
Abstract
Background:
Ice hockey referees and linesmen are at risk for musculoskeletal injuries because of the lack of protective equipment and contact with players, sticks, pucks, the ice surface and boards.
Purpose:
To quantify and analyze injuries reported by officials of the International Ice Hockey Federation (IIHF).
Study Design:
Descriptive epidemiology study.
Methods:
A 61-question survey tool was designed by an interdisciplinary team to evaluate musculoskeletal injuries experienced by ice hockey officials. This survey was administered to 600 active IIHF referees and linesmen. Only completed survey responses were included in the statistical analysis. Continuous variables were analyzed using unpaired t-tests, while categorical data were assessed utilizing chi-square tests.
Results:
Of the 600 surveys administered, 264 surveys were completed by officials from 45 countries (44% response rate). Of the respondents, 72% were male, and 28% were female, with a mean age of 31.1 ± 5.8 years. Officiating experience averaged 11.4 ± 6.0 years (6.3 ± 4.5 years with the IIHF). A total of 295 injuries were reported by 55% of the officials. Injuries occurred more frequently during games compared with training, and officials who worked year-round had more total injuries than those who took time off (P = .03). The most common injuries involved the wrist and hand (n = 64 [22%]), head and face (n = 58 [20%]), and the knee (n = 47 [16%]). Wrist and hand trauma included 23 fractures. Knee and shoulder injuries were most likely to require surgery compared with other body areas (P < .001); 30 officials underwent surgery because of an acute knee injury (10%). Injury prevention activities were effective at reducing injuries (P = .04).
Conclusion:
Most ice hockey officials experienced musculoskeletal injuries during their career. The risk of trauma to the wrist and hand can possibly be reduced via equipment modifications including protective gloves. A greater emphasis should be placed on injury prevention programs and time away from officiating competitions.
Ice hockey is considered one of the fastest and most violent contact sports, resulting in a high potential for injuries. 2,22,27 The intrinsic injury risk results from skating at speeds up to 30 mph (48 kph) with razor-sharp skate blades on an ice sheet that is confined by unyielding boards. 1,13,30 In addition, a vulcanized rubber puck travels at speeds in excess of 100 mph (161 kph). A large body of literature has detailed the incidence, type, mechanism, and severity of injuries to ice hockey players who compete in these playing conditions. 9,22,27,33 However, there is no published literature examining injuries to the officials who regulate this fast-paced collision sport.
Sports officials are often an afterthought for casual sports fans unless they disagree with a call made against their team, but ice hockey referees and linesmen are accomplished athletes. 12 These officials are required to skate at a tremendous pace to keep up with the flow of the game. There are no substitutions or line changes for officials who skate between 5 and 10 miles (8-16 km) during a game. The International Ice Hockey Federation (IIHF) has utilized a 4-official system, including 2 referees and 2 linesmen since 2008. One referee is the lead, and the other is the trail. As the flow of the game switches from one end of the ice rink to the other, the trail becomes the lead and vice versa. Referees and linesmen enforce the rules and ensure safe play for all participants on the ice.
Ice hockey officials are certainly at risk for musculoskeletal injuries owing to the lack of protective equipment and contact with players, the puck, boards, and sticks. The sports medicine community has not given ice hockey officials the same attention as players. The purpose of this study was to report on the injuries sustained by referees and linesmen working in IIHF games. Knowledge of these injury patterns will help medical personnel who cover ice hockey games and also guide future research on injury prevention for these officials. We hypothesized that the majority of ice hockey officials experience musculoskeletal injuries during their career.
Methods
After receiving institutional review board approval, we developed a questionnaire for IIHF officials based on the work of Bizzini et al 4,5 on soccer referees from the Fédération Internationale de Football Association (FIFA). The final instrument was generated by an interdisciplinary team that included orthopaedic surgeons, sports medicine physicians, athletic trainers, and ice hockey officials. The survey was also approved by the IIHF Medical Committee and Officiating Committee for use.
Unlike soccer 14 and rugby, 15 which have consensus statements on the definition of injury for their respective sports, ice hockey does not have a consensus statement on what constitutes an injury. 11 We used the IIHF’s definition of a player injury as a reportable event for officials: “any injury sustained in a practice or game that prevented the player [official] from returning to the ice; any injury sustained in training or a game that caused the player [official] to miss a subsequent training session or game; a laceration which required medical attention; all dental injuries; all concussions and all fractures.” 11,34 “Traumatic injuries” were defined as those resulting from a specific traumatic event, while “overuse injuries” referred to those not associated with a specified incident.
The 61-question survey (Supplemental Material) was distributed electronically using a secure link to rostered IIHF officials during the 2020 Winter IIHF Meeting. Responses were collected by use of independent survey software (Qualtrics). All participants provided informed consent. The first part of the survey investigated characteristics and officiating experience. The second part focused on musculoskeletal complaints and injuries sustained while training or officiating games. The third part of the survey identified preexisting medical problems (eg, high blood pressure, diabetes, etc). The final section inquired about injury prevention.
Statistical analysis was conducted utilizing SPSS Statistics Version 25 (IBM). Only completed survey responses were included in the statistical analysis. Continuous variables were analyzed utilizing unpaired t test. Categorical data were assessed using chi-square test, measuring the difference between expected and observed values. The numerical values reported indicate the mean and standard deviation unless otherwise indicated. Statistical significance was denoted as P < .05.
Results
Of the 600 active IIHF referees and linesmen who were contacted, 264 officials from 45 countries completed the survey, for a 44.0% participation rate. 19 Table 1 summarizes the participant characteristics. Of the respondents, 72.0% were male, and 28.0% were female, with a mean age of 31.1 ± 5.8 years and a mean body mass index (BMI) of 24.9 ± 5.8. Overall, 45.1% were referees, 52.3% were linesmen, and 2.7% performed both roles.
Characteristics of Participants (N = 264) a
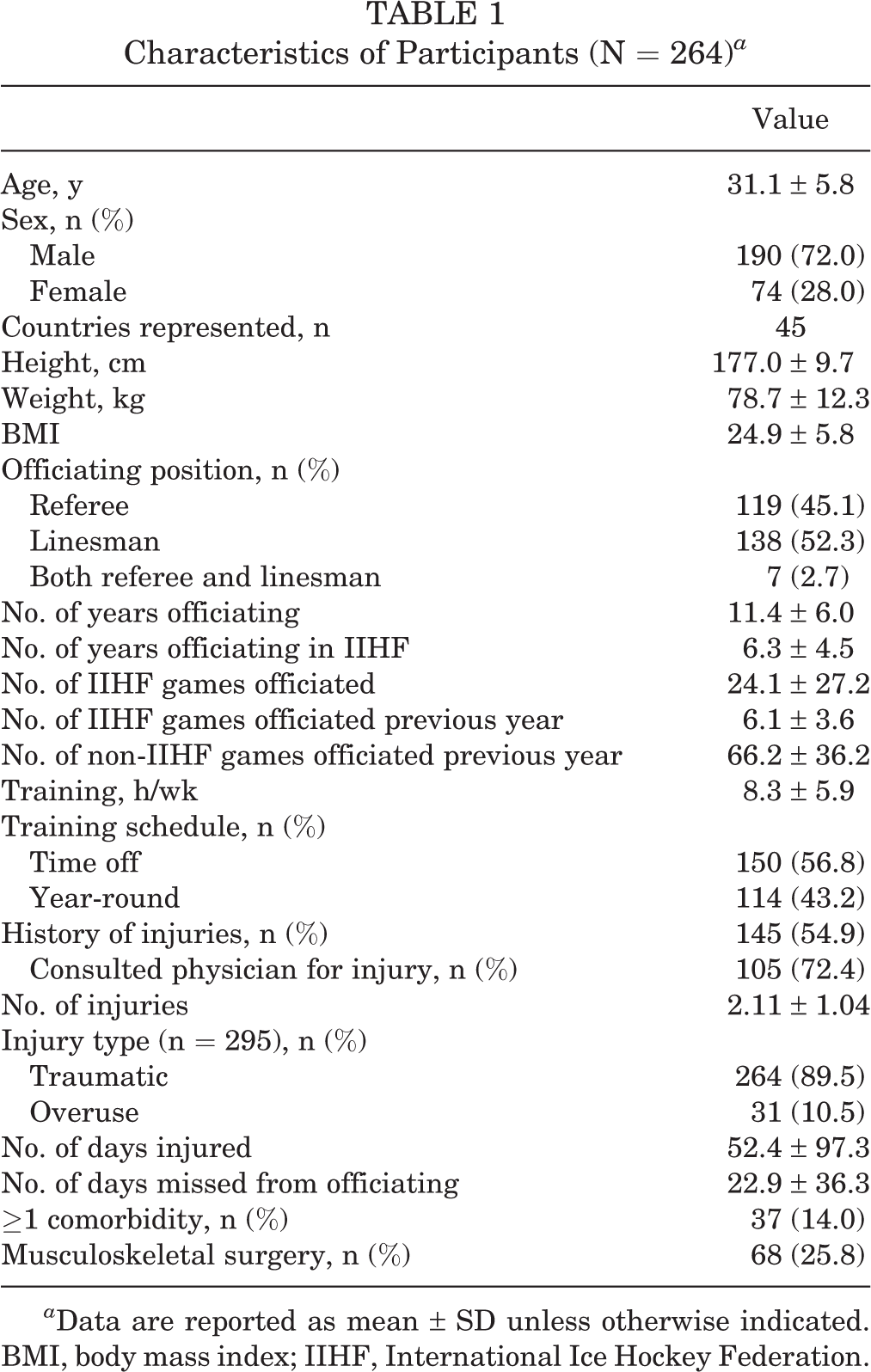
a Data are reported as mean ± SD unless otherwise indicated. BMI, body mass index; IIHF, International Ice Hockey Federation.
This was an experienced cohort of officials. The mean number of years officiating was 11.4 years, including 6.3 years with the IIHF. The mean number of IIHF games officiated was 24.1, including 6.1 games during the 2019 IIHF season. Overall, 54.9% (n = 145) of officials reported a history of injuries because of officiating games or training. These officials reported a total of 295 injuries, of which 89.5% (n = 264) were traumatic and 10.5% (n = 31) occurred from overuse. Additionally, 72.4% (n = 105) of these officials sought the care of a physician for their injury. On average, they missed 22.9 days from officiating with each injury.
Further, 14.0% (n = 37) of officials reported at least 1 medical comorbidity, which included seasonal allergies (n = 15), asthma (n = 10), hypertension (n = 6), kidney disease (n = 2), diabetes (n = 2), hypothyroidism (n = 1), and bradycardia (n = 1). Notably, 25.8% (n = 68) of officials required musculoskeletal surgery, and 43 surgical procedures were a direct result of an injury sustained while officiating on the ice.
Comparison of Referees and Linesmen
Table 2 summarizes the respondent characteristics by sex and officiating position. The mean age of male referees (n = 100) was 33.9 years, and the mean BMI was 25.9. They had a mean of 13.3 years of officiating experience, with 7.42 years of officiating with the IIHF. The mean age of male linesmen (n = 90) was 29.5 years, with a mean BMI of 25.2, a mean of 10.8 years of officiating experience, and 5.77 years of officiating with the IIHF. Of all male officials (combined referees and linesmen), 55.0% reported an injury in their career, for a mean of 2.12 injuries per official.
Comparison by Sex and Officiating Position a
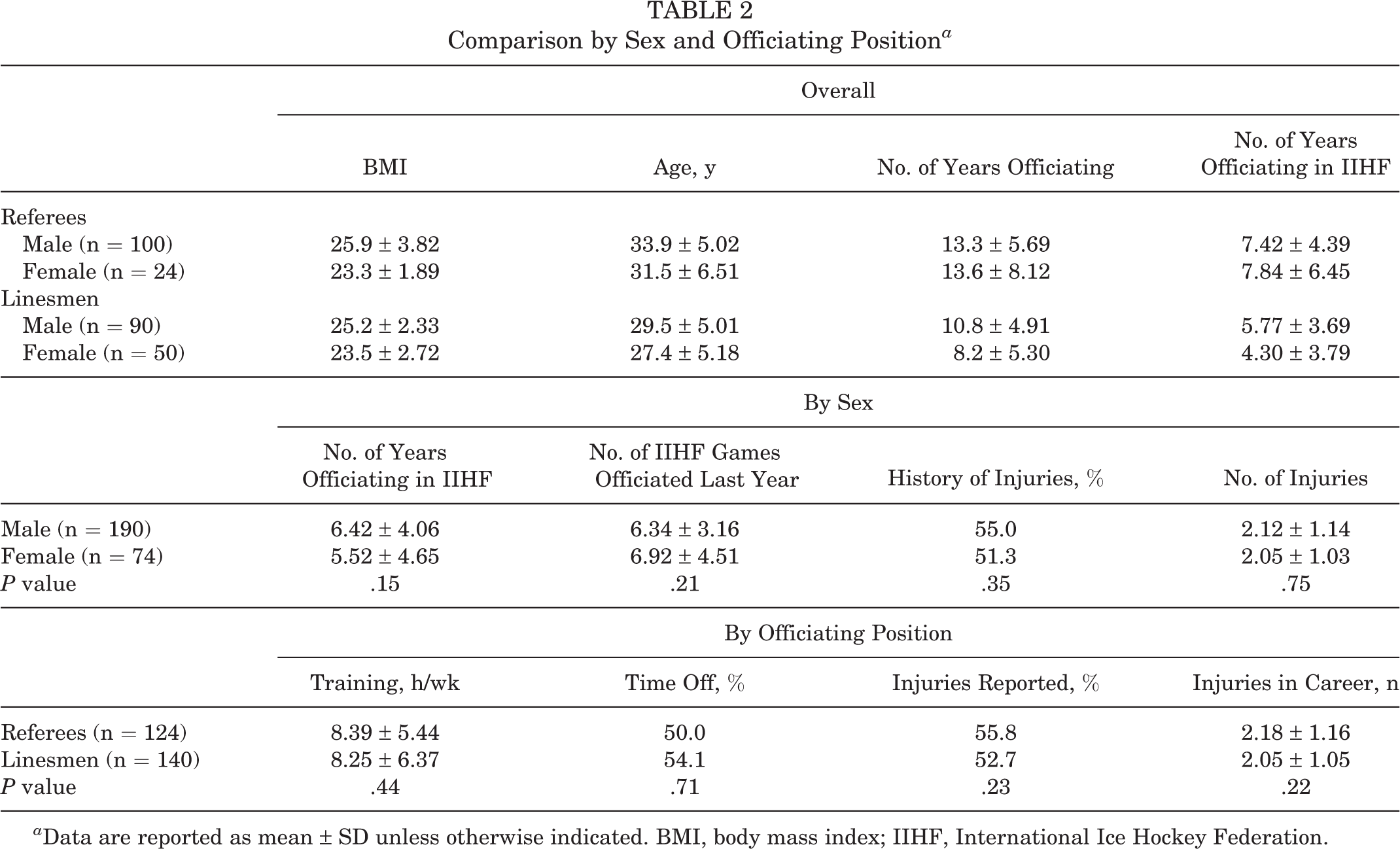
a Data are reported as mean ± SD unless otherwise indicated. BMI, body mass index; IIHF, International Ice Hockey Federation.
The mean age of female referees (n = 24) was 31.5 ± 6.51 years, and the mean BMI was 23.3 ± 1.89. They reported a mean of 13.6 ± 8.12 years of officiating experience, with 7.84 ± 6.45 years of experience working IIHF tournaments. Female linesmen (n = 50) had a younger mean age than female referees at 27.4 ± 5.18 years and a mean BMI of 23.5 ± 2.72. They reported 8.2 ± 5.30 years of officiating experience, with 4.30 ± 3.79 years officiating in IIHF games. Overall, 51.3% of female officials reported an injury, with a mean 2.05 ± 1.03 reported injuries.
No difference in the number of injuries was noted when comparing male versus female officials (2.12 ± 1.14 vs 2.05 ± 1.03 injuries, respectively; P = .75) or when comparing referees to linesmen (2.18 ± 1.16 vs 2.05 ± 1.05 injuries, respectively; P = .22) (Table 2). When stratified by age, officials aged ≥30 years had a significantly larger number of reported injuries than those aged <30 years (2.22 ± 1.19 vs 1.93 ± 1.08 injuries, respectively; P = .047). However, when stratified by BMI, there was no difference in the number of injuries between officials with a normal BMI, defined as <25, and those with an elevated BMI (2.10 ± 1.07 vs 2.14 ± 1.15 injuries, respectively; P = .41) (Table 3).
Effect of Age and BMI on Injuries a
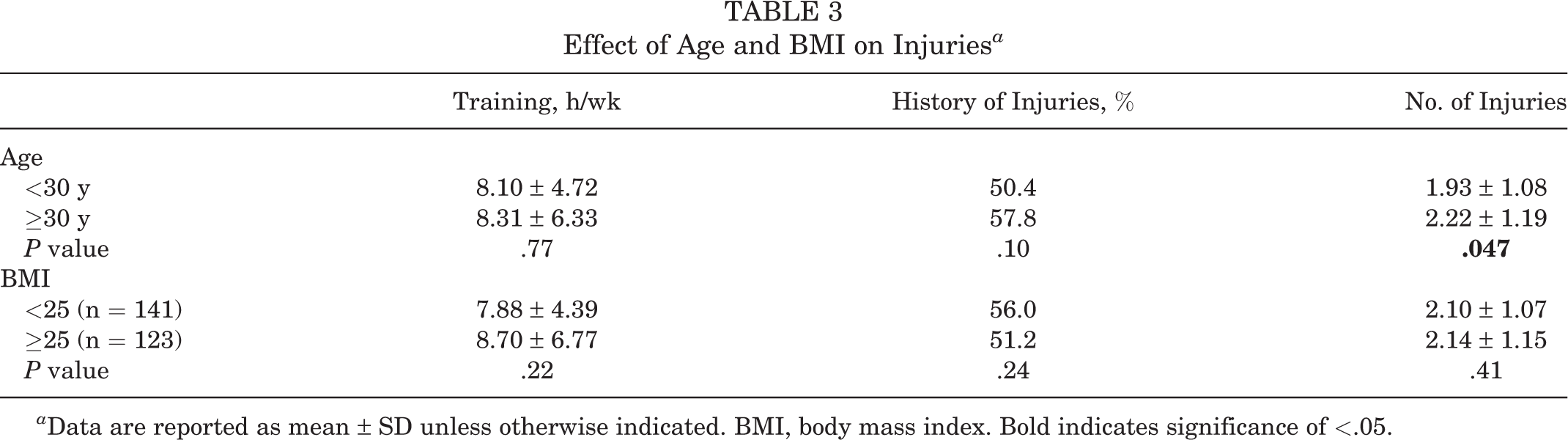
a Data are reported as mean ± SD unless otherwise indicated. BMI, body mass index. Bold indicates significance of <.05.
Injuries by Body Area
The 295 reported injuries were divided into 9 categories according to the area of injury (dental; wrist and hand; head and face; chest and stomach; knee and leg; groin, hip, and pelvis; back; foot and ankle; and shoulder and elbow) (Figure 1 and Table 4). Injuries to the wrist/hand were the most common (n = 64), followed by the head/face (concussions and lacerations, n = 58) and knee/lower leg (n = 47). There were 43 reported surgeries; 30 of the surgical procedures involved the knee, 12 surgical procedures were performed on the shoulder and elbow, and there was 1 hip procedure. A knee or shoulder injury had the highest likelihood of requiring surgery compared with the remaining body areas (P < .001).

Injury breakdown by body area for survey respondents.
Injuries According to Body Area (n = 295) a
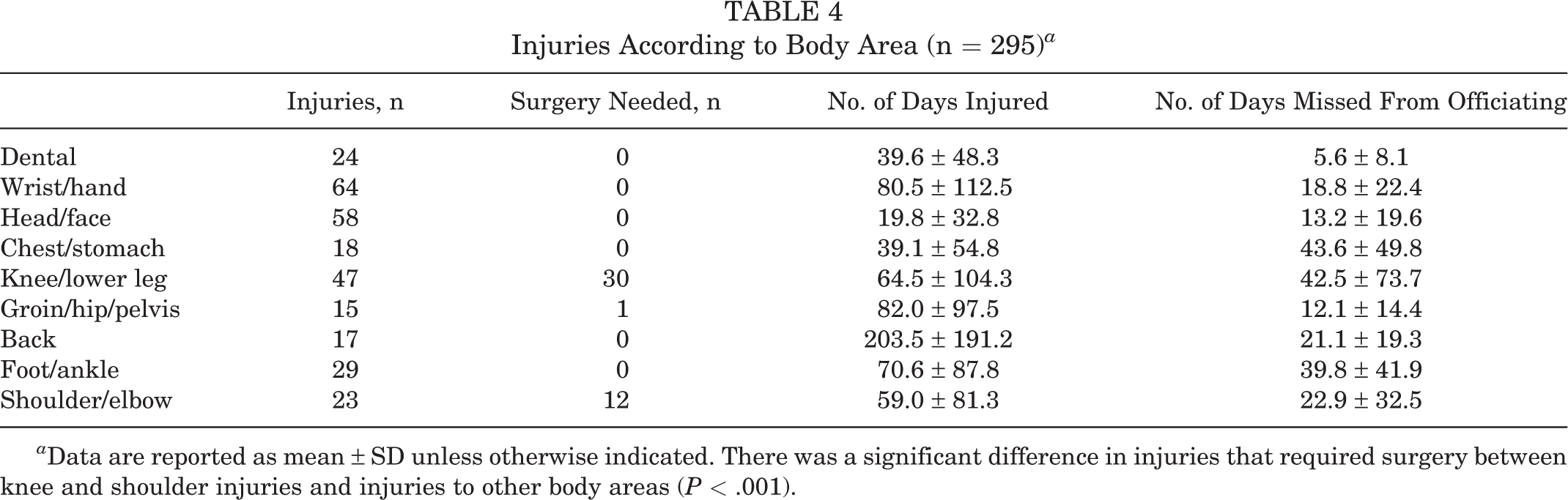
a Data are reported as mean ± SD unless otherwise indicated. There was a significant difference in injuries that required surgery between knee and shoulder injuries and injuries to other body areas (P < .001).
Wrist and hand injuries (Table 5) included 23 fractures (35.9%), 16 contusions (25.0%), 8 lacerations (12.5%), 5 dislocations (7.8%), 5 ligament or tendon injuries (7.8%), and 7 categorized as other (10.9%).
Types of Wrist/Hand Injuries (n = 64)

Injury Prevention Activities
Referees and linesmen both made injury prevention a priority, with 88.6% of surveyed officials engaging in injury prevention activities. Only 30 (11.4%) of the surveyed officials did not do anything specific to minimize injuries on the job. More than half (n = 144 [54.5%]) of the surveyed officials participated in a stretching or flexibility program to help minimize injuries, an almost equal number utilized a personal trainer (n = 35 [13.3%]) or physical therapist (n = 36 [13.6%]), and 19 officials (7.2%) made use of massage therapy as an injury prevention option.
There was a significant difference in the number of injuries according to the training schedule. Officials who took time off from training had significantly fewer injuries than those who trained year-round (2.01 ± 1.05 vs 2.27 ± 1.18 injuries, respectively; P = .031). However, 50.9% of officials who trained for <10 h/wk sustained an injury compared with only 40.5% of officials who trained for ≥10 h/wk (P = .026) (Table 6).
Injuries According to Injury Prevention and Training a

a Data are reported as mean ± SD unless otherwise indicated. Boldface P values indicate a statistically significant difference between groups (P < .05).
Discussion
Ultimately, 54.9% (n = 145) of surveyed IIHF officials reported an injury, of which 89.5% (n = 264) were traumatic and 10.5% (n = 31) occurred from overuse. Additionally, 72.4% (n = 105) sought care from a physician for their injury. On average, officials missed 22.9 ± 36.3 days from competition with each injury. The most common injuries involved the wrist and hand (21.7% [n = 64]), head/face (19.7% [n = 58]), and the knee (15.9% [n = 47]). Wrist and hand trauma included 23 fractures. Knee and shoulder injuries were most likely to require surgery (P < .001). Further, 30 (10.2%) surgical procedures were needed because of an acute knee injury. Injury prevention was effective for risk reduction (P = .043). Referees and linesmen who worked year-round had more injuries than those who took time off (P = .031).
Our survey investigated musculoskeletal injuries in a cohort of IIHF referees and linesmen from 45 different countries. These ice hockey officials were younger (mean age, 31.1 ± 5.8 years) than referees in elite soccer and Gaelic football. 4,6,23,29 The mean BMI (24.9 ± 5.8) of the surveyed ice hockey officials was similar to that in previous studies of soccer officials (mean, 23-26). 4,21,23,29 A BMI of 25 has been used in previous work to correlate with performance and health in officials. 8
IIHF referees and linesmen demonstrated a 54.9% career injury prevalence in our study, slightly higher than what has been reported for referees in elite soccer leagues. 4 Bizzini et al, 4 in a study of top-level Swiss soccer referees, found a 40% career injury prevalence in their surveyed officials. Another study of female soccer officials, looking at referees and assistant referees at the 2007 FIFA Women's World Cup, found a 48% career incidence of injuries. 3 The annual injury rate was reported as 58% for Gaelic football officials, 52% for hurling officials, and 42% for officials covering both sports. 6
The anatomic locations and types of injuries in our study were unexpected and did not follow the findings of any previous studies on referees. The most frequently reported injuries were to the wrist, hand, and finger (n = 64), followed by injuries to the head/face (concussions, lacerations; n = 58) and injuries to the knee/leg (n = 47). In a study of top-level Croatian soccer officials, calf strains and ankle sprains were the most common injuries during competition, with quadriceps and hamstring strains occurring during fitness training. 17 Gaelic sports officials had a high injury rate in the lower limbs, with hamstring and calf strains being the most commonly reported. 6 In a study of Swiss soccer officials, hamstring strains and ankle sprains were the most commonly reported injuries. 4
The injury breakdown reported by the officials in this study was also inconsistent with published research on injuries in ice hockey players. A recent epidemiology study looking at Swiss ice hockey teams found the most injuries to involve the hip and groin, followed by concussions. 7 A study of ice hockey players at the IIHF World U20 and U18 Championships identified a high percentage of head/face injuries (lacerations and concussions) in the U20 group. 34 The shoulder was the most commonly injured area in the U18 group. 34 Concussions were the most common National Collegiate Athletic Association men’s hockey injuries, followed by medial collateral ligament sprains and acromioclavicular joint contusions. 13 Another study of ice hockey injuries from the IIHF Men’s World Championships and Olympic Games identified injuries to the head/face, medial collateral ligament, and acromioclavicular joint as the most common body regions. 33
The most straightforward explanation for the high incidence of hand and wrist injuries in the officials in our study is the lack of protective gloves during competition. The most common hand or wrist injury was a fracture (Table 5). The literature on hand and wrist injuries in ice hockey is limited. 2,18,25,31 Finger contusions and wrist sprains were reported in an epidemiology study of men’s and women’s collegiate hockey players. 25 Another study found that hand, wrist, and elbow injuries comprised roughly 14% of hockey-related visits to the emergency department. 10
A high percentage of knee injuries (63.8%) in our series required surgery (n = 30). Previous work on Premier League soccer referees found that 81% of officials sustained a knee injury at some point during their career. 23 Further research to determine the exact mechanism and type of knee injuries can help guide prevention strategies.
More than half of IIHF officials engaged in injury prevention activities, including a stretching or flexibility program, use of a personal trainer, physical therapy, and massage therapy. The IIHF referees who did not engage in injury prevention activities were more likely to sustain an injury (65.5% vs 50.9%, respectively; P = .043). Furthermore, ice hockey officials who worked year-round without time off had more injuries than those who took dedicated breaks (2.27 ± 1.18 vs 2.01 ± 1.05 injuries, respectively; P = .031). The dangers of specialization and overtraining are well documented in the literature. 26,28,38 The number of weekly training hours also affected the injury risk, as 50.9% of officials who worked out for <10 h/wk sustained an injury as opposed to 40.5% of officials who worked out for ≥10 h/wk (P = .026). Injury prevention strategies and taking time off from officiating may help to reduce the injury risk. Some of these injury prevention tactics have been reported in other studies involving soccer referees. 4
Notably, only 72.4% (n = 105) of injured officials (n = 145) sought care from a physician for their injuries. This may be because of officials receiving care from athletic trainers or other members of the medical staff. However, this may also indicate barriers to officials accessing care from physicians. While professional and international ice hockey teams often work closely with a designated team physician, ice hockey officials are not provided with a designated physician. This is a potential area for improvement with the development of a protocol for injured officials to undergo an evaluation by a physician. The IIHF has recommended adding officials to its Injury Reporting System, which may improve injury identification and access to care. Additionally, the IIHF may consider recruitment of an additional physician to provide medical care for officials during IIHF events.
Limitations
There are limitations to this study. First, the overall participation rate was lower than desired at 44.0% (264/600). Although response rates of ≥70% are desirable for external validity, a lower response rate may be acceptable. 32 Visser et al 37 demonstrated that studies with response rates as low as 20% provided more accurate results than studies with response rates of 60% to 70%. A recent cohort study demonstrated that, despite low response rates (18%-60%) and different data collection methods, results were remarkably consistent. 24 Still, this represents the second largest study on officials in the literature, as Gabrilo et al 17 reported on 342 Croatian soccer referees. A language barrier may have contributed to the lower response rate, as the survey was only available in English. Second, the retrospective design could have introduced recall bias. Several publications have questioned the accuracy of self-reported injury studies. 4,20,36 A comparison of prospective and retrospective injury studies in Australian rules football over a 12-month period showed that recall accuracy significantly declines at 1 year. 16 Only 80% of the athletes were able to remember the number of injuries and the particular body parts involved. A comparison of prospective surveillance with retrospective recall in physical education students in the Netherlands found that participants did not recall >50% of their recorded injuries. 35 This would seem to suggest that the present study likely underestimated the true number of injuries in ice hockey officials. Third, we did not specifically define time away from year-round training in the survey question. The individual interpretation of the question could have resulted in a wide range of values from a couple of weeks to a couple of months. This applied specifically to the injury risk for officials who trained and worked year-round without any dedicated time away from the sport. Last, it is possible that some officials did not disclose an injury to avoid the loss of IIHF officiating opportunities.
Conclusion
The majority of ice hockey officials experienced musculoskeletal injuries during their career. Knowledge of injury patterns in ice hockey officials will help medical personnel diagnose and treat injuries in this unique population and guide future research on injury prevention. The risk of trauma to the wrist and hand could possibly be reduced via equipment modifications including protective gloves. A greater emphasis should be placed on injury prevention programs, and officials should be encouraged to intermittently take time away from the ice. We support the IIHF recommendation to add officials to its Injury Reporting System.
Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671221117504.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221117504 - Injuries to Ice Hockey Referees and Linesmen: A Survey of International Ice Hockey Federation Officials
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221117504 for Injuries to Ice Hockey Referees and Linesmen: A Survey of International Ice Hockey Federation Officials by Charles A. Popkin, Thomas A. Fortney, Ajay S. Padaki, Andrew J. Rogers, David P. Trofa, T. Sean Lynch, Markku Tuominen and Michael J. Stuart in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgment
The authors acknowledge and thank the IIHF Officiating and Medical Committees for their help and support in making this study possible. The authors also highly appreciate the cooperation of all the referees and linesmen in the IIHF who took the time to complete the survey.
Final revision submitted March 12, 2022; accepted May 17, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.A.P. has received research support and education payments from Arthrex. A.J.R. has received education payments from Arthrex; consulting fees from DePuy/Medical Device Business Services, Linvatec, and Smith & Nephew; speaking fees from Arthrex; and hospitality payments from Stryker. D.P.T. has received research support from Arthrex and education payments from Arthrex and Smith & Nephew. T.S.L. has received educational support from Linvatec and Smith & Nephew and consulting fees from KCI and Smith & Nephew. M.J.S. has received research support from Stryker and consulting fees, speaking fees, and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Columbia University (protocol No. AAAR2657).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.