to increase anterior rotational torque (P > .999). The rotational torque of the repair was significantly lower than the native joint in the posterior (P = .017) and anterior (P < .001) directions.
Conclusion:
This study demonstrated that the deltoid and trapezius play a role in clavicular rotational stabilization. The proposed anatomic repair improved posterior rotational stability but did not improve anterior rotational stability as compared with the combined deltotrapezial defect; however, neither was restored to native stability.
Clinical Relevance:
Traumatic or iatrogenic damage to the deltotrapezial fascia and the inability to restore anatomic deltotrapezial attachments to the acromioclavicular joint may contribute to rotational instability. Limiting damage and improving the repair of these muscles should be a consideration during AC reconstruction.
More than 100 surgical stabilization techniques have been proposed for acromioclavicular (AC) joint injuries without a consensus gold standard. 13 The majority of techniques aim to provide stability by mimicking the AC and coracoclavicular (CC) ligaments, as their role in AC joint stabilization has been demonstrated in numerous biomechanical studies. The AC joint capsule, or AC ligamentous complex (ACLC), provides horizontal stability in the anteroposterior plane, 7,9,14,21 with the posterosuperior bundle serving as the primary restraint, 21 and the CC ligaments provide vertical and horizontal stability. 7,9,14 However, despite a biomechanical understanding of the AC and CC ligaments and advanced anatomic reconstruction procedures, the most common complication of AC joint surgery is the failure to maintain sustained anatomic reduction postoperatively. 2,3,5,24,29
One hypothesis for the failure of sustained anatomic reduction, which biomechanical testing of constructs has failed to address, is the complex in vivo motion of protraction. This motion combines anterior scapular tilt, anterior acromial translation, and internal scapular rotation. Previous reconstructions of the AC and CC ligaments have demonstrated the ability to biomechanically restore translational stability in the superoinferior and anteroposterior planes; however, several studies have identified that rotational stability is more challenging to achieve. 1,10,25
A recent study proposed that the AC joint dynamic stabilizers, the deltoid and trapezius, should be considered during surgical reconstruction for additional joint stabilization. 22 LeVasseur et al 22 performed an anatomic investigation of the relationship between the AC joint and its dynamic stabilizers. In this study, the authors identified that the deltoid is confluent with 90% of the anterior ACLC and that the trapezius is confluent with 70% of the posterior ACLC, demonstrating an intimate relationship between the muscles and the ACLC. Another recent anatomic study identified that the deltotrapezial fascia is strongest along the trapezius and overlaying the AC joint. 6 Although considered important dynamic stabilizers of the joint, the deltoid’s clavicular attachment is often excised during surgical repair and repaired by simply suturing it back to the trapezial fascia above the clavicle. 4 This likely does not take into account the complex anatomy of the muscle’s origin along the clavicle, AC joint capsule, and acromion.
Despite the recent anatomic evaluations of the AC joint dynamic stabilizers, there is a lack of literature investigating the biomechanical significance of the deltoid and trapezius on AC joint stabilization. The purpose of this study was to determine the biomechanical support of the deltoid and trapezius on AC joint stability. The study focused on the rotational stability provided by the muscles to posterior clavicular rotation (simulating protraction) and anterior clavicular rotation (simulation retraction). Additionally, a novel technique to anatomically repair the deltoid and trapezial attachments was attempted, as compared with the traditional nonanatomic technique of suturing the deltotrapezial fascia together above the joint. It was hypothesized that the deltoid and trapezius would provide rotational stability to the AC joint and that the novel repair technique would restore the native joint stability.
Methods
Twelve fresh-frozen human cadaveric shoulder specimens were used for this study (mean ± SD; age, 60.25 ± 10.25 years; bone mass density, 0.748 ± 0.230 g/cm2). Specimens without a medical history of shoulder issues and/or osteoarthritis were obtained from MedCure. This cadaveric study was exempt from institutional review board approval at our institution.
Experimental Design
Sequential dissection of the deltoid and trapezial attachments to the AC capsule and subsequent biomechanical testing were performed to evaluate their contribution to the rotational stability of the joint. The purpose of the dissection was to understand the kinematic contributions of each dynamic stabilizer to the AC joint. However, it was unlikely that just a single muscle would be affected in vivo. This defect may be different from the iatrogenic dissection of the deltoid during AC reconstruction or the tearing of these attachments that occurs with high-grade AC joint separation. A standardized cadaveric testing protocol was developed to ensure reproducible dissection of the deltotrapezial defects. Figure 1 represents the experimental design of testing and dissection sequence.
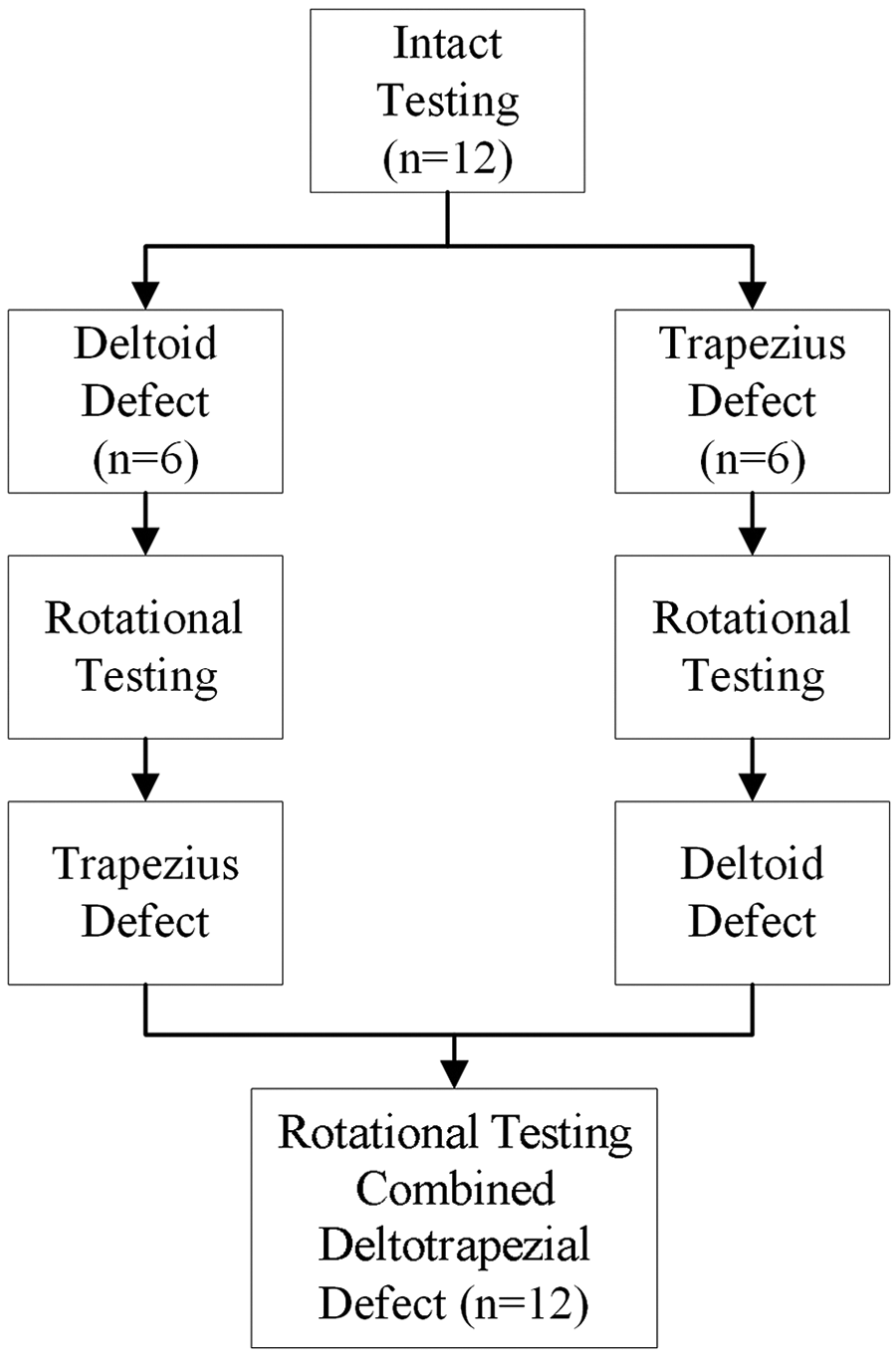
Experimental design of testing and dissection sequence.
The AC joint was identified, and 1 cm medial and lateral to the joint was marked on the deltoid and trapezial attachments (2-cm dissection in total). Specimens were randomly assigned to undergo either a deltoid-first or a trapezius-first defect before testing the combined deltotrapezial defect and the repair condition. Each native specimen served as its own control as the result of the large physiological range of differences in native rotational stability. In the native joint, the resistance to rotation (rotational torque; N · m) was measured. For ease of discussion, the relative change within each specimen was calculated using the following equation:

Specimen Preparation
The specimens were thawed at 21°C overnight and dissected free of all soft tissue except the deltoid, trapezius, AC capsule, and CC ligaments. The CC ligaments were left intact for consistent anatomic positioning of the AC joint. The glenohumeral joint was disarticulated, and the humerus was removed. After dissection, the specimens were examined and excluded if any tears to ligaments or the capsule were present.
The scapula was potted in a 7.6 × 7.6–cm polyvinyl chloride (PVC) pipe using plaster of Paris, with the inferior angle in the bottom of the pipe and the AC joint plane parallel to the pipe’s axis. 1,10 To accommodate for the variety of clavicular lengths, the clavicle was shortened so that there would be a 1.0-cm gap between the most medial deltoid attachment and the PVC pipe when potted. The medial clavicle was centrally potted in 3.2 × 7.6–cm PVC pipe using bone cement at a 90° angle to the AC joint. 1
Biomechanical Testing Setup
The plaster-cemented scapula was fixed to the X-Y-Z table of a servohydraulic testing system (MTS 858 Bionix II; MTS Systems). The cemented clavicle was secured to a custom fixture attached to a 2500-N MTS load cell. This setup allowed for the investigation of rotational loading during dissection and repair without repositioning the specimen (Figure 2A).
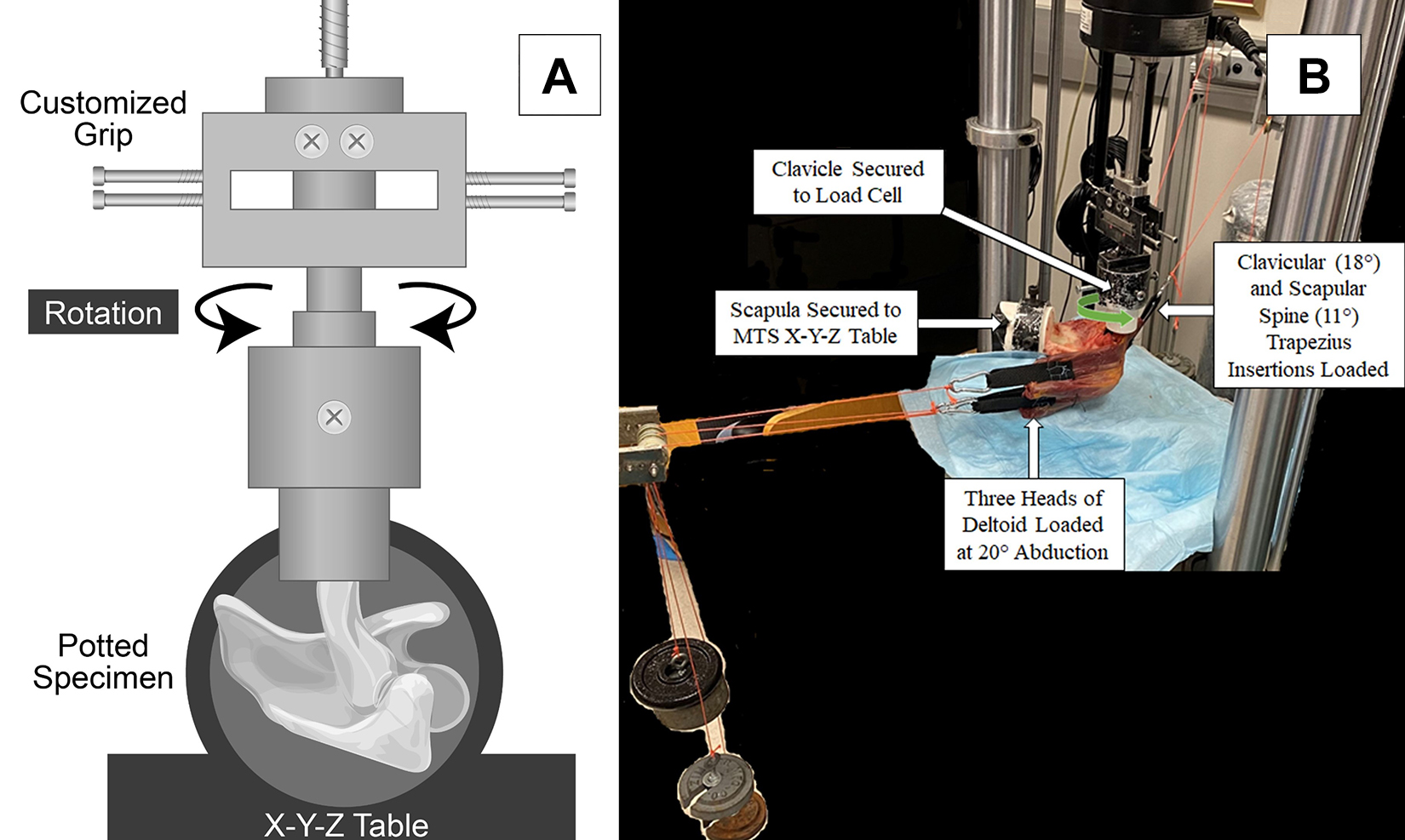
Biomechanical testing setup. (A) Custom-made fixture allowed for rotational testing of the clavicle with the scapula secured to the servohydraulic testing system. (B) The pulley system allowed for loading of the deltoid and trapezial muscles.
Polyester straps were sutured to the deltoid and trapezius to allow for weight loading during testing. Three straps were sutured to the anterior, middle, and posterior heads of the deltoid. A pulley system was designed to pull these straps at 20° of abduction. This abduction angle was chosen to simulate partial deltoid engagement. Based on calculations of loading the muscles at higher angles of abduction (increased percentage of maximal muscle force), there was concern that the straps attached to the muscle bellies would not hold in vitro. Two straps were sutured to the fibers of the trapezial insertion on the clavicle and scapular spine. The clavicular fibers of the trapezius connect from the superior nuchal line through C6, and the scapular spine trapezial fibers connect to vertebrae C7 to T1. 8 Therefore, the pulleys for clavicular and scapular trapezial loading were respectively oriented at 18° and 11° relative to the transverse plane (Figure 2B). Of note, there was no incidence of strap pullout from the muscles in which they were sutured.
Before study initiation, it was determined to load the muscles with approximately 10% of their maximum force. Maximum force was calculated according to the following formula:

Before testing, 5 cycles of a reduced rotation of 10° in the anterior and posterior direction (20° of range) were used for preconditioning. After preconditioning, the specimens underwent 10 cycles of cyclic loading with 20° of anterior and posterior rotation (40° of range) at a rate of 5 deg/s, as previously described. 1,11 The actuator moved the clavicle, and the torque required to achieve the designated degrees of rotation was recorded. The mean values of all cycles were used for analysis.
Sequential Cutting
Intact and defect conditions are demonstrated in Figure 3. After being mounted on the MTS machine, each native specimen was calibrated to neutral and underwent a native (intact) testing protocol. Figure 3A represents the native specimen. Specimens were randomized into 2 groups to receive either a “deltoid then trapezius” defect or a “trapezius then deltoid” defect using a No. 15 blade (Aspen Surgical Products). Trapezial defects (Figure 3B) were created by carefully dissecting the trapezial insertions to the posterior and posterosuperior ACLC. After the AC joint was marked, a 2-cm trapezial defect was created by dissecting 1 cm medial to the joint along the clavicle and 1 cm lateral and posterior to the joint along the acromion. Deltoid defects (Figure 3C) were created by carefully dissecting the deltoid superior, anterior, and inferior attachments to the ACLC. This was performed by marking the AC joint and dissecting 1 cm of the deltoid origin along the distal clavicle medial to the AC joint and 1 cm of the deltoid origin along the anterior acromion, creating a 2-cm deltoid defect in total.

Images representing the 4 conditions under which the specimens were tested: (A) intact, (B) “trapezius cut first” defect, (C) “deltoid cut first” defect, (D) combined deltotrapezial defect. Images are rotated 90° for anatomic orientation. AC, acromioclavicular.
These defects were determined to sufficiently cut all deltotrapezial attachments to the AC joint capsule. 22,26,30 After each dissection step, specimens were examined to ensure that the AC joint capsule was not damaged, and biomechanical testing of rotational evaluation was performed. After the first defect (trapezius or deltoid) and testing, the other muscle attachment was carefully dissected (Figure 3D). To maintain a standardized testing approach, specimens remained in the testing setup for the entirety of the defect and repair trials and were not taken down.
Anatomic Deltotrapezial Repair
After sequential dissection, anatomic deltotrapezial repair was performed as shown in Figure 4. Given a lack of tendinous insertion, a No. 0 violet monofilament PDS (polydioxanone suture, Ethicon, Raritan, NJ) was run along the muscular border of the trapezius and deltoid defect to reinforce the insertion in a simple continuous running pattern. Two FiberTak Biceps Implant Systems (Arthrex) were used to repair the deltoid and trapezius. This all-suture anchor was preloaded with 4 limbs of SutureTape (Arthrex) and 4 attached tapered needles. For the deltoid repair, a 1.9-mm drill hole was placed in the anterior clavicle 1 cm medial to the AC joint. After the anchor was inserted, it was preloaded to set the suture anchor in the intramedullary cavity. Two of the limbs were brought across the anterior ACLC and passed through the anterior edge of the acromion. The limbs were passed through the lateral deltoid defect in a horizontal mattress fashion to pull this portion of the defect against the acromion. The other 2 limbs were pulled through the medial deltoid defect in a horizontal mattress fashion to pull the medial deltoid defect against the clavicle.

Anatomic deltotrapezial repair. (A) Illustration of repair demonstrating the PDS suture (purple) running along the defect to reinforce muscular attachment and the medial (blue) and lateral (black) limbs of the suture anchor repair. Black arrows denote anchor insertion site. (B) Completed repair in the MTS machine.
For the trapezius repair, a 1.9-mm drill hole was place in the superior clavicle 1 cm medial to the AC joint. The posterior distal clavicle has limited cortical bone, which was avoided for the trapezial anchor. 31 Similar to the deltoid repair, 2 of the limbs were brought across the superoposterior ACLC and passed through the medial acromion (posterior to the ACLC). The limbs were passed through the lateral trapezial defect in a horizontal mattress fashion to secure the defect anatomically to the acromion. The other 2 limbs were pulled through the medial trapezial defect in a horizontal mattress fashion to secure this portion of the defect against the clavicle.
To standardize the repair process, the same surgeon (I.J.W.) performed all repairs. After repair, the specimen underwent 5 cycles of preloading with 10° of anterior and posterior rotation to eliminate creep before undergoing a final test of 10 cycles of 20° of anterior and posterior rotation (40° range).
Statistical Analysis
Raw data were measured as rotational torque (N·m). For ease of discussion, the change in rotational torque of each specimen was measured and used to calculate relative changes within each specimen as compared with the native specimen (equation 1). This methodology was pursued to better reflect the relative changes of each specimen in correlation with the cut sequence because the native measurements demonstrated a wide physiological range attributed to interindividual differences in size and anatomy. The data were analyzed using a Student t test for comparison of the native specimen to the cutting or repair state and repeated-measures analysis of variance (ANOVA) to compare cutting sequences within a single group. After a significant ANOVA test, differences among conditions were evaluated with the post hoc Bonferroni correction for multiple comparisons. The threshold for significance was set at P < .05. All analyses were performed with SPSS Statistics (Version 27.0; IBM).
A priori analysis was performed, and on the basis of previous studies, we assumed an SD of 0.75 N·m of rotational torque across the testing conditions, with a correlation of 0.5 among the repeated measures. Therefore, to obtain a power of 80% at an alpha level of .05 to detect a 1.0-N·m difference in rotational torque, we chose to include 12 specimens.
Results
Table 1 presents the torque required for 20° of posterior and anterior clavicular rotation.
Torque Required for 20° of Clavicular Rotation a

a Data are presented as mean ± SD.
bP Values in parentheses represent post hoc Bonferroni correction vs the intact (native) state. Bold indicates statistical significance (P < .05). Dashes denote that comparison was not made due to sequential cutting design of study.
c Deltotrapezial defect vs repair.
Posterior Clavicular Rotation: Protraction
The mean resistance in torque for 20° of posterior clavicular rotation with the native specimen was 3.93 ± 2.24 N·m. Figure 5 presents results as the percentage change from the native state.
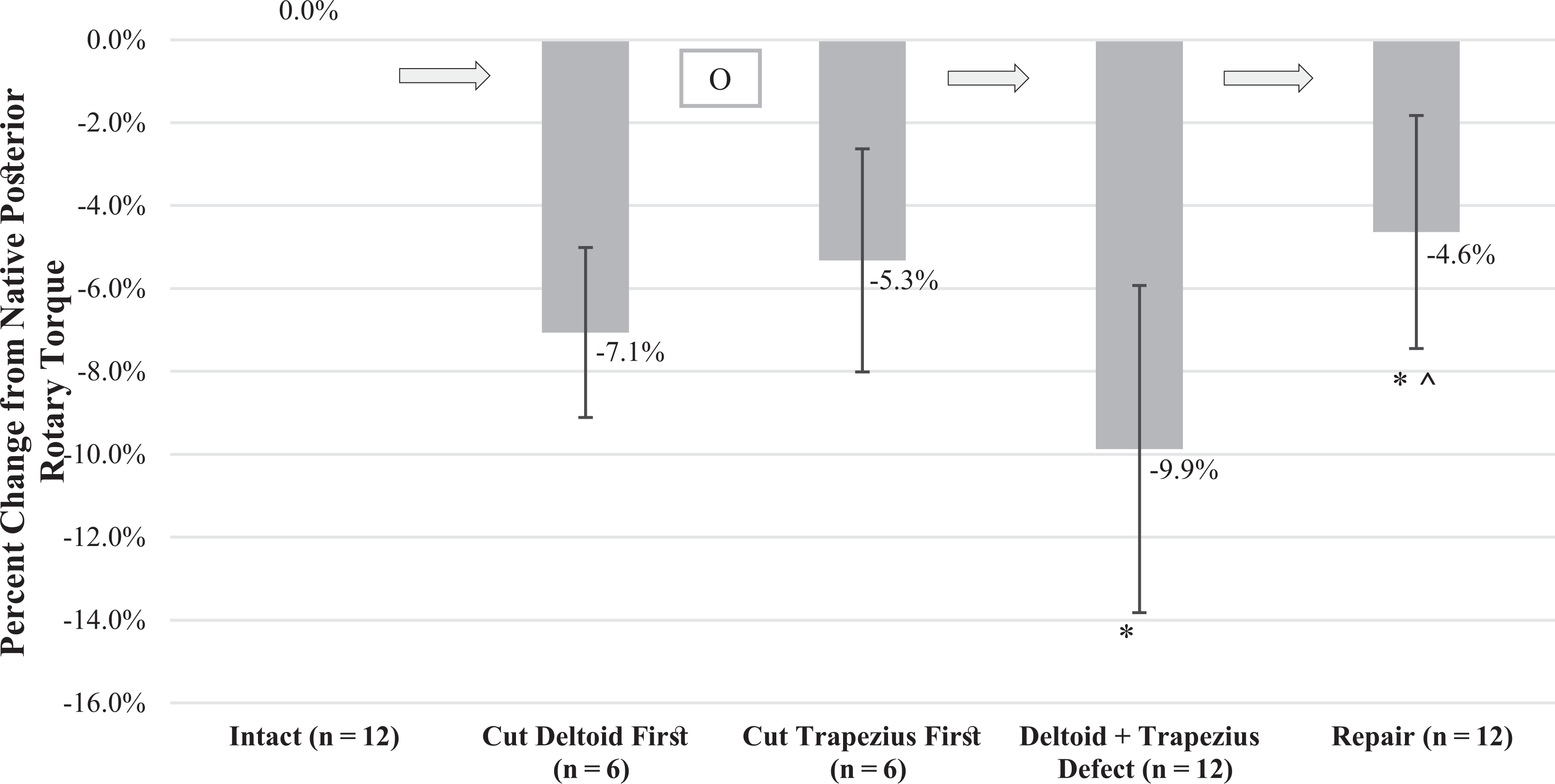
Change from native posterior rotational torque. Mean percentage change in torque required for 20° of posterior clavicular rotation in various conditions: intact (native), deltoid defect, trapezial defect, deltotrapezial defect, and after repair. Error bars denote SD. *Statistically significant decrease from intact. ^ Statistically significant increase from deltotrapezial defect. OR, odds ratio.
Individual cutting groups (n = 6) were first analyzed for variation using repeated-measures ANOVA. The deltoid-first defect group (n = 6) demonstrated a significant difference in required rotational torque: intact, 0.0%; deltoid defect, –7.1% ± 2.0%; deltotrapezial defect, –9.3% ± 3.1%; and repair, –4.1% ± 3.4% (P = .004). The post hoc Bonferroni test showed that the decreases of the deltoid-first group (P = .206) and combined deltotrapezial defect (P = .250) were nonsignificant, as well as the increase in rotational torque provided by the repair (P = .130). There was also a significant difference in required rotational torque for the trapezius-first defect group (n = 6): intact, 0.0%; trapezial defect, –5.3% ± 2.7%; deltotrapezial defect, –10.5% ± 4.9%; and repair, –5.1% ± 2.3% (P < .001; repeated-measures ANOVA). The post hoc Bonferroni indicated an insignificant decrease of the trapezius-first group (P = .079), a significant decrease of the deltotrapezial defect group (P = .046), and a nonsignificant increase of the repair group (P = .109).
Notably, when the repeated-measures ANOVA was analyzed with the exclusion of the first cut, which required analysis in 2 study arms, the case volume of the analysis increased to 12. This resulted in a significant difference when progressing from the intact state (0.0%) to the deltotrapezial defect (–9.9% ± 3.9%) and repair (–4.6% ± 2.8%) (P < .001). The post hoc Bonferroni test demonstrated that the deltotrapezial defect resulted in a significant decrease in posterior rotational torque (P = .002). The repair resulted in a significant improvement from the deltotrapezial defect (P = .001); however, the repair was still significantly lower than the native condition (P = .017).
Anterior Clavicular Rotation: Retraction
The mean resistance in torque for 20° of anterior clavicular rotation with the native specimen was 4.05 ± 2.13 N·m. Figure 6 presents results as the percentage change from the native state.
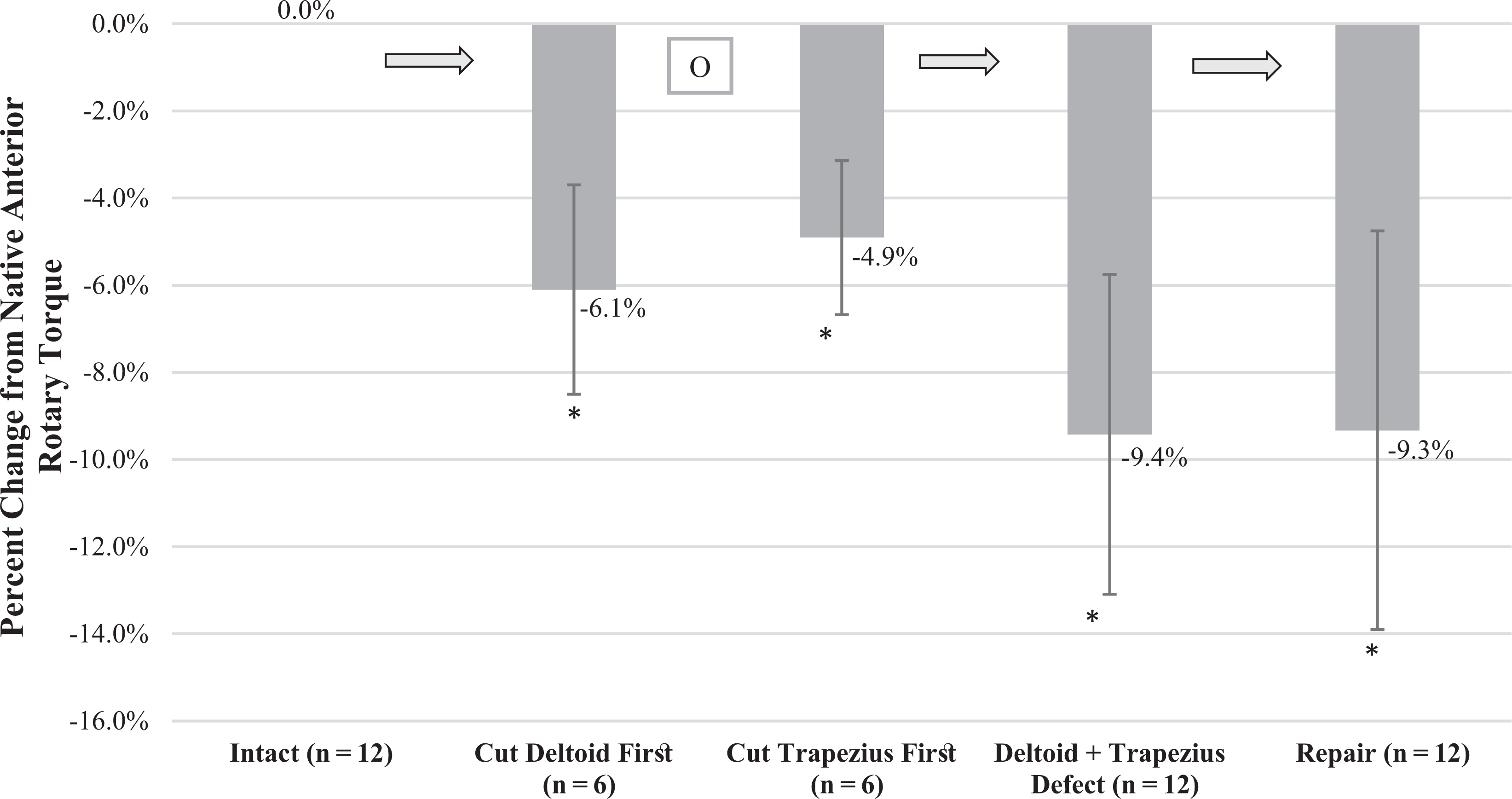
Change from native anterior rotational torque. Mean percentage change in torque required for 20° of anterior clavicular rotation in various conditions: intact (native) condition, deltoid defect, trapezial defect, deltotrapezial defect, and after repair. Error bars denote SD. *Significant decrease compared with intact (P < .05). OR, odds ratio.
Individual cutting groups (n = 6) were first analyzed for variation using repeated-measures ANOVA. The deltoid-first defect group (n = 6) demonstrated a significant difference in required rotational torque: intact, 0.0%; deltoid defect, –6.1% ± 2.4%; deltotrapezial defect, –9.4% ± 3.1%; and repair, –8.8% ± 3.9% (P < .001). The post hoc Bonferroni test showed significant decreases of the deltoid-first group (P = .002) and deltotrapezial defect (P = .010), but the repair did not significantly change anterior rotational torque (P > .999). There was also a significant difference for the trapezius-first defect group: intact, 0.0%; trapezial defect, –4.9% ± 1.8%; deltotrapezial defect, –9.5% ± 4.5%; and repair, –9.9% ± 5.5% (P < .001). The post hoc Bonferroni test indicated significant decreases of the trapezius-first group (P = .032) and deltotrapezial defect (P = .039), but the repair did not significantly change anterior rotational torque (P > .999).
When the repeated-measures ANOVA was analyzed with the exclusion of the first cut, which required analysis in 2 study arms, the case volume of the analysis increased to 12. This resulted in a significant difference when progressing from the intact state (0.0%) to deltotrapezial defect (–9.4% ± 3.7%) and repair (–9.3% ± 4.6%; P < .001). The post hoc Bonferroni test demonstrated that the deltotrapezial defect resulted in a significant decrease in anterior rotational torque (P < .001). The repair did not result in a significant difference in anterior rotational torque (P > .999), and the repair was still significantly lower than the native condition (P = .017).
Discussion
The most important finding of this study was that the deltotrapezial insertions on the AC joint capsule together provided approximately 10% of the torque required for 20° of posterior clavicular rotation (simulating protraction) and 10% of the torque required for 20° of anterior clavicular rotation (simulation retraction). The deltoid appeared to decrease rotational torque in both directions more than the trapezius; however, comparison between these groups was not statistically appropriate, as analysis was performed by comparing each specimen to itself because of interspecimen variability. The novel anatomic repair technique increased posterior rotational torque but did not support anterior rotational torque. The hypothesis that the deltoid and trapezius provide rotational stability to the AC joint was confirmed; yet, the hypothesis that the repair technique would improve rotational stability was only partially confirmed in the posterior direction, as rotational torque was increased when compared with the defect but did not restore native rotational torque.
Biomechanical investigations of the AC joint static stabilizers are well-documented 1,7 –10,14,21,25 ; however, the dynamic stabilizers (deltoid and trapezial muscles) have not been investigated biomechanically. During an open AC reconstruction, one of the initial steps is to elevate the deltotrapezial fascia from the clavicle using an incision in line with the posterior trapezial insertion and anterior deltoid origin. 4 Through the use of 3-dimensional digital footprint mapping, LeVasseur et al 22 demonstrated that the deltoid was confluent with 91% of the anterior ACLC and the trapezial insertion was confluent with 71% of the posterior ACLC with extensions over 14% of the superior ACLC. While there is limited literature to support the role of the deltoid and trapezius in AC joint stability, previous studies have investigated the role of the deltotrapezial fascia. 6,27 Czerwonatis et al 6 performed an anatomic evaluation of the deltotrapezial fascia from 11 cadaveric specimens, finding that the fascia covered the distal descending trapezius and ran over the AC joint to the proximal deltoid. They observed that the most robust fiber content (mean thickness, 1.7 mm; range, 1-2 mm) was located over the AC joint, where its fibers connected to the capsule. Pastor et al 27 performed a biomechanical in vitro study of 8 cadaveric specimens with sequential injury to the AC ligaments and deltotrapezial fascia. This study concluded that when compared with the native shoulder, defects to the AC ligaments and deltotrapezial fascia resulted in a 1.11° increase in anterior clavicular rotation (P = .012) and 2.71-mm increase in lateral translation (P = .017). Although the present study analyzed the impact of injury directly to the deltoid and trapezius rather than the deltotrapezial fascia, these results align with our findings. The present study found that dissection of the deltoid and trapezial AC joint capsule attachments (with the AC joint capsule and CC ligaments intact) reduced the torque required to rotate the clavicle in the posterior direction by 9.9% (P = .002) and the force to rotate the clavicle in the anterior direction by 9.4% (P < .001). These findings suggest that the deltoid and trapezius support the rotational stability of the AC joint.
With radiographic studies demonstrating rates of loss of reduction ranging from 30% to 53%, 12,15,17,19 surgical management of AC joint reconstruction must continue to develop. Based on the clinical practice of the senior author (A.D.M.), our hypothesis was that the complex in vivo motion of protraction may be contributing to unsatisfactory reduction results. One part of this complex motion is anterior scapular tilt, which at the AC joint capsule is a comparative motion with posterior clavicular rotation. Restoring the native rotational stability of the AC joint has proven more difficult in biomechanical studies than the restoration of superoinferior or anteroposterior displacement. 1,10,25 Beitzel et al 1 noted that anatomic CC ligament reconstruction most successfully restored displacement of the joint during anterior and posterior rotation, but the motion at the AC joint was greater than that of the native condition (P < .001). Dyrna et al 10 stated that complete capsulotomy of the AC joint capsule decreased rotational stability by 89% to 98% of the native state. Their combined AC and CC reconstruction improved the rotational stability but was still significantly weaker than the native condition (P = .01). Morikawa et al 25 cited a significant reduction in posterior rotational torque versus the native state after dissection of the superior AC joint capsule. The study partially restored rotational stability with repair of the superior capsule with suture; however, the repair failed to restore native rotational stability. The present study demonstrated that the deltoid and trapezial muscles play a role in posterior and anterior rotational stability. The anatomic deltotrapezial repair increased posterior rotational torque by 5.3%; however, the repair did not fully restore native posterior rotational torque.
Lizaur et al 23 reported that up to 93.5% of patients with acute complete dislocation of the AC joint requiring operative treatment have damage to the deltoid, trapezius, or both. Clinically, these findings may be most impactful with moderate and severe AC joint injuries (eg, Rockwood types 3-4), especially type 4 injuries in which the clavicle is displaced posteriorly through the trapezius. 13 Only 1 study has attempted to incorporate the deltoid and trapezius into the repair during AC reconstruction. 23 Those authors repaired AC separations in 46 patients by suturing the deltoid and trapezius over the clavicle and used temporary wire fixation of the CC ligaments. With a mean 5.8 years of postoperative follow-up (range, 2-7.9 years), the authors noted that just 10.9% of patients had redisplacement of the AC joint. It is important to note that distal clavicle excision is sometimes performed during AC joint and CC ligament reconstruction, and this may involve removing the native attachment sites of the dynamic stabilizers. Additionally, further consideration to minimize the resection of the deltoid and trapezius during open AC reconstruction should be considered to enhance postoperative rotational stability. These findings may favor arthroscopy-assisted AC reconstruction over open techniques when feasible, considering the reduced injury to the deltoid and trapezius.
Limitations
This study is not without limitations. First, as with all biomechanical studies, the in vitro setting and use of cadaveric specimens may not accurately replicate an in vivo setting with live patients. During high-grade AC joint injuries, there may not be defined tissue to repair, as opposed to when the deltotrapezial fascia is released during surgical repair. After the attempted repair technique, there was no scar tissue formation expected during in vivo postoperative healing. Adding 2 anchors to the clavicle may increase the risk of fracture; however, we feel that this risk is minimized by the small drill hole (1.9 mm) and the use of an all-suture anchor. To maintain optimal soft tissue integrity, only fresh-frozen cadaveric specimens were used, and specimens were thawed just once, immediately before testing, and tested just once to minimize tissue damage.
A second limitation is that, to simulate rotational forces felt during protraction and retraction at the joint, the clavicle was rotated posterior and anterior. This motion ignores the complex addition of anterior acromial translation and internal/external scapular rotation placed on the joint with protraction. Additionally, there is no way to isolate and test patients for loss of rotational stability clinically. Third, the deltoid and trapezius are dynamic stabilizers of the AC joint. Given the in vitro nature of this study, they were tested only at predetermined loads and angles to limit the testing on a single specimen. The loads and angles used in the study may not reflect the in vivo relationship between the muscles and the AC joint capsule. Last, the mean age of the cadavers in this study was 60.25 years. Even though this study used each specimen as its own control, the advanced age of the specimens could have influenced rotational stability of the joint.
Conclusion
This study demonstrated in an immediate postoperative cadaveric model that the deltoid and trapezius play a role in clavicular rotational stabilization. The proposed anatomic repair improved posterior rotational stability but did not improve anterior rotational stability as compared with the deltotrapezial defect; however, neither was restored to native stability. Limiting damage and improving the repair of these muscles should be a consideration during AC reconstruction.
Footnotes
Acknowledgment
The authors thank Geneva Hargis, PhD, and Christopher Bonin, PhD, for creating the medical illustrations.
Final revision submitted May 22, 2022; accepted June 6, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: The study was funded internally by the University of Connecticut Department of Orthopaedic Surgery. Implants for the study were donated by Arthrex; the company had no influence on the study design, data collection, or interpretation of the results or the final manuscript. A.D.M. has received consulting fees from Arthrex and Astellas Pharma, speaking fees from Kairos Surgical, and honoraria from Arthrosurface. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.