
Abstract
Background:
Patella alta and elevated tibial tubercle–trochlear groove (TT-TG) distance can predispose patients to lateral patellar dislocations and recurrent instability. Their influence on patient-reported outcomes (PROs) after medial patellofemoral ligament (MPFL) reconstruction is less clear.
Hypothesis:
We hypothesized that neither moderately increased TT-TG distance nor patella alta would negatively affect PROs after isolated MPFL reconstruction in patients with relatively normal patellar tracking (no large J-sign).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We identified patients who underwent isolated MPFL reconstruction at a single institution between 2008 and 2016. The decision to perform an isolated MPFL reconstruction was at the discretion of the operating surgeon but was not performed in the setting of a large J-sign. Patient characteristics and surgical details were collected, and patients completed the Norwich Patellar Instability Score, Knee injury and Osteoarthritis Outcome Score, and Marx activity score. Patellar height (Caton-Deschamps Index [CDI]) was assessed on preoperative lateral radiographs, and TT-TG distance was measured on preoperative axial magnetic resonance imaging (MRI) scans. Patients were grouped based on CDI and TT-TG distance, and outcomes were compared. Linear regression modeling was performed to determine whether patella alta or elevated TT-TG distance was associated with poorer PRO scores.
Results:
Of 165 knees in 152 patients who underwent isolated MPFL reconstruction, 115 patients (125 knees; 76%) with minimum 1-year follow-up were contacted at a mean of 5.2 years after surgery. Recurrent dislocation occurred in 5 of 125 knees (4%). Preoperative radiographs were available in 111 knees (89%), and preoperative MRI scans were available in 89 knees (71%). Mean CDI was 1.13, and 35% had a CDI ≥1.20. Mean TT-TG distance was 17.5 mm, and 26% had a TT-TG distance >20 mm. After adjusting for patient age, sex, body mass index, and graft choice, we observed that neither patella alta nor elevated TT-TG distance were associated with poorer PROs.
Conclusion:
Isolated MPFL reconstruction in the setting of moderately elevated TT-TG distance or patella alta was not associated with worse PROs in this cohort with relatively normal patellar tracking (no large J-sign).
Patellar dislocations are relatively common knee injuries that often affect a young, active patient population. Recurrent episodes of patellar instability can result in pain, decreased function, and patellofemoral arthritis. Surgical treatment with medial patellofemoral ligament (MPFL) reconstruction is indicated in many patients with recurrent patellar instability. 18 The procedure can be performed either in isolation or in combination with other surgical procedures to restore knee stability.
There are multiple osseous abnormalities, such as trochlear dysplasia, 3,6,7 patella alta, 8,21,25 and increased tibial tubercle–trochlear groove (TT-TG) distance, 16 that can predispose patients to patellar instability. Normally, the patella engages the trochlear groove as the knee is flexed beyond 30°. 3 Patella alta refers to a high position of the patella. As a result of this high position, the patella does not engage the trochlear groove until later in knee flexion, increasing the risk of lateral patellar dislocation. 8,21,25 In cases of dysplasia, the trochlea is abnormally shallow, which results in decreased resistance to lateral patellar translation. 3,6,7 Increased TT-TG distance is another anatomic variation that increases the risk of patellar dislocation by increasing the lateral vector of pull of the extensor mechanism.
Isolated MPFL reconstruction has been shown to yield excellent outcomes in the majority of patients with patellofemoral instability 18 ; however, there are some patients with altered osseous anatomy in whom the addition of a bony procedure is indicated. 16 Tibial tubercle osteotomies are effective at improving patellar stability but do introduce increased complication risk, including nonunion of osteotomy site, persistent anterior knee pain, and potential vascular injury. 16,26 Consequently, there has been ongoing research investigating the outcomes of isolated MPFL reconstruction in more borderline clinical situations.
Several authors have investigated the effect of patella alta and increased TT-TG distance on the risk of recurrent instability after isolated MPFL reconstruction. 2,17,18 However, there has been less work published regarding the effect of these factors on patient-reported outcomes (PROs) after isolated MPFL reconstruction. Evaluating the effect of patellar height and TT-TG distance on PROs after isolated MPFL reconstruction is key, as it will better clarify the outcomes of isolated MPFL reconstruction in patients with anatomy that, historically, has been treated with tibial tubercle osteotomy.
The purpose of this study was to evaluate the influence of preoperative imaging measurements (TT-TG distance and patellar height) on PROs and recurrent dislocation risk after isolated MPFL reconstruction. We hypothesized that neither moderately increased TT-TG distance (>20 mm) nor patella alta (Caton-Deschamps Index [CDI] >1.20) would negatively affect PROs after isolated MPFL reconstruction in patients with relatively normal patellar tracking (no large J-sign).
Methods
Study Design and Evaluation Methods
After receiving institutional review board approval, we performed a retrospective review to identify patients who underwent primary MPFL reconstruction for recurrent patellar instability at our institution between 2008 and 2016. Recurrent patellar instability was defined as ≥2 patellar dislocations or persistent symptoms of patellar subluxation and instability with a positive patellar apprehension test after nonoperative treatment of a first-time patellar dislocation. Routine operative treatment of first-time patellar dislocations was not performed during this period, and no acute first-time dislocations were included in this study. Patients in whom a tibial tubercle osteotomy or additional bony procedure was performed were excluded. Although the decision to proceed with a tibial tubercle osteotomy was ultimately made by the surgeon and patient, general indications for tibial tubercle osteotomy in the study period included the presence of a large J-sign in association with an elevated TT-TG distance (>20 mm) and/or significant patella alta (CDI >1.30). No age-based exclusion criteria were used, but all patients treated surgically at this institution are aged ≥13 years. No physeal-sparing procedures were included.
Chart review was performed to collect patient descriptive information and details of the surgical procedures plus any concomitant procedures. Preoperative imaging was reviewed in available patients. Patellar height was assessed using the CDI on lateral plain radiographs at 30° of knee flexion. 4 Trochlear dysplasia was evaluated on magnetic resonance imaging (MRI) scans via sulcus angle measurement, 5 and TT-TG distance was measured on MRI scans using the Schöttle method. 19 Articular cartilage status of the patellofemoral compartment was assessed at arthroscopy using the modified Outerbridge classification system. 13
Patients were contacted via mail and telephone to collect PRO measures (PROMs). Patellar instability was assessed according to Norwich Patellar Instability Score (NPI). 22 Pain, symptoms, function, and quality of life were assessed via the Knee injury and Osteoarthritis Outcome Score (KOOS). 15 Activity level in the past year was evaluated using the Marx activity score. 11
Patient Population
Chart review identified 201 knees in 185 patients who underwent primary MPFL reconstruction between 2008 and 2016. Of these 201 knees, 36 were excluded because a tibial tubercle osteotomy was performed in conjunction with the MPFL reconstruction. Thus, 165 isolated MPFL reconstructions in 152 patients with recurrent patellar instability were eligible for study inclusion. Of these eligible patients, 115 (125 knees; 76%) with minimum 1-year follow-up were contacted at a mean of 5.2 years after surgery and assessed for recurrent instability events. PROMs were completed by 89 eligible patients (95 knees; 58%) (Figure 1).

Flowchart of patient inclusion in the study. MPFL, medial patellofemoral ligament; PROM, patient reported outcome measures.
Surgical Technique
All patients who experienced recurrent patellar instability during this period were treated with MPFL reconstruction with a tibial tubercle osteotomy performed at the discretion of the surgeon. Procedures were performed by 4 sports medicine fellowship-trained orthopaedic surgeons (including D.C.F., R.A.M. and C.K.K.). In all cases, the procedure began with diagnostic arthroscopy, and any intra-articular pathology, including meniscal and chondral lesions, was addressed at this time. MPFL reconstruction was performed according to the general principles of anatomic graft placement without graft tension. Femoral tunnel position was determined using anatomic (at the saddle between the medial epicondyle and adductor tubercle) and/or radiographic (Schöttle point) landmarks, and patellar attachment was performed on the proximal half of the patella. 20 Patellar fixation was achieved using 1 or 2 anchors, and femoral fixation was performed using an interference screw. Specific graft type varied with time and surgeon and included autograft hamstring tendon and allograft tissue (hamstring tendon, peroneus longus tendon, and tibialis anterior tendon).
Rehabilitation Protocol
All patients were instructed to initiate formal physical therapy within 1 week of surgery. Treatment consisted of superior and medial patellar glides, quadriceps, hamstrings, core and hip abductor strengthening, active and passive range of motion exercises from 0° to 90° of flexion, and gait retraining. Brace use and weightbearing restrictions after surgery varied by surgeon and over time. A corresponding home exercise program was also executed to supplement the above-mentioned treatment.
Statistical Analysis
Summary statistics (means, standard deviations, and proportions) were calculated for patient characteristics and outcomes. Patients were grouped based on patellar height and TT-TG distances for comparisons of outcomes. The effect of patellar height on outcomes was evaluated using 2 separate thresholds for patella alta. First, patients were grouped based on CDI ≥1.20 versus <1.20. Patients were then grouped based on CDI ≥1.30 versus <1.30 to evaluate the effect of more severe patella alta. Patients were also grouped based on TT-TG distance >20 versus ≤20 mm. Failure risk based on these groupings was compared using the Fisher exact test. PROs were compared using independent-samples t tests after confirmation that sample distributions were normal using the Kolmogorov-Smirnov test. Linear regression modeling was then performed to determine whether patella alta or elevated TT-TG distance was associated with poorer PRO scores, adjusting for patient age, sex, BMI, and graft choice.
A power analysis demonstrated that 80% power would to be achieved to detect a clinically important 10-point difference in KOOS scores with an expected standard deviation of 15 points by including a total of 64 patients with an expected 2:1 distribution between the patella alta/elevated TT-TG distance group and the normal anatomy group (α = .05). All statistical tests were performed with STATA 13.1 (StataCorp, College Station, TX).
Results
Overall, 34 knees (27.2%) underwent reconstruction using autograft, and 91 knees (72.8%) underwent reconstruction using allograft. Of the 125 knees with minimum 1-year follow-up, 45 were from male patients, and 80 were from female patients. The mean patient age at surgery was 24.5 years (range, 13-57 years). Recurrent patellar dislocations occurred in 5 of the 125 total knees (4.0%) with 1-year minimum follow-up during the study period.
Preoperative radiographs were available in 111 knees (89%). The mean CDI for all knees was 1.13. Overall, 39 knees (35%) had a CDI ≥1.20 (including 21 knees [19%] with a CDI ≥1.30), and the remaining 72 knees had a CDI <1.20. Preoperative MRI scans were available in 89 patients (71%). The mean sulcus angle was 144.5°, and the mean TT-TG distance was 17.5 mm. A total of 23 knees (26%) had a TT-TG distance >20 mm, and the remaining 66 knees had a TT-TG distance ≤20 mm. There were only 3 patients with CDI >1.40 and 3 patients with a TT-TG distance >24 mm. Articular cartilage damage of Outerbridge 3 or 4 was noted on the patella in 56 knees (50.4%) and on the trochlea in 8 knees (7.2%). Most lesions were noted to be medial on the patella and lateral on the trochlea. Patient characteristics, articular cartilage status, graft choice, and other preoperative anatomic measurements were similar in those with increased CDI and TT-TG distance compared with those with normal values (Table 1).
Patient Characteristics and Graft Choice Based on Preoperative Patellofemoral Anatomy a
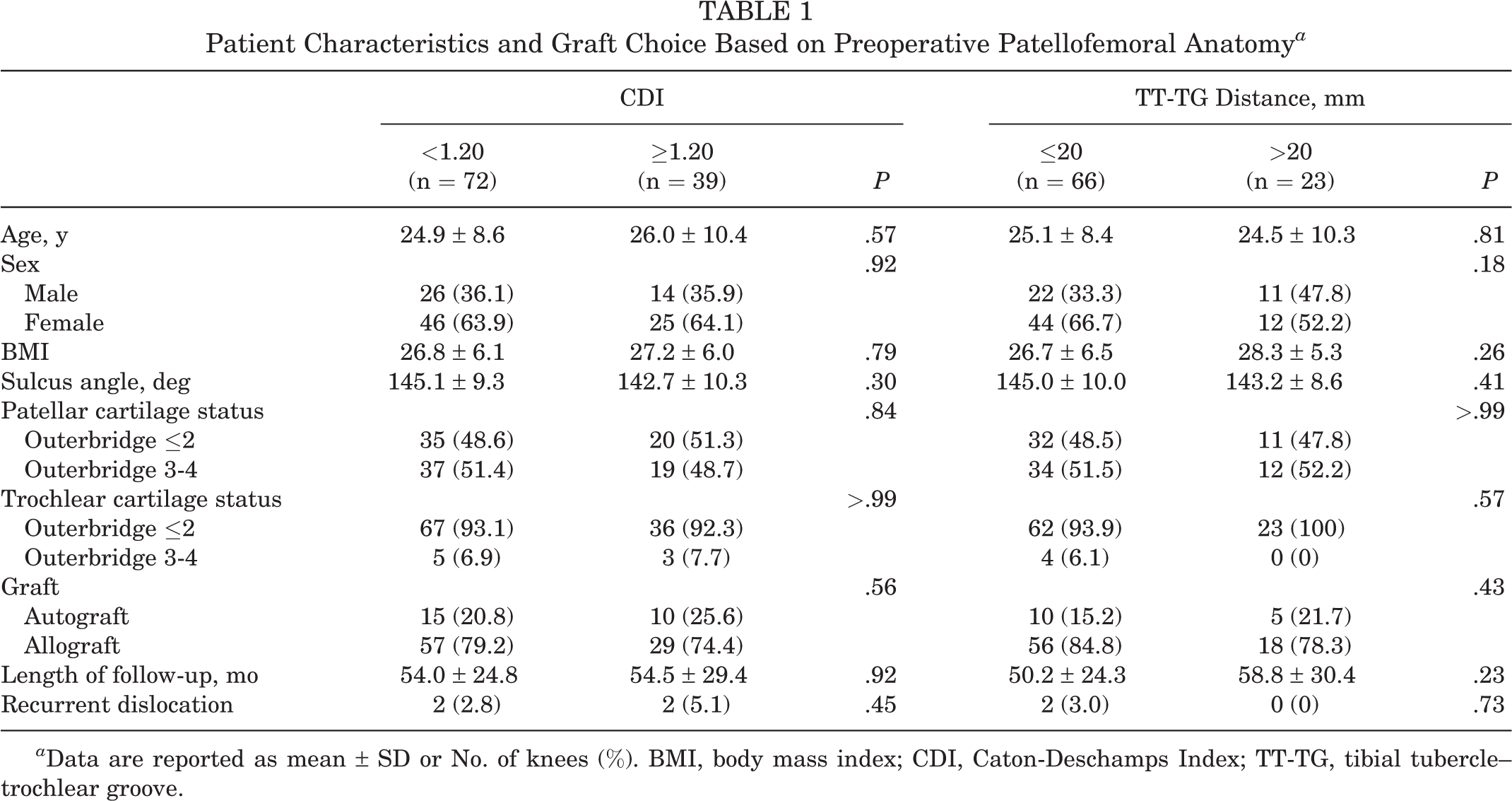
a Data are reported as mean ± SD or No. of knees (%). BMI, body mass index; CDI, Caton-Deschamps Index; TT-TG, tibial tubercle–trochlear groove.
Of the 111 knees with preoperative radiographs, 4 (3.6%) experienced repeat dislocations during the study period. Two cases of recurrent patellar dislocation occurred in knees with CDI ≤1.20, and 2 cases occurred in knees with CDI >1.20 (P = .45). Of the 89 knees with preoperative MRI scans, 2 (2.2%) experienced repeat dislocations during the study period. Two recurrent dislocation events occurred in the knees with TT-TG ≤20 mm group, and none occurred in knees with TT-TG >20 mm (P = .73).
PROMs were completed for 89 knees with preoperative radiographs and 71 knees with preoperative MRI scans. There were 59 knees in the CDI ≤1.20 group and 30 knees in the CDI >1.20 group (including 16 with a CDI ≥1.30). There were 52 knees in the TT-TG ≤20 mm group and 19 knees in the TT-TG >20 mm group. No PROs were noted to be lower in the groups with elevated CDI or TT-TG distance (Table 2). Knees with a CDI >1.20 demonstrated a slightly increased Marx activity level compared with those with CDI ≤1.20 (P = .042). Knees with a TT-TG distance >20 mm had less patellar instability according to the NPI (P = .038).
Patient-Reported Outcomes Based on CDI (n = 89 Knees) and TT-TG Distance (n = 71 Knees) a

a Data are reported as mean ± SD. Boldface P values indicate statistically significant comparison (P < .05). ADL, Activities of Daily Living; CDI, Caton-Deschamps Index; KOOS, Knee injury and Osteoarthritis Outcome Score; NPI, Norwich Patellar Instability Score; QoL, Quality of Life; Sport/Rec, Sport and Recreation; TT-TG, tibial tubercle–trochlear groove.
Multiple linear regression analysis demonstrated little correlation between the CDI and PRO scores after MPFL reconstruction, adjusting for patient age, sex, BMI, and MPFL graft choice (Table 3). There was no correlation between CDI and any PROM. Elevated TT-TG distance was noted to correlate with lower pain on the KOOS Pain subscale (P = .025) but no other PROMs.
Regression Analysis of Patient-Reported Outcomes a
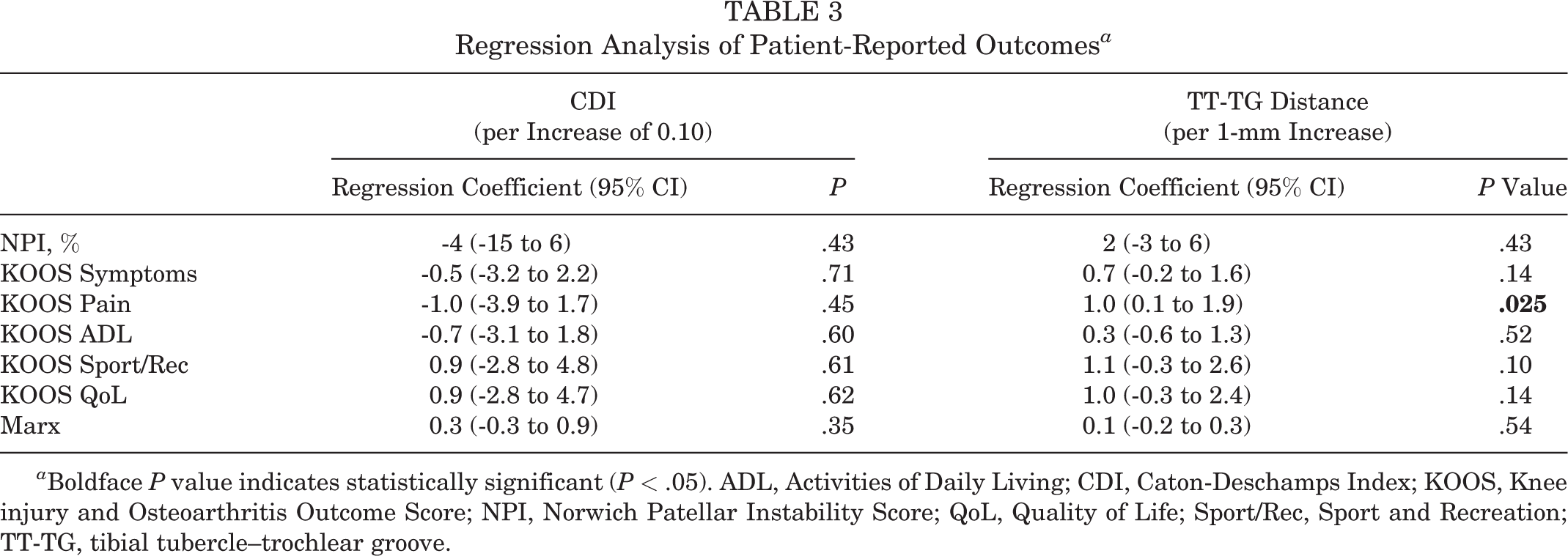
a Boldface P value indicates statistically significant (P < .05). ADL, Activities of Daily Living; CDI, Caton-Deschamps Index; KOOS, Knee injury and Osteoarthritis Outcome Score; NPI, Norwich Patellar Instability Score; QoL, Quality of Life; Sport/Rec, Sport and Recreation; TT-TG, tibial tubercle–trochlear groove.
Comparison of patient and imaging factors of those knees with completed PROMs and those without them demonstrated a slightly older age in the group that did not complete the PROMs (P = .042), but there were no other significant differences (Table 4).
Comparison of Knees With or Without Completed PROMs a

a Data are reported as mean ± SD or n (%). Boldface P value indicates statistically significant comparison (P < .05). BMI, body mass index; CDI, Caton-Deschamps index; PROM, patient-reported outcome measure; TT-TG, tibial tubercle–trochlear groove.
Discussion
The most important finding of this study is that neither elevated TT-TG distance nor CDI was associated with poorer PRO scores or decreased activity level after isolated MPFL reconstruction in this cohort with relatively normal patellar tracking. The findings of this study must be interpreted with careful consideration of the indications for isolated MPFL reconstruction. Patients with large J-signs were treated with tibial tubercle osteotomy in addition to MPFL reconstruction and not included in the current study. The findings of this study should not be used to support the performance of isolated MPFL reconstruction in patients with a large J-sign.
Several previous studies have evaluated the effect of anatomic factors on outcomes of isolated MPFL reconstruction with similar results. Pinheiro Junior et al 14 evaluated 21 knees with patella alta (CDI >1.2) and 16 knees with normal patellar height and noted no significant differences in postoperative Lysholm or Kujala scores between the 2 groups. Blanke et al 2 noted no significant difference in postoperative Kujala and Lysholm scores in patients with increased TT-TG distance and patella alta after isolated MPFL reconstruction. In addition, there was no difference in recurrent dislocation events based on patellar height or TT-TG distance. Matsushita et al 12 assessed the effects of preoperative TT-TG distance on outcomes after isolated MPFL reconstruction. There were 19 knees with an increased TT-TG distance (TT-TG >20 mm) and 15 knees with normal TT-TG distance. No correlation was found between TT-TG distance and postoperative Kujala or Lysholm scores. Finally, in a series of 224 isolated MPFL reconstructions, Hiemstra et al 9 noted no statistically significant association between presence of trochlear dysplasia, elevated TT-TG distance, or patella alta and postoperative symptoms of patellar instability, as assessed using the Banff Patellofemoral Instability Instrument. Importantly, these studies, which often used a CDI >1.20 as the cutoff for patella alta, generally included few patients with a CDI >1.30 (if they reported such information) and provided little insight into the effect of a CDI >1.30 on PROs. The data from the current study suggest that patella alta even in excess of a CDI of 1.30 does not result in poorer PROs, provided there is relatively normal patellar tracking.
It is important to note that the performance of isolated MPFL reconstruction in the setting of a CDI >1.30 may be associated with increased risk of recurrent patellar dislocation. Sappey-Marinier et al 17 demonstrated that elevated preoperative patellar height (CDI ≥1.3) increased the odds of failure after isolated MPFL reconstruction in their cohort of >200 MPFL reconstructions. They did note that the presence of a J-sign, which was present in 27% of their patients, was an additional independent predictor of failure in this cohort. The current study is underpowered to assess the risk of failure based on patellar height or TT-TG distance.
When indications for tibial tubercle osteotomy are discussed, it should also be considered that reducing recurrent dislocation risk and improving PROs may not be the only potential benefits of the addition of a tibial tubercle osteotomy. In the setting of elevated TT-TG distances, the patella may track laterally in some (but not all) patients, 23,27 even without a large J-sign. The increased contact pressures associated with lateral tracking are likely reduced via tibial tubercle osteotomy, particularly anteromedialization. 1 Similarly, patella alta has been associated with increased contact pressures in the patellofemoral joint. 10,24 While biomechanical studies are currently lacking, distalization of an abnormally high patella would be expected to lead to increased patellofemoral contact area and decreased contact pressures. Any clinical benefits of osteotomy to decrease contact pressures in the setting of either lateral patellar tracking or patella alta would likely take many years to come to light via reduction of patellofemoral osteoarthritis risk and not be apparent in this study.
Limitations
This study has several limitations. This study was performed in a retrospective manner, resulting in the use of data from several surgeons using a variety of MPFL reconstruction techniques and grafts with likely subtle differences in surgical indications for isolated MPFL surgery. While leading to a more heterogeneous study cohort, these differences also resulted in data that reflect real-world surgical practice more than a single surgeon series with a specific surgical technique. In addition, the minimum follow-up of 1 year was relatively short, which limited the ability of the study to report on longer-term outcomes of isolated MPFL reconstruction. Further, there was loss to follow-up of 24%, and only 57% of patients completed PRO questionnaires, which may lead to selection bias. Importantly, the group that completed PROMs was similar to the group that did not in regard to patient characteristics that were available for comparison, with only a 3-year difference in patient age noted. In addition, there were relatively few patients with a CDI >1.30. Although we believe the study to be appropriately powered to detect differences in PROs in this group of patients, this study cannot provide insights into the risk of redislocation based on CDI. Similarly, the study included few patients with a TT-TG distance >24 mm and cannot provide any insights in the results of isolated MPFL reconstruction in patients with this degree of TT-TG distance elevation.
Conclusion
Performance of an isolated MPFL reconstruction in the setting of moderately elevated TT-TG distances or patella alta was not associated with worse PROs in this cohort with relatively normal patellar tracking (no large J-sign). This study lacked sufficient power to comment on the relationships between patellar height and TT-TG distance of recurrent dislocation risk after isolated MPFL reconstruction.
Footnotes
Final revision submitted February 13, 2022; accepted March 22, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.C.F. has received education payments from CDC Medical; consulting fees from Bioventus, Ceterix, DePuy/Medical Device Business Services, Linvatec, Smith & Nephew, Vericel, and Zimmer Biomet; nonconsulting fees from Smith & Nephew and Karl Storz Endoscopy America; and honoraria from Vericel. M.D. has received education payments from Smith & Nephew. R.D. has received grant support from Arthrex and education payments from Arthrex and Smith & Nephew. C.K.K. has received grant support from DJO, education payments from CDC Medical, consulting fees from Arthrex and Zimmer Biomet, and nonconsulting fees from Arthrex and Smith & Nephew. R.A.M. has received grant support from DJO and education payments from CDC Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Ohio State University.