
Abstract
Background:
Determining the rotational axis of the bony trough during lateral meniscal allograft transplant (MAT) is difficult. The use of anatomic landmarks may help a surgeon determine the rotational alignment of the graft during the procedure.
Purpose:
To investigate the association between the knee's anatomic landmarks and the position of the bony trough to prevent extrusion after lateral MAT.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Enrolled were 44 patients who underwent lateral MAT between July 2000 and February 2011. The patients’ mean age at the time of surgery was 30.8 years. Extrusion was measured on magnetic resonance imaging (MRI) scans at a mean of 3.6 months postoperatively, and patients were divided into an extrusion group (n = 15) and a no-extrusion group (n = 29). Three coronal MRI scans from each patient were selected, each from the region at the level of the tibial tuberosity (TT), the anterior bony trough, and the posterior bony trough. We measured the distance between the center of the anterior bony trough and the center of the TT (the TT distance) and the distance between the center of the posterior bony trough and the medial border of the lateral femoral condyle (LFC) (the LFC distance).
Results:
The mean center of the anterior bony trough was in a more medial position relative to the center of the TT in the no-extrusion group (–2.9 ± 4.8 mm) compared with the extrusion group (1.3 ± 4.9 mm; P = .010). The mean center of the posterior bony trough was in a more medial position relative to the medial border of the LFC in the no-extrusion group (–1.7 ± 3.9 mm) compared with the extrusion group (1.0 ± 3.2 mm; P = .027). Both TT distance and LFC distance were significantly correlated with extrusion (P = .005 and .025, respectively). The cutoff value was –0.24 mm for the anterior bony trough and –0.58 mm for the posterior bony trough (negative values indicate that the trough was medial to the respective landmarks).
Conclusion:
To prevent extrusion of the allograft, the center of the anterior bony trough needs to be aligned with the center of the TT, and the center of the posterior bony trough needs to be aligned with the medial border of the LFC.
Meniscal allograft transplant (MAT) has been performed to prevent the development of arthritic changes in young, active patients after subtotal or total meniscectomy. 18 However, nonanatomic placement of the meniscal horn increases the risk of early graft failure after MAT. 5 Therefore, anatomic placement of the meniscal allograft is imperative to achieve satisfactory outcomes. 3,5,10 Although some surgeons prefer performing MAT without attaching a bone block, 4 the lateral meniscal allograft is usually prepared with a bony bridge or keyhole connecting both horns because the distance between the anterior and posterior horns is very short. 3,5,23 Accurate placement of the lateral meniscal allograft depends on the position of the bony bridge or keyhole. Errors in placement of the bony bridge or keyhole can occur during lateral MAT, resulting in midbody extrusion. 3,10
The meniscal allograft should be placed anatomically along the centers of both anterior and posterior horns of the patient’s knee. However, determining the centers of both horns of the lateral meniscus during MAT is difficult. Cadaveric studies have demonstrated that the posterior insertion of the lateral meniscus attaches 2.6 to 5.8 mm medial to the lateral tibial spine. 14,15,21 A magnetic resonance imaging (MRI) study revealed that the most common insertion sites of the posterior horn of the lateral meniscus were the medial tibial spine and lateral tibial spine. 17 Another study reported that the posterior horn insertion was attached to the intertubercular area just posteromedial to the tibial attachment of the anterior cruciate ligament (ACL) and the posterior slope of the lateral tibial spine. 24 The anterior horn of the lateral meniscus is braided with the tibial insertion of the ACL. 6 Overlapping of the lateral meniscal anterior horn by the ACL tibial insertion has been quantitatively investigated. 7,19 It is difficult to determine the center of the anterior horn without dissection.
When a surgeon prepares the bony keyhole in lateral MAT, the lateral tibial spine is used as a landmark to determine where to place the bony keyhole. 10,13,23 However, the direction of the lateral tibial spine is not coincident with the line connecting the centers of both horns of the lateral meniscus. 2 Moreover, determining the rotational axis of the bony trough during the operation is difficult. There is a paucity of literature reporting anatomic landmarks that can aid rotational alignment of the graft during lateral MAT.
The purpose of this study was to investigate the associations between anatomic landmarks and the position of the bony trough to prevent extrusion of the lateral MAT. We hypothesized that there would be constant associations between anatomic landmarks and the position of the bony trough to prevent extrusion in lateral MAT.
Methods
Patients
Between July 2000 and February 2011, a total of 46 consecutive lateral MATs using a fresh-frozen graft were performed by a single surgeon (N.H.C.) at a single institution. Indications for MAT were young, active patients with pain in the lateral compartment for >6 months after previous surgery. All patients had previously undergone subtotal or total meniscectomy for complex tear or irreducible bucket-handle tear of the lateral meniscus. They had no valgus malalignment >3°, which was confirmed on long-leg standing radiography. The patients had no diffuse Outerbridge grade 3 chondromalacia in the lateral compartment. Contraindications were patients with diffuse chondromalacia of the lateral compartment higher than grade 3 and those with lower limb valgus malalignment >3°.
The inclusion criterion was primary lateral MAT with or without concomitant ligament surgery. Exclusion criteria were untreated ligamentous instability or age >50 years. The patients who did not undergo follow-up MRI after surgery were also excluded. The study protocol was reviewed and approved by an institutional review board, and all patients provided written informed consent.
Surgical Procedure
On coronal-view MRI scans, the size of the meniscal allograft was measured preoperatively. The lateral meniscal allograft was prepared using a bony bridge. The recipient meniscus was debrided to expose the meniscocapsular junction of the posterior horn and midbody. A mini-arthrotomy was performed, and the anterior horn of the recipient meniscus was excised. A bony trough was made just lateral to the ACL insertion on the tibia along the line between the anterior and posterior horns of the lateral meniscus. The bony bridge of the allograft was inserted into the bony trough, and arthroscopy was used to confirm the correct position of the meniscal allograft. Meniscal repairs were performed as described in literature. 14
After surgery, partial weightbearing was permitted as soon as tolerated, and closed kinetic chain exercises were started as early as possible. Full weightbearing was allowed after 6 weeks and squatting after 12 weeks. Jogging began after 4 to 5 months. Return to sports activity was allowed after 6 to 8 months.
Postoperative MRI Evaluation
All patients underwent follow-up MRI within 6 months after surgery so we could evaluate allograft status and check for extrusion. On coronal MRI scans, a view showing the maximum extrusion of the midbody was chosen, and the distance between the outer edge of the articular cartilage of the tibial plateau and the outer edge of the allograft was measured. Extrusion was defined as a distance of >3 mm. 9 Patients were divided into 2 groups according to whether extrusion was present or absent.
To determine the rotation of the bony trough on the axial plane, the center of the tibial tuberosity (TT) and the medial border of the lateral femoral condyle (LFC) were chosen as constant anatomic landmarks during surgery and postoperative MRI evaluation. The TT can be palpated easily during surgery and can be used as a landmark for the anterior part of the bony trough by follow-up MRI evaluation. The medial border of the LFC is located just lateral to the lateral tibial spine. It can be used as a landmark during arthroscopy at a knee flexion angle of 90° as well as a landmark for the posterior part of the bony trough on follow-up MRI.
For each patient, 3 coronal MRI scans were selected: those showing the center of the TT, the anterior trough, and the medial wall of the lateral condyle at the posterior trough. In addition, an axial MRI scan was chosen that provided the best view of the bony trough (Figure 1). On the coronal images, a vertical line was drawn through the center of the TT, and another vertical line was drawn through the center of the anterior bony trough.

(Left) Axial magnetic resonance imaging (MRI) scan showing the best view of the bony trough. (Right) Coronal MRI scans showing the center of the tibial tuberosity (top), anterior trough (middle), and medial wall of the lateral condyle at the posterior trough (bottom).
The distance between the center of the TT and the center of the anterior bony trough was termed TT distance (Figure 2A). If the center of the anterior bony trough was located medial to the center of the TT, the TT distance was designated as negative; if the center of the anterior bony trough was located lateral to the center of the TT, the TT distance was designated as positive. Similarly, the distance between the center of the posterior bony trough and the medial border of the LFC was termed LFC distance (Figure 2B). If the center of the posterior bony trough was located medial to the center of the LFC, the LFC distance was designated as negative; if the center of the posterior bony trough was located lateral to the center of the LFC, the LFC distance was designated as positive. The TT distance and LFC distance were measured by an orthopaedic fellow (B.S.Y.) who was blinded to the extrusion of the allograft.
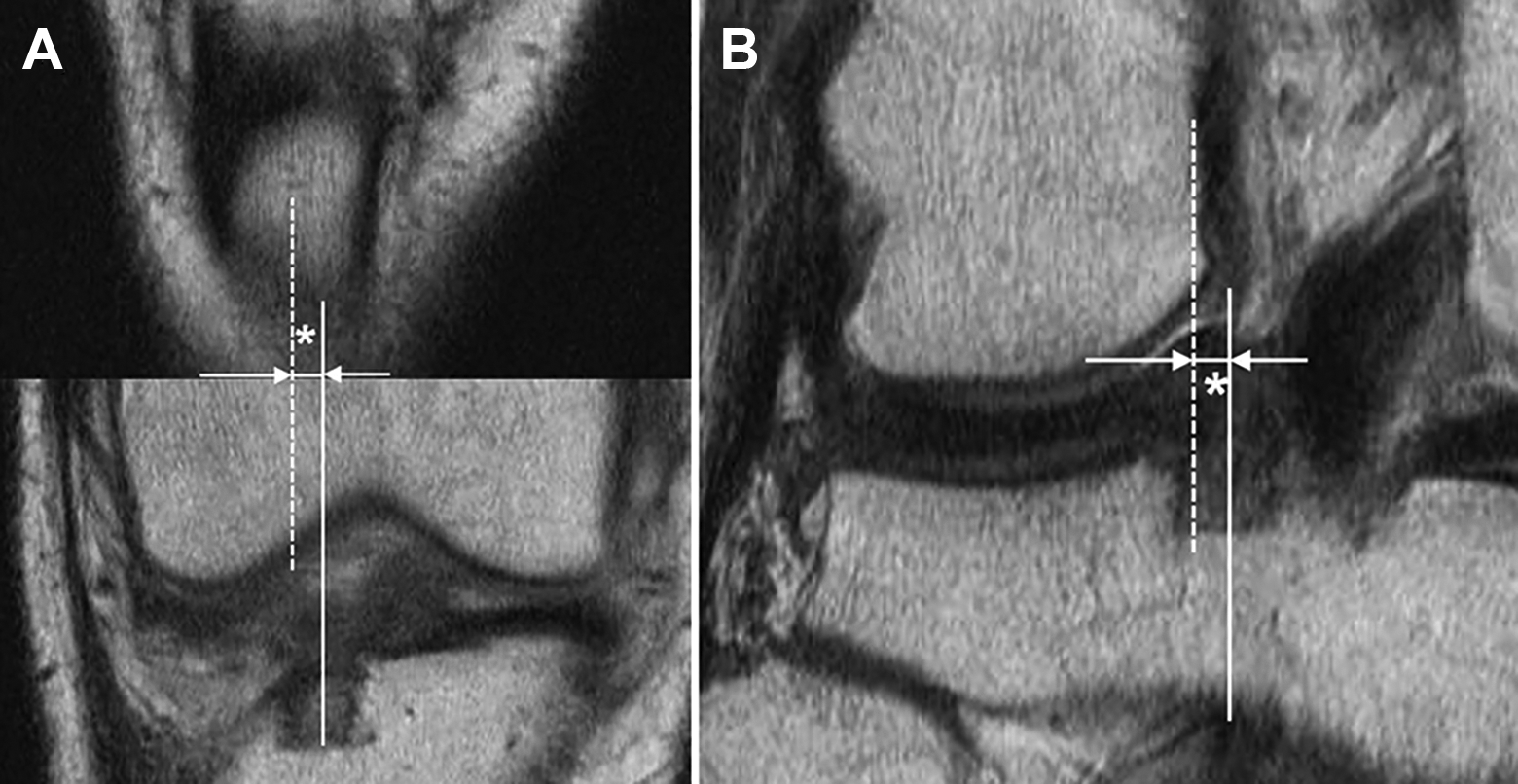
(A) A line was drawn along the center of the tibial tuberosity (dashed line), and another line was drawn along the center of the anterior bony trough (solid line); the tibial tuberosity distance was defined as the distance between the 2 lines (asterisk). (B) The same procedure was performed to measure the distance between the center of the posterior bony trough (solid line) and the medial border of the lateral femoral condyle (dashed line), defined as the lateral femoral condyle distance (asterisk).
Statistical Analysis
In a pilot study of 10 patients each from the extrusion and no-extrusion groups, the mean TT distance and LFC distance of the 2 groups were used to calculate the sample size. For a power of 0.8 and an alpha value of .05, the sample size required was 14 patients per group for TT distance and 13 for LFC distance.
The TT distance and LFC distance are reported as mean and standard deviation. The means and standard deviations of the TT distance and LFC distance were compared between the extrusion and no-extrusion groups using an independent t test because each variable showed normal distribution. A correlation analysis between extrusion and TT or LFC distance was performed. For TT distance and LFC distance, the receiver operating characteristic curve and the area under the curve (AUC) and its 95% CI were calculated. The AUC was tested by a 2-sided binomial z test with a significance level of P < .5. The optimal cutoff value was determined at the maximal Youden index. Data were analyzed using SPSS statistical software (SPSS 12.0) and G*power program (Version 3.1.5). The threshold for significance was set at P < .05.
Results
Of the 46 initial patients, 2 patients were excluded because they did not undergo follow-up MRI. Therefore, 44 patients were included in this study. The mean age of the patients was 30.8 ± 8.99 (range, 13-49) years. There were 33 (75%) male and 11 (25%) female patients. Two patients underwent concomitant ACL reconstruction, 1 patient underwent concomitant ACL and medial collateral ligament reconstruction, and 1 patient underwent posterior cruciate ligament and posterolateral corner reconstruction before MAT. The follow-up MRI examination was conducted 3.6 ± 2.8 months (range, 0.25-7.0 months) after MAT. Mean extrusion of the allograft was 2.38 ± 1.37 mm (range, 0-5.2 mm).
Among the 44 patients, 15 had extrusion and 29 had no extrusion. The mean age between the extrusion and no-extrusion groups showed no significant difference. The mean center of the anterior bony trough was in a more medial position to the center of the TT in the no-extrusion versus the extrusion group (P = .010), and the mean center of the posterior bony trough was in a more medial position to the medial border of the LFC in the no-extrusion versus the extrusion group (P = .027) (Table 1).
Age and Measurements on Follow-up Magnetic Resonance Imaging Scans for Patients With and Without Extrusion a

a Data are reported as mean ± SD (range). Boldface P values indicate statistically significant difference between groups (P < .05). LFC, lateral femoral condyle; LM, lateral meniscus; TT, tibial tuberosity.
b Defined as the distance between the center of the TT and the center of the anterior bony trough. Negative values indicate that the center of the anterior bony trough was located medial to the center of the TT; positive values indicate that the center of the anterior bony trough was located lateral to the center of the TT.
c Defined as the distance between the center of the posterior bony trough and the medial border of the LFC. Negative values indicate that the center of the posterior bony trough was located medial to the center of the LFC; positive values indicate that the center of the posterior bony trough was located lateral to the center of the LFC.
The amount of extrusion was significantly correlated with both TT distance (P = .005) and LFC distance (P = .025) (Table 2). As the anterior bony trough moved 1 mm laterally, extrusion increased by 0.4 mm. As the posterior bony trough moved 1 mm laterally, extrusion increased by 0.3 mm. The AUC (0.73; 95% CI, 0.58-0.89) for TT distance had a sensitivity of 60% and specificity of 79% to predict extrusion. The calculated cutoff value was –0.24 mm. The AUC (0.69; 95% CI, 0.53-0.85) for the LFC distance had a sensitivity of 73.3% and specificity of 62.1% to predict extrusion. The calculated cutoff value was –0.58 mm (Table 3).
Correlations Between Measurements on Magnetic Resonance Imaging Scans and Extrusion a

a Boldface P values indicate statistical significance (P < .05). LFC, lateral femoral condyle; TT, tibial tuberosity.
b Defined as the distance between the center of the TT and the center of the anterior bony trough.
c Defined as the distance between the center of the posterior bony trough and the medial border of the LFC.
AUCs and Cutoff Values of the Measurements Made on Magnetic Resonance Imaging Scans a

a AUC, area under the receiver operating characteristic curve; LFC, lateral femoral condyle; TT, tibial tuberosity.
b Defined as the distance between the center of the TT and the center of the anterior bony trough.
c Defined as the distance between the center of the posterior bony trough and the medial border of the LFC.
Discussion
The most important finding of this study was that the TT and the medial border of the LFC were important anatomic landmarks in determining the position of the anterior and posterior bony troughs during lateral MAT. The amount of extrusion was significantly correlated with both TT distance (r = 0.412; P = .005) and LFC distance (r = 0.337; P = .025). To prevent extrusion of the allograft, the center of the anterior bony trough needs to be aligned with the center of the TT, and the center of the posterior bony trough needs to be aligned with the medial border of the LFC. Our study hypothesis was confirmed.
Nonanatomic horn position increases the risk of early graft failure after lateral MAT. 7 Therefore, anatomic placement of the allograft is imperative to long-term survival of the graft after MAT. Accurate placement of the lateral meniscal allograft depends on the position of the bony bridge or keyhole. However, errors in placement of the bony bridge or keyhole during lateral MAT can occur in the coronal, sagittal, and axial planes, resulting in midbody extrusion. 3,10 In a previous study, long-term follow-up after MAT revealed a greater decrease in joint space width in the extrusion group than in the no-extrusion group. 12 Thus, a laterally placed keyhole of the allograft during lateral MAT is associated with postoperative extrusion. Choi et al 3 measured the length of the entire tibial plateau (LT) as well as the distance between the lateral edge of the lateral tibial plateau and the center of the bony bridge of the allograft (LB) on a postoperative MRI axial view. The LB-to-LT ratio was correlated with the amount of extrusion. Namely, the investigators found significantly less extrusion in patients whose meniscal transplants were positioned with LB:LT >40%. The cutoff percentage above which major extrusion did not occur was 42%. These findings demonstrated that closer positioning of the center of the bony trough to the center (50%) of the entire tibial plateau width resulted in less graft extrusion. Hence, an externally rotated allograft is associated with allograft extrusion. Lee et al 10 measured axial trough angle between a tangential line along the posterior tibial condyle and a longitudinal line along the center of the bony trough of the allograft. An increase in axial trough angle was correlated with an increase in extrusion, and the cutoff value of the axial trough angle was 5.6°. This finding indicates that a more anteriorly placed meniscal allograft can cause postoperative extrusion. Lee et al 9 measured the distance from the center of the articular cartilage of the lateral tibial condyle to the anterior border of the anterior horn of the allograft in a sagittal MRI view. Those investigators reported that this distance was correlated with extrusion, and the cutoff value was 21.5 mm for absolute extrusion.
During lateral MAT, determining the direction of the bony trough or keyhole on the axial plane is difficult. Determining the direction of the guide pin on the coronal and sagittal planes can be aided by fluoroscopy; however, making this determination on the axial plane is difficult even under fluoroscopic control. The lateral tibial spine is used as a landmark for the direction of the guide pin, 10,13,23 because both anterior and posterior horns insert to the anterior and posterior aspects of the lateral tibial spine. 6 However, a longitudinal line along the lateral tibial spine is not coincident with the line connecting the centers of both horns of the lateral meniscus. A study using tibial plateaus retrieved during total knee arthroplasty demonstrated that a wire drilled along the lateral tibial spine was 7.4° ± 9.6° internally rotated to a wire drilled along the centers of both anterior and posterior horns of the lateral meniscus. 2 A cadaveric study reported that the center of the anterior horn was located at 45.1% ± 1.3% of the tibial width, the center of the posterior horn was located at 49.8% ± 1.9% of the tibial width, and the lateral tibial spine was located at 44.4% ± 2.3% of the tibial width. 22 This study demonstrated that centers of both anterior and posterior horns insert medially to the lateral tibial spine.
Surrounding landmarks can be used to determine the center of the anterior horn during lateral MAT. Urban et al 20 reported that the anterior horn of the lateral meniscus inserted 0.48 cm lateral to the tibial midline. Johnson et al 16 reported that arthroscopic landmarks of the anterior horn of the lateral meniscus included the anterior half of the ACL tibial insertion, the lateral tibial spine, and the articular margin of the anterolateral tibial plateau. A quantitative analysis demonstrated that the center of the anterior horn of the lateral meniscus was located 14.4 ± 2.2 mm anteromedial to the apex of the lateral tibial eminence and 7.1 ± 1.3 mm anteromedial to the closest edge of the articular cartilage of the lateral tibial plateau. 7 However, the overlap of the ACL on the anterior horn root of the lateral meniscus averaged 63.2%. 7 Therefore, determining the center of the anterior horn of the lateral meniscus is very difficult without dissection of the tibial insertion of the ACL.
Few published literature describing anatomic landmarks that can be used to determine the rotational alignment of a meniscal allograft in the axial plane is available. Lee et al 8 sought to determine the presence of rotational axis during MAT. Those investigators overlapped multiple MRI axial views to identify the centers of both anterior and posterior horns of both medial and lateral menisci. A line connecting the centers of both anterior and posterior horns of each meniscus was drawn. The investigators next drew an Akagi line connecting the tibial insertion of the posterior cruciate ligament and the medial edge of the patellar tendon, 1 a line between the medial border of the patellar tendon and the apex of medial tibial spine, and a line between the lateral border of the patellar tendon and the apex of the lateral tibial spine (PTLS). The Akagi line and the PTLS were rotated internally 17.3° ± 5.5° and externally 6.1° ± 5.8° to the longitudinal line connecting the centers of both anterior and posterior horns of the lateral meniscus. The investigators found that these reference lines differed significantly from a line connecting the centers of the anterior and posterior horns in the lateral meniscus.
The present study demonstrated that the center of the TT and the medial border of the LFC can be used as anatomic landmarks to determine rotational alignment of the bony trough of the allograft. However, several other landmarks and axes, including the lateral tibial spine, Akagi line, and PTLS, should be considered in determining the rotational axis of the lateral meniscal allograft.
Limitations
There were limitations to this study. First, the sample size was small. However, the number of patients in the no-extrusion and extrusion groups was sufficient according to sample size calculation. Second, extrusion of the allograft was measured within 6 months after surgery. Extrusion may increase over time during the follow-up period. However, a serial MRI study during the first postoperative year after MAT reported that initial extrusion did not increase significantly. 11 Third, the center of the TT is not easily palpable, especially in patients with obesity.
Conclusion
To prevent extrusion of the allograft, the center of the anterior bony trough needs to be aligned with the center of the TT, and the center of the posterior bony trough needs to be aligned with the medial border of the LFC. The center of the TT and the medial border of the LFC can be used as anatomic landmarks to determine rotational alignment of the bony trough of the allograft.
Footnotes
Final revision submitted March 19, 2022; accepted May 12, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Eulji Medical Center (Eulji IRB 12-70).