
Abstract
Background:
Rapid consolidation of the bone block is paramount for the success of the Latarjet procedure. Noncannulated screws have shown satisfactory long-term bone block fusion, while cannulated screws are challenged with inferior mechanical properties and fusion rates.
Purpose:
To report outcomes of the Latarjet procedure using cannulated screws, notably bone block fusion and complication rates at 3 months, as well as clinical scores and return to sports at minimum 2 years postoperatively.
Study Design:
Case series; Level of evidence, 4.
Methods:
We reviewed the records of 124 consecutive patients (124 shoulders) who underwent primary Latarjet procedures using cannulated screws between 2015 and 2018. All patients underwent clinical examination at 3 months postoperatively, including range of motion and radiographs to assess graft fusion. The Walch-Duplay score, Rowe score, Subjective Shoulder Value, and visual analog scale for pain were collected at a minimum follow-up of 2 years.
Results:
Overall, 9 patients (7%) required reoperation: 7 (6%) had screw removal for unexplained residual pain, 1 (0.8%) had lavage for deep infection, and 1 (0.8%) had evacuation to treat a hematoma. Furthermore, 3 patients (2.4%) had recurrent instability, none of whom underwent reoperation. At 3-month follow-up, all 124 shoulders showed complete radiographic graft fusion, and at 40 ± 11 months (mean ± SD; range, 24-64 months), 88% of patients had returned to sport (109/124), the Walch-Duplay score was 86 ± 14, Rowe was 84 ± 15, Subjective Shoulder Value was 88 ± 11, and visual analog scale for pain was 1 ± 1.
Conclusion:
The clinical relevance of these findings is that 4.5-mm cannulated screws are safe and effective for primary Latarjet procedures and grant adequate graft healing, with low recurrence of instability and a high rate of return to sports.
Anterior shoulder instability with or without bone loss can be treated via arthroscopic labral or capsular repair 14,26,32 or via bone block procedures (e.g. coracoid process, iliac crest, or distal tibial allograft). 11,14,17,23 Recent systematic reviews have confirmed the efficacy of bone block procedures at preventing recurrent dislocations, 10,21,22 notably the Latarjet procedure, which transfers the coracoid process to the anteroinferior margin of the glenoid 13,43 and provides adequate clinical outcomes with minimal complications and progression of osteoarthritis. 38
Rapid consolidation of the bone block is paramount for the success of the Latarjet procedure, 7 where fixation is typically achieved using 2 screws for optimal compression and contact. Noncannulated screws have shown satisfactory long-term bone block fusion and low recurrence of instability 29 but can be challenging to position within the limited working space and access through the surrounding muscles. 31 Cannulated screws are easier to position, as they can be inserted over guide wires, which may be repositioned if necessary, although some authors have argued that their use is associated with reduced strength 25 and increased costs. 36
In 2012, Shah et al 35 published the outcomes of 48 Latarjet procedures; only 5 shoulders had received cannulated screws, 4 of which had recurrent instability. The authors observed no cases of recurrent instability in the remaining 43 shoulders that received noncannulated screws and thus postulated that cannulated screws offer inferior fixation because of reduced thread depth and purchase within the scapula and hence insufficient graft compression. Thereafter, several biomechanical studies on bone block fixation found no difference in graft stability using cannulated or noncannulated screws, 1,36 whereas others reported inferior stability using cannulated screws. 41,42
The senior author (L.N.) has been performing the Latarjet procedure using the same cannulated screws in the past 7 years. Therefore, the purpose of the present study was to report the outcomes of the Latarjet procedure using cannulated screws to ascertain bone block fusion and complication rates at postoperative 3 months, as well as clinical scores and return to sports at ≥2 years. The hypothesis was that cannulated screws would grant similar outcomes to those of noncannulated screws in the recent literature.
Methods
Study Design
The protocol for this study received approval from our institutional review board. We retrospectively reviewed the records of 150 consecutive patients (153 shoulders) who underwent primary Latarjet procedures between 2015 and 2018 by the same senior surgeon (L.N.). To eliminate factors that could affect shoulder apprehension or compromise return to sports, we excluded 17 patients (17 shoulders) who underwent surgical procedures on the contralateral shoulder, 6 patients (6 shoulders) who had previous surgical procedures on the ipsilateral shoulder, and 3 patients (6 shoulders) who had bilateral procedures. This left a cohort of 124 patients (124 shoulders), all of whom provided informed consent for their participation in this study.
Preoperative Assessment
We retrieved patient characteristics; cause of first anterior instability episode; time from first dislocation/subluxation to surgery; level of sport; and preoperative range of motion (ROM), including active forward elevation, internal rotation, and external rotation with the elbow at the side (ER1) and at 90° of abduction (ER2).
Surgical Technique
All operations were performed by the same surgeon (L.N.) with the patient in the beach-chair position under general anesthesia using an interscalene block. A 4- to 5-cm vertical incision was made extending distally from the tip of the coracoid. The deltopectoral interval was identified and developed. The coracoacromial ligament was identified and incised, leaving a 1.5-cm stump of tissue. The pectoralis minor was then released from the medial aspect of the coracoid, and an osteotomy was made using an oscillating right angle saw from medial to lateral at the junction of the horizontal and vertical aspects, aiming to harvest a 2.5- to 3-cm coracoid bone block to form the graft.
When completely mobilized, the graft was held using a Bone-Block Grasper (Arthrex, Inc) and flipped to debride and prepare its posterior aspect using a saw to obtain a flat cancellous surface. Two 1.57-mm pins were inserted at least 1 cm apart, perpendicular through the graft, and holes were drilled using a 3.2-mm drill. 43 A subscapularis split was performed at the junction of the superior two-thirds and the inferior one-third. Retractors were placed to provide glenoid exposure: (1) a Kolbel retractor medially in the subscapularis fossa; (2) a 4-mm Steinman pin placed in the superior glenoid neck, retracting the superior subscapularis; and (3) a Hohmann retractor placed over the inferior aspect of the subscapularis and under the inferior glenoid neck. A vertical capsulotomy was made using a knife at the level of the joint line. A Trillat humeral head retractor was inserted into the joint through the capsulotomy, retracting the humeral head and the anterior capsule laterally.
After the anterior glenoid was clearly exposed, the anterior labral lesion was confirmed and excised with the bony Bankart fragment if present. The anterior glenoid was prepared using an osteotome to obtain a flat decorticated surface with bleeding bone. First, a 1.57-mm inferior pin was inserted at the 5-o’clock position (right shoulder) or 7-o’clock position (left shoulder) approximately 7 mm medial and parallel to the glenoid joint line. 43 A trocar was used to avoid any possible impingement on the surrounding soft tissues and protects the brachial plexus. The trocar was removed, and the position of the pin was assessed (if necessary, the 1.57-mm pin can be repositioned without jeopardizing the glenoid bone stock).
A 3.2-mm cannulated drill bit was then used to drill over the pin to create the inferior bicortical hole in the glenoid. The graft was retrieved and positioned with the grasper over the inferior drill hole, and a gauge was used to measure the length of the screw required to cross the graft and the glenoid (available in 2-mm increments from 30 to 40 mm). A 4.5-mm titanium partially threaded cannulated low-profile screw (length of threads, 12 mm; Arthrex, Inc) was inserted over the pin, provisionally fixing the graft, but not tightened in case slight alterations were needed to ensure that the superior graft was aligned along the joint line to avoid lateral overhang of the graft. After appropriate positioning of the graft was obtained, the inferior screw was fully tightened to seat the graft without excessive pressure. Second, the superior bicortical hole in the glenoid was drilled through the superior hole of the coracoid graft. Finally, the length of the superior screw was measured using a gauge and tightened to achieve final graft fixation (Figure 1).
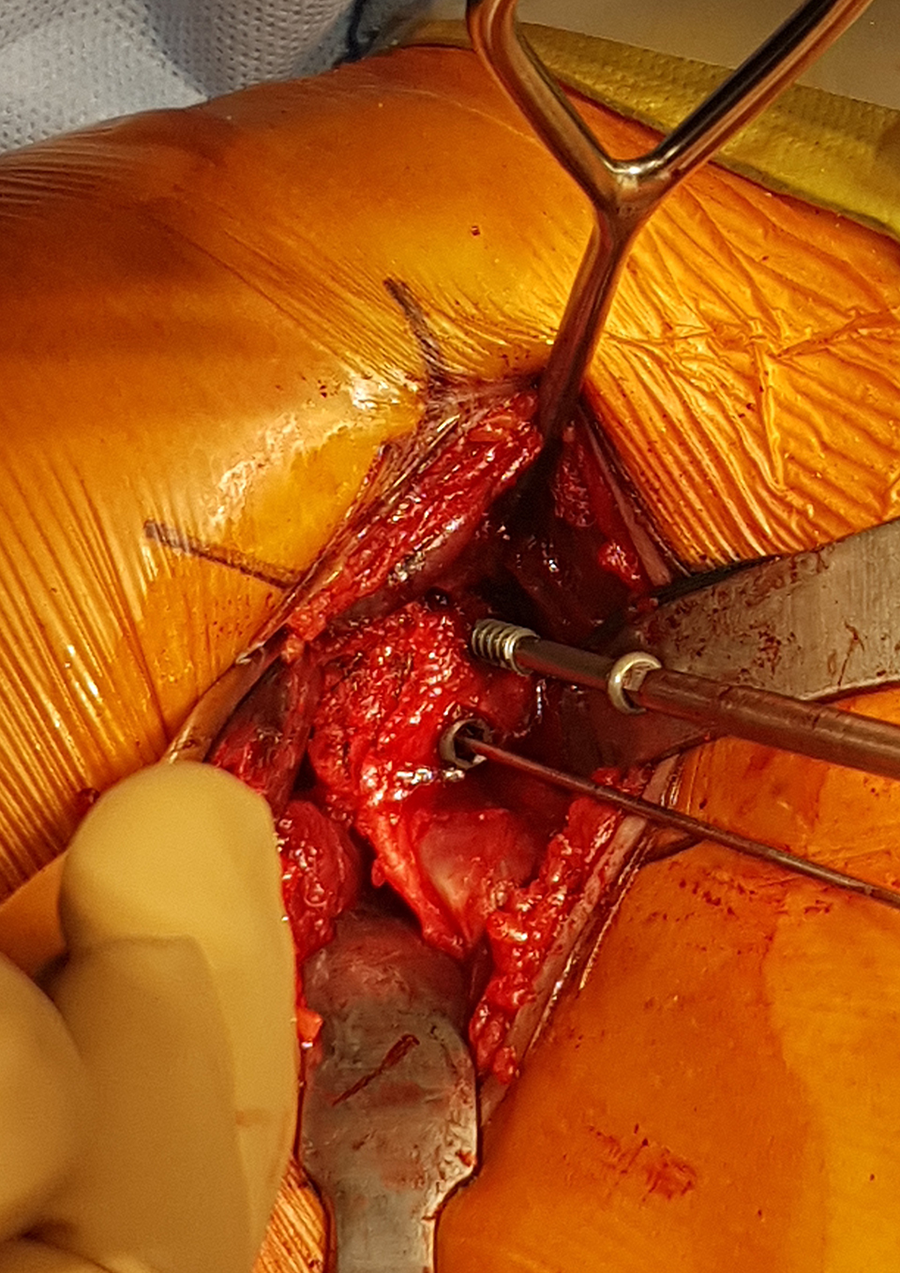
The superior screw is inserted and tightened to achieve final graft fixation.
After the graft was adequately fixed to the anterior glenoid, the Trillat humeral head retractor was removed. The anterior capsule was then sutured to the remaining stump of the coracoacromial ligament with the arm in external rotation. 29,30 The subcutaneous tissues and skin were closed, and a dressing was applied.
Postoperative Rehabilitation
The shoulders were immobilized using a sling for a minimum of 2 weeks to prevent pain, and all patients started self-rehabilitation exercises 2 days after surgery, following a standard protocol. 33 Patients were allowed to return to daily activities after 2 weeks and to resume sport after 3 months, only if they had recovered mobility and had complete radiographic graft fusion.
Postoperative Evaluation
All patients underwent clinical examination at 3 months, during which we assessed ROM, including active forward elevation, internal rotation, ER1, and ER2. Bernageau view radiographs 5 were acquired under fluoroscopic guidance to assess graft fusion, which was confirmed if full contact between the graft and the glenoid was visible (Figure 2). At a minimum follow-up of 2 years, we noted whether and to what level patients returned to their main preoperative sport; whether any patients experienced postoperative stiffness (ROM deficit >20° in ≥2 planes vs contralateral shoulder); and clinical scores such as Walch-Duplay, 39 Rowe, 37 Subjective Shoulder Value (SSV), 18 visual analog scale for pain, and satisfaction.

Bernageau view radiographs were used to assess graft fusion, which was confirmed if full contact between the graft and the glenoid was visible.
Statistical Analysis
The normality of distributions was assessed using Shapiro-Wilk test. For normally distributed continuous data, differences between groups were evaluated using analysis of variance, while for nonnormally distributed data, differences were evaluated using Kruskal-Wallis test. Pre- and postoperative scores were evaluated using paired t test or Wilcoxon signed rank test. Statistical analysis was performed using R Version 3.4.3 (R Foundation for Statistical Computing). P values <.05 were considered statistically significant.
Results
The final cohort of 124 patients comprised 99 men (80%) and 25 women (20%) aged 26.0 ± 7.8 years (mean ± SD; range, 15-49 years) at the time of the Latarjet procedure (Table 1). The mean time from first instability episode to surgery was 4.2 ± 4.7 years (range, 0-22 years), and most episodes were caused by trauma (n = 109; 88%). Only 5 patients (4%) had work-related incidents.
Patient Characteristics (124 Shoulders)
a Hill-Sachs lesion sizes: small = visible only during internal rotation; medium = visible during internal and neutral rotation; large = visible during internal, neutral, and external rotation.
After the surgery, 11 patients (9%) had postoperative stiffness at 3 months after surgery, but all recovered mobility at 4 months, with 9 (7%) requiring reoperation: 7 (6%) had screw removal for unexplained residual pain, 1 (0.8%) had lavage for deep infection, and 1 (0.8%) had evacuation to treat a hematoma. In the 7 patients who required screw removal, bone resorption was observed on the anterosuperior facet of the graft. Furthermore, 3 patients (2.4%) had recurrent instability, none of whom underwent reoperation: 2 had traumatic subluxations with bone block lysis, diagnosed on computed tomography (CT) scans at 14 months (n = 1) and 18 months (n = 1), while 1 patient with myasthenia gravis before the index procedure had idiopathic subluxation.
Of the 124 patients, 122 (98%) played sport preoperatively, and 109 (89%) returned to sport postoperatively. A total of 63 (51%) returned to their main sport at the same or higher level (43 overhead sports, 20 nonoverhead sports); 33 (27%) returned to their main sport at a lower level (16 overhead, 17 nonoverhead); 13 (11%) changed sport (6 overhead, 7 nonoverhead); and 13 (11%) stopped sports (7 overhead, 6 nonoverhead). Of the 33 patients who returned to their main sport at a lower level, 7 indicated that this was a professional reason, 12 said that it was a personal reason, 4 attributed it to an injury unrelated to the operated shoulder, and 10 stated that it was because of the operated shoulder. Of the 13 patients who stopped sports, 7 said that this was related to the operated shoulder, while 6 cited other reasons.
At 3-month follow-up, all 124 shoulders showed complete graft fusion on Bernageau view radiographs, though it was not possible to measure or assess graft resorption. None of the patients exhibited signs or symptoms of nonunion, so CT scans were not acquired to assess graft fusion. The active forward elevation was 164° ± 13° (range, 120°-180°), ER1 was 53° ± 17° (range, 0°-90°), and ER2 was 87° ± 10° (range, 70°-100°), while ER1 on the contralateral shoulder was 63° ± 15° (range, 30°-90°) (Table 2).
Preoperative and 3-Month Postoperative Range of Motion a

a Data are reported as mean ± SD (range) degrees or No. (%).
At final follow-up of 40 ± 11 months (range, 24-64 months); the Walch-Duplay score was 86 ± 14; Rowe was 84 ± 15; SSV was 88 ± 11; visual analog scale for pain was 1 ± 1; and satisfaction was rated as disappointed in 4 patients (3%), satisfactory in 6 (5%), good in 31 (25%), and excellent in 82 (67%) (Table 3). The 4 patients who reported their satisfaction as disappointed indicated it was due to recurrence of instability (n = 3) and inability to return to sports owing to their operated shoulder (n = 1).
Postoperative Clinical Outcomes (n = 124)

Discussion
The most important finding of the present study was that at 3-month follow-up, all 124 shoulders showed complete graft fusion on Bernageau view radiographs. Furthermore, at a mean final follow-up of 40 ± 11 months, 89% of the cohort returned to sports, and the clinical scores as well as ROM were satisfactory, though 3 patients (2.4%) had recurrent instability and 9 (7.3%) required reoperation. None of the complications encountered were related to nonunion, and none of the patients exhibited signs or symptoms of nonunion; thus, CT scans were not acquired to assess graft fusion, as they were deemed unnecessary considering the cost and exposure to radiation. It remains therefore difficult to ascertain that none of the patients had any delayed graft healing or transitory nonunion, though the remaining clinical outcomes support this assumption. The clinical relevance of these findings is that 4.5-mm cannulated screws are safe and effective for primary Latarjet procedures in shoulders that had no previous surgical procedures. The same cannulated screws could also be safe and effective in shoulders that had previous surgery, though their suitability may depend on the type of prior surgery and on the reason for failure or revision, but this merits further investigation.
Shah et al 35 reported that only 5 patients in their series received cannulated screws, of which 4 (80%) experienced recurrent instability, which might have been due to the inclusion of several revision procedures in patients with failed primary procedures. Even though Shah et al did not state other reasons for the high rate of recurrences, it might have been due to the unfamiliarity of using cannulated screws or a learning curve. In the present series, 3 patients (2.4%) had recurrent instability, which is lower than the rate of 8.5% cited by a recent systematic review on long-term outcomes. 22
Several biomechanical studies on graft fixation have found no difference in graft stability using cannulated or noncannulated screws, 1,36 whereas others have reported inferior stability using cannulated screws. 41,42 Alvi et al 1 found no difference in the mean number of cycles to failure or energy to failure between cannulated and noncannulated screws, although they did note catastrophic failure of 1 cannulated screw on initiation of testing. Willemot et al 41 compared 2 types of cannulated screws (3.5 and 3.75 mm) and 1 type of noncannulated screw and noted greater displacements using the 3.75-mm cannulated screw. Comparison between biomechanical studies and clinical series is difficult because of the variety of cannulated and noncannulated screws available; the extent to which screw diameter, material, and thread properties affect screw strength and effective stability remains unclear.
In the present series, patients achieved satisfactory clinical scores using cannulated screws. At a follow-up of 40 ± 11 months, the Walch-Duplay score was 86 ± 14, Rowe was 84 ± 15, and SSV was 88 ± 11, which are comparable with scores in a recent systematic review 22 that indicated a weighted mean Walch-Duplay score of 88.5, Rowe of 88.5, and SSV of 89.1. Furthermore, the present series had a graft union rate of 100% at 3 months after surgery, which is better than that in a recent systematic review by Malahias et al, 27 who cited a graft union rate of 94.6%.
It is worth noting that in the present series, 7 patients (5.6%) required screw removal owing to unexplained pain. This rate is comparable with findings of Godenèche et al, 19 who performed a study specific to screw removal for unexplained pain after the Latarjet procedure and postulated that it might be due to soft tissue impingement between the screw and the subscapularis muscle. Complications after the Latarjet procedure are mainly due to technical mistakes, such as malpositioning or insufficient screw length, 4,15,20 which may cause nonunion 34 or degenerative glenohumeral arthritis, 29 and the risk for these complications decreases as surgeons gain experience. 9,12,24 Soft tissue impingement could be decreased by using alternative fixations, such as resorbable screws and cortical suspension devices. Whereas resorbable screws have been noted to increase risks of osteolysis 3 and fractures 40 as compared with nonresorbable screws, EndoButtons 6,9,28 may provide an alternative to screw fixation, although their outcomes are still not clear. Specifically, some studies have found comparable load to failure 31 and functional results 28 to screw fixation without complications related to hardware removal, 6,9,16,28 while others have indicated delayed graft fusion with greater graft mobilization. 2,8
Limitations
The results of this study should be interpreted with the following limitations in mind. First, we did not collect preoperative clinical scores, imaging information on the labrum, and capsular status, and we did not assess the timing of return to sports or quantify bone loss. Second, while Bernageau view radiographs under fluoroscopic guidance are more reliable than standard radiographs to assess graft fusion, CT scans would be more accurate to detect nonunion and graft resorption; however, they are not routinely acquired, as they incur considerable costs and exposure to radiation, which can be justified only if patients present with symptoms or radiographic signs of nonunion or lysis of the graft. Finally, the present findings cannot explain why previous studies found inferior strength and/or stability using cannulated screws: the cause-and-effect relationships remain unclear, and the various cannulated screws available for the Latarjet procedure differ in material composition, inner and outer diameters, thread depth and coarseness, and insertion torque and pressure.
Conclusion
The clinical relevance of these findings is that 4.5-mm cannulated screws are safe and effective for primary Latarjet procedures in shoulders that had no previous surgical procedures, while granting adequate graft healing, with low recurrence of instability and a high rate of return to sports.
Footnotes
Acknowledgment
The authors are grateful to Mo Saffarini and Luca Nover for their assistance with statistical analysis and manuscript preparation.
Final revision submitted May 5, 2022; accepted May 24, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: The statistical analysis and manuscript preparation for this study were funded by GCS Ramsay Santé pour l’Enseignement et la Recherche. L.N. has received consulting fees from Arthrex and Wright, royalties from Wright, and stock options from Sparta Biopharma. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from GCS Ramsay Santé pour l’Enseignement et la Recherche (COS-RGDS-2020-05-014-NEYTON-L).