
Abstract
Background:
It remains unclear whether lateral joint space narrowing without severe cartilage loss before meniscal allograft transplantation (MAT) affects clinical outcomes and graft extrusion.
Hypothesis:
Patients with greater preoperative joint space narrowing would show more graft extrusion, more osteoarthritis progression, and worse clinical outcomes than would those with less narrowing.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
We retrospectively evaluated 61 patients who underwent lateral MAT and had a minimum follow-up of 4 to 5 years. The median preoperative joint space width (JSW) on Rosenberg view radiographs was used to classify patients into those with less joint space narrowing (JSW ≥3 mm; group A) and greater joint space narrowing (JSW <3 mm; group B). We compared differences between groups in terms of graft extrusion and articular cartilage loss (modified Outerbridge grade ≥3) on 1-year postoperative magnetic resonance imaging (MRI) scans and changes in JSW and clinical outcomes at the last follow-up.
Results:
There were 31 patients in group A and 30 patients in group B; the mean follow-up time for all patients was 64.4 ± 10.3 months. All patients showed a significant preoperative to postoperative improvement in outcome scores (P < .001 for all). The mean preoperative JSW was 3.8 ± 0.9 mm in group A and 2.3 ± 0.4 mm in group B (P < .001). In group B, there was more graft extrusion on postoperative MRI scans (3.0 ± 0.9 vs 1.9 ± 0.6 mm, respectively; P < .001) and a higher proportion of patients with pathological graft extrusion at final follow-up (43.3% vs 12.9%, respectively; P = .011) compared with group A. At 1 year postoperatively, cartilage loss grade ≥3 was observed at the lateral femoral condyle in 3.2% and 20.0% of patients in groups A and B (P = .053), respectively, and at the lateral tibial plateau in 3.2% and 30.0% of patients (P = .006), respectively. There were moderate correlations between graft extrusion and preoperative absolute JSW (r = –0.471; P < .001) and preoperative relative JSW (r = –0.428; P = .001).
Conclusion:
Patients with less preoperative joint space narrowing had less graft extrusion and cartilage loss on 1-year postoperative MRI scans, as well as better radiological and clinical outcomes at midterm follow-up, compared with patients with greater preoperative narrowing.
In relatively active and young patients with meniscal deficiencies, it is important to perform meniscal allograft transplantation (MAT) to restore native biomechanics, improve knee function, and delay the progression of osteoarthritis (OA). 35 Long-term studies have reported satisfactory clinical and radiological outcomes of MAT, and it is no longer considered experimental. 7,15,39 There may be several prognostic factors for MAT survivorship, 41 and it is important to identify the factors and to determine whether they can be modified. A recent systematic review revealed that patients with full-thickness cartilage lesions had at least a 3 times higher rate of graft failure than did those with partial-thickness cartilage lesions. 41 However, to date, the effect of joint space narrowing on MAT outcomes is relatively unknown.
After lateral meniscectomy, contact stresses increase by 200% to 350%, whereas after medial meniscectomy, contact stresses increase by 100%. 31 Subtotal or total meniscectomy results in progressive degenerative changes in the tibiofemoral joint, and lateral meniscectomy is associated with a higher incidence of OA than is medial meniscectomy. 28 A meniscal deficiency is a risk factor for joint space narrowing. 42 Lee et al 17 reported significant joint space narrowing (–0.65 ± 1.09 mm) during a mean meniscal deficiency period of 3.1 years. Therefore, in practice, many patients who are considered candidates for lateral MAT already have cartilage loss and joint space narrowing before the appearance of symptoms. 17,37
It is generally accepted that the amounts of joint space narrowing and meniscal extrusion are highly relevant to MAT outcomes. 8,13 Meniscal extrusion is a risk factor for OA progression in both native knee joints and after MAT. 1,22 Therefore, accurate graft implantation without extrusion is important to provide proper postoperative biomechanical function. 36,40 However, even if graft positioning is performed accurately without extrusion at the time of MAT, graft extrusion may occur if postoperative joint space narrowing occurs. To the best of our knowledge, no study has reported the effect of preoperative joint space narrowing on the progression of graft extrusion and OA. Even if MAT is performed according to surgical indications, the degree of joint space narrowing at the time of MAT is different for each patient.
In the current study, we aimed to compare the midterm follow-up results of lateral MAT in patients with different degrees of preoperative joint space narrowing to evaluate its effects on graft extrusion and radiological and clinical outcomes. We hypothesized that patients with greater preoperative joint space narrowing would show further graft extrusion, more OA progression, and worse outcomes than would those with less preoperative narrowing.
Methods
Patients
After receiving ethics committee approval for the study protocol, we retrospectively reviewed the medical records of 87 patients who underwent lateral MAT at our institution between 2014 and 2015. Included were patients who (1) underwent magnetic resonance imaging (MRI) within 2 days postoperatively, (2) underwent follow-up MRI at 12 months after lateral MAT, and (3) had midterm follow-up data (minimum, 48-60 months). The exclusion criteria were (1) absolute mechanical axis angle >5° or >3° deviation compared with the contralateral side on long-leg standing radiographic scanograms from the hips to ankles, (2) age >45 years, (3) uncorrected knee laxity (grade >1), (4) radiographic joint obliteration in the Rosenberg view, and (5) medial compartment OA of Kellgren-Lawrence grade ≥2. Localized articular cartilage lesions classified as modified Outerbridge grade 3 or 4, which were confined to the area covered by the meniscal graft, were not considered an exclusion criterion.
Based on these criteria, we excluded 2 patients who did not undergo follow-up MRI, 4 patients with incomplete clinical data, 14 patients who had a follow-up <5 years, and 6 patients who had a preserved joint space <15%. The remaining 61 patients were included in this study.
Surgical Technique and Postoperative Rehabilitation
The surgical indication for lateral MAT was previous total or subtotal meniscectomy; 52 of the 61 patients with a lateral meniscal deficiency were diagnosed with a discoid meniscus at the time of meniscectomy. Lateral MAT was performed using the keyhole technique with modified instruments by a single experienced surgeon (J.G.K.). 21 All patients received fresh-frozen and nonirradiated meniscal allografts. The graft size was measured on anteroposterior and lateral radiographs with scanograms for the correction of magnification using the modified Pollard method. 9,30 After an arthroscopic evaluation and resection of the remaining lateral meniscus, 4-cm longitudinal arthrotomy was performed just lateral to the lateral border of the patellar tendon. A keyhole-shaped slot was created using our customized osteotome and dilator (Cellumed) along the centers of the anterior and posterior attachment sites under the lateral eminence of the tibial articular surface and approximately 15° above the tibial slope. The lateral meniscal allograft, including a bone bridge, was advanced into the keyhole-shaped slot and was manually reduced under the condyle with a finger under traction of the posterior leading suture. After confirming that the entire meniscal allograft was spread out evenly, we used the inside-out method to secure the middle horn of the meniscal allograft. The posterior horn was secured using the Fast-Fix 360 system (Smith & Nephew), and the anterior one-third was secured with 2 or 3 direct polydioxanone sutures (PDS II; Ethicon) using the outside-in method. A final arthroscopic evaluation was conducted to confirm the fixed anterior and posterior roots and tension of the entire meniscal allograft.
All patients underwent a delayed rehabilitation program, as reported in a previous study. 20 Patients were placed in a cast with a varus force at full extension for 3 weeks after lateral MAT. Range of motion exercises were started at 3 weeks after the cast was removed, and the allowed range of motion at 6 and 12 weeks was 90° and 120°, respectively. A lateral unloading brace (DonJoy OA Adjuster; DJO Global) was applied for 9 weeks after the cast was removed. Gradual partial weightbearing was allowed during the first 6 weeks, and full weightbearing was allowed at 6 weeks. Patients were instructed to perform isometric quadriceps muscle-strengthening and straight leg–raising exercises immediately after surgery. Isokinetic exercises were started at 10 to 12 weeks, and light running and squatting were allowed at 4 to 5 months. Return to noncontact sports was permitted at 7 to 9 months, although strenuous contact sports were prohibited until 10 to 12 months. Whether the patient decided to return to sports depended on the recovery of muscle strength and knee function over time.
Clinical and Radiographic Evaluations
Subjective function was assessed using the Lysholm score and International Knee Documentation Committee (IKDC) subjective score. Outcome measures and radiographic examinations were administered preoperatively and at 6, 12, 24, and 48 to 60 months postoperatively. All radiographic assessments were performed using a picture archiving and communication system (PACS) workstation (Centricity RA1000; GE Healthcare).
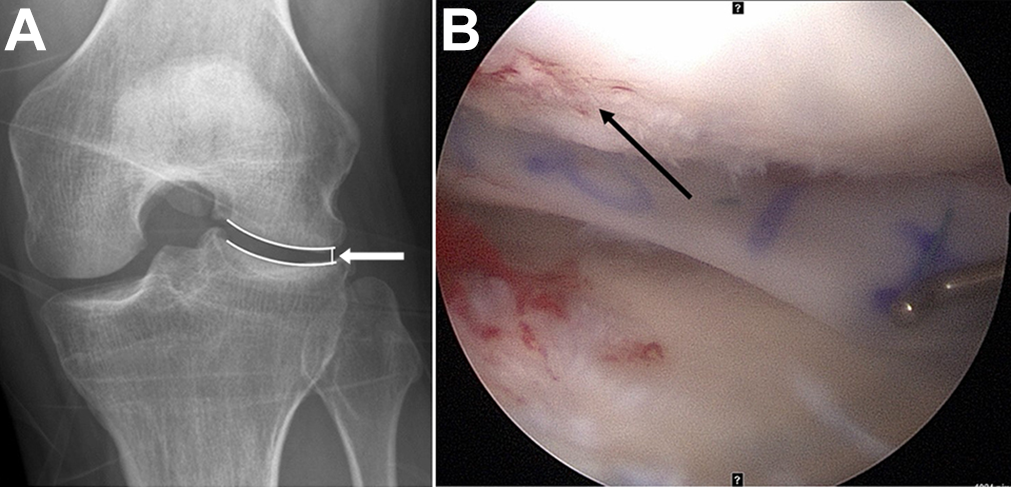
The absolute joint space width (JSW) for each patient was measured in the Rosenberg view from the lateral edge of the femoral condyle to the lateral edge of the tibial plateau (Figure 1). 10,19 Bony spurs were excluded from the measurements. To better standardize the data, we also calculated the relative JSW for each patient by dividing the absolute JSW of the operated knee by the absolute JSW of the contralateral knee. The progression of joint space narrowing was assessed at 3 time points: 1 day before surgery, 1 year postoperatively, and midterm follow-up (48-60 months postoperatively).

The absolute joint space width (arrow) of a left knee on a Rosenberg view radiograph was calculated from the lateral edge of the femoral condyle to the lateral edge of the tibial plateau. Any bony spurs were excluded from the measurement.
Lower extremity alignment was evaluated by measuring the mechanical axis angle (hip-knee-ankle angle) on standing anteroposterior scanograms. 43 Radiological measurements were independently performed by 2 experienced orthopaedic surgeons (D.W.L. and J.K.L.). Each examiner conducted all measurements twice with a 6-week interval, and the mean value of these measurements was used in the analysis.
The median preoperative JSW was used to classify patients into those with less narrowing and greater narrowing. We calculated the median JSW to be 3.0 mm. Based on this value, there were 31 patients with less or no narrowing (JSW ≥3 mm; group A) and 30 patients with greater narrowing (JSW <3 mm; group B).
MRI Evaluation
To assess extrusion of the meniscal allograft and the cartilage status of the lateral compartment, we performed a follow-up MRI at 2 days and 12 months postoperatively. Patients signed an informed consent form before undergoing MRI using a 3.0-T system (Signa HD; GE Healthcare). Analysis was performed using the cross-link tool of the PACS workstation. Graft extrusion in the coronal plane was assessed by measuring the distance from the lateral margin of the graft to the superolateral aspect of the tibial plateau. Pathological extrusion was defined as graft extrusion ≥3 mm (Figure 2). 3,5,13,24,25 Patients were categorized into pathological and nonpathological extrusion subgroups based on MRI findings at 1 year postoperatively.

Magnetic resonance imaging scan at 1 year postoperatively showing graft extrusion of 3.1 mm (arrow).
The cartilage status in the lateral compartment was assessed according to the modified Outerbridge grade (grade 0, normal; grade 1, cartilage surface fibrillation; grade 2, <50% loss of cartilage thickness; grade 3, >50% loss of cartilage thickness; grade 4, exposed subchondral bone). 6,12,29 The worst areas of cartilage loss (Outerbridge grade ≥3) of the lateral femoral condyle (LFC) and the lateral tibial plateau (LTP) were reported to determine the overall status of the corresponding articular cartilage. 23
Statistical Analysis
Statistical analysis was performed using SPSS software (SPSS Statistics 21; IBM Corp), and statistical significance was set at P < .05. Changes in JSW, graft extrusion, functional scores, and cartilage status from preoperatively to latest (midterm) follow-up were compared between groups A and B. The independent t test was used to compare parametric variables (eg, JSW, graft extrusion, and functional scores), and the Mann-Whitney U test was used to compare nonparametric variables (eg, cartilage loss). Preoperative and postoperative parametric or nonparametric variables within each group were compared using the paired t test or Wilcoxon signed rank test. The Pearson correlation coefficient was used to analyze the relationship between JSW and graft extrusion. Intraobserver and interobserver agreements were assessed using kappa values and were classified as excellent (0.81-1.00), substantial (0.61-0.80), moderate (0.41-0.60), fair (0.21-0.40), or slight (0.00-0.20). 16
To detect a difference of 2 mm in graft extrusion between the 2 groups with a level of significance of 5% and a power of 80%, the required sample size was determined to be 16 patients per group. Therefore, the number of patients in both groups had sufficient statistical power.
Results
The intraobserver and interobserver agreements for the JSW measurements ranged from 0.82 to 0.89, indicating excellent agreement. The mean follow-up period for all patients was 64.4 ± 10.3 months. The mean preoperative JSW was 3.1 ± 1.2 mm overall (3.8 ± 0.9 mm in group A and 2.3 ± 0.4 mm in group B; P < .001). In addition, there was a significant between-group difference in the percentage of patients with cartilage loss grade ≥3 at the LTP (P = .033). There were 3 patients (1 in group A and 2 in group B) with an Outerbridge grade 4 lesion who underwent microfracture of the LFC at the same time as MAT. There were no differences in age, sex, mechanical axis angle, functional knee scores, or cartilage status of the LFC at the time of lateral MAT between the study groups (Table 1).
Descriptive and Preoperative Data a

a Data are presented as mean ± SD or n (%). Boldface values indicate a statistically significant difference between groups (P < .05). IKDC, International Knee Documentation Committee; JSW, joint space width; LFC, lateral femoral condyle; LTP, lateral tibial plateau; MRI, magnetic resonance imaging.
The changes in JSW over time are summarized in Table 2, and radiological and clinical outcomes at midterm follow-up are presented in Table 3. Graft extrusion at 1 year postoperatively was greater in group B than in group A (3.0 ± 0.9 vs 1.9 ± 0.6 mm, respectively; P < .001). At 1 year postoperatively, cartilage loss grade ≥3 was observed at the LFC in 3.2% and 20.0% of patients (P = .053), respectively, and at the LTP in 3.2% and 30.0% of patients (P = .006), respectively, in groups A and B.
Changes in JSW Over Time a

a Data are presented as mean ± SD. Boldface values indicate a statistically significant difference between groups (P < .05). JSW, joint space width.
Radiological and Clinical Outcomes at Midterm Follow-up a
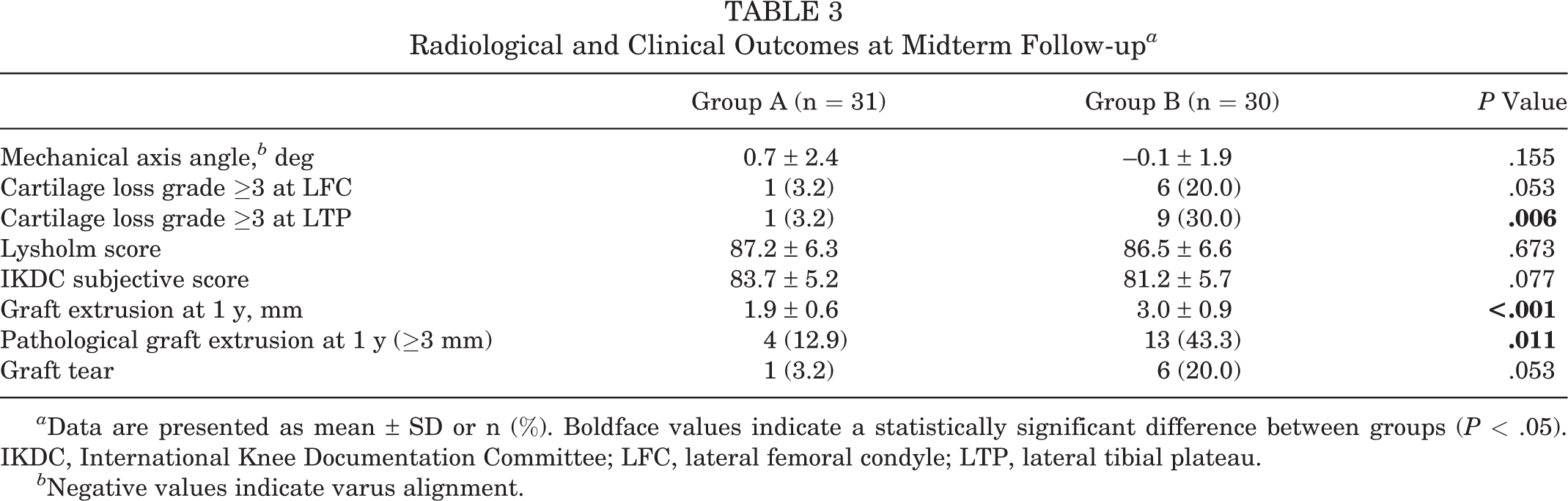
a Data are presented as mean ± SD or n (%). Boldface values indicate a statistically significant difference between groups (P < .05). IKDC, International Knee Documentation Committee; LFC, lateral femoral condyle; LTP, lateral tibial plateau.
b Negative values indicate varus alignment.
The progression of joint space narrowing, graft extrusion, and cartilage loss between the 2 groups is described in Table 4. There were no significant within-group differences in preoperative versus postoperative JSW (P = .381 in group A and P = .446 in group B); however, there were significant within-group and between-group differences in graft extrusion between 2 days and 1 year postoperatively (P < .001 for all). There were no significant within-group differences in preoperative versus postoperative cartilage loss at the LFC (P = .331 in group A and P = .064 in group B) or LTP (P = .346 in group A and P = .102 in group B).
Changes in Joint Space Narrowing, Graft Extrusion, and Cartilage Loss Between Preoperatively and Midterm Follow-up a

a Data are presented as mean ± SD or n (%). Boldface value indicates a statistically significant difference between groups (P < .05). JSW, joint space width; LFC, lateral femoral condyle; LTP, lateral tibial plateau.
b Postoperative minus preoperative values.
c Postoperative 1-year minus postoperative 2-day values.
The Lysholm and IKDC subjective scores for all patients were higher at midterm follow-up than the preoperative scores (P < .001 for both). There was no difference in Lysholm or IKDC scores between the 2 groups at midterm follow-up (P = .673 and P = .077, respectively).
A graft tear was found in 1 patient (3.2%) in group A and 6 patients (20.0%) in group B (P = .053). Overall, 7 graft tears occurred at a mean time of 2.1 years; 2 patients with these tears underwent revision lateral MAT, 3 patients underwent meniscectomy (less than one-third of the allograft), and 2 patients did not undergo surgery. The definition of graft failure was meniscectomy of greater than one-third of the allograft. Therefore, midterm follow-up results excluded the findings of 2 patients who underwent revision MAT.
In the correlation analysis, there was a moderate negative correlation between postoperative graft extrusion and preoperative absolute (r = –0.471) and relative (r = –0.428) JSW, indicating that larger graft extrusion was associated with a smaller preoperative JSW (Table 5).
Correlation Between Graft Extrusion and Preoperative JSW a

a JSW, joint space width.
Discussion
The most important finding of the current study was that patients with less or no preoperative joint space narrowing (JSW ≥3 mm; group A) had better radiological and clinical outcomes than did those with greater narrowing (JSW <3 mm; group B) at midterm follow-up after lateral MAT. Graft extrusion at 1-year follow-up was greater in group B than in group A (3.0 ± 0.9 vs 1.9 ± 0.6 mm, respectively; P < .001), and there was a higher percentage of patients with pathological graft extrusion at final follow-up in group B versus group A (43.3% vs 12.9%, respectively; P = .011). In addition, there were moderate negative correlations between larger graft extrusion and smaller absolute (r = –0.471; P < .001) and relative (r = –0.428; P = .001) preoperative JSW. These results imply that more joint space narrowing before lateral MAT could negatively affect allograft stabilization.
Lateral meniscal deficiencies related to meniscectomy or neglected degenerative discoid meniscal tears result in increased contact stresses on the articular cartilage and progressive degenerative changes, such as cartilage loss and joint space narrowing, in the lateral compartment. 17,18,33 In evaluating joint space narrowing, we thought that the results of analysis in the Rosenberg view were more meaningful than were those in the full-extension view. 19,26 The reason for measuring the JSW of the lateral edge was that in most cases, only the lateral edge was observed to be significantly reduced. 26 We suggest that joint space narrowing of the lateral edge and cartilage loss are not closely related. In other words, it is unreasonable to apply a universal classification such as the Kellgren-Lawrence grade for determining joint space narrowing of the lateral edge. Even if there is a progression of joint space narrowing, the cartilage status is often maintained relatively well (Figure 3). In our study, there were no significant differences in the proportion of patients with cartilage loss grade ≥3 on the LFC.
Images from a patient with moderate joint space narrowing at the time of lateral meniscal allograft transplantation (MAT). (A) Preoperative Rosenberg view showing a joint space width of 2.4 mm in the left knee (white arrow). (B) At the time of lateral MAT, no cartilage lesions were observed, although cartilage fibrillation (modified Outerbridge grade 1; black arrow) was seen.
Joint space narrowing in a large number of patients at the time of MAT may be attributed to the high incidence of a lateral discoid meniscus. In our study, 85.2% of 61 patients with a lateral meniscal deficiency were diagnosed with a discoid meniscus at their first visit to our institution. The prevalence of a lateral discoid meniscus was reported to be 15.3% in Korea and 16.6% in Japan, although there are no exact data regarding the prevalence in the general population. 2 Ahn et al 2 showed that some adult patients with a torn lateral discoid meniscus had various stages of preexisting lateral compartment OA at their first clinical visit. In their study involving 305 patients, marginal osteophytes on radiographs were found in 36% of patients with a torn lateral discoid meniscus, and a confirmed chondral lesion on arthroscopic examination was found in 27% of patients. Ahn et al 2 concluded that a symptomatic torn lateral discoid meniscus was associated with coexisting OA. Preoperative symptoms do not reflect the cartilage status in the compartment where the meniscus is deficient, and studies have reported that in practice, cartilage loss is already significantly progressed if symptoms become apparent in patients under consideration for MAT. 17,37
In the current study, pathological graft extrusion was significantly more common in group B than in group A, although all patients showed ≤3 mm of graft extrusion on MRI scans at 2 days postoperatively. Graft extrusion increased by 1.1 ± 0.8 mm in group A and 2.0 ± 0.9 mm in group B (P < .001). The biomechanical and clinical effects of graft extrusion on knee joints after MAT have not been clearly identified. 32,34,35 However, theoretically, a well-positioned allograft within the joints of the femur and tibia could transmit a close to normal load, as noted in previous biomechanical studies. 4,14,27 In the presence of pathological graft extrusion, the meniscal graft cannot provide normal meniscal function, which can cause early graft and cartilage degeneration. 4,14,27 A 2019 study involving 45 patients reported that pathological graft extrusion was found in 42.2% of patients at long-term follow-up, and the pathological extrusion group had greater joint space narrowing than did the nonextrusion group. 22 In terms of OA progression, cartilage loss grade ≥3 at the LFC was seen in 3.2% and 20.0% of the patients in groups A and B, respectively, at 1 year postoperatively, a finding that approached significance (P = .053), although there was no significant difference between the groups preoperatively. Summarizing our study findings, we believe that patients with greater joint space narrowing preoperatively have an increased chance of more graft extrusion and worse OA compared with those with less narrowing preoperatively. However, because there was no statistically significant difference between the 2 study groups in terms of the progression of cartilage loss, studies with larger sample sizes are needed to confirm this hypothesis.
The findings of the present study provide indirect evidence that joint space management at the time of lateral MAT is necessary to reduce graft extrusion and OA progression. In our study, axial malalignment was <5° in all patients, including those with greater joint space narrowing. In the same context as attempting cartilage repair for cartilage lesions, joint space narrowing can also be considered a factor that needs correction. 11,38
Limitations
The present study had several limitations. First, this was a retrospective study with a relatively small sample size of 61 patients. However, preoperative descriptive data after a retrospective review showed that the 2 groups did not differ significantly. Second, the JSW in the Rosenberg view did not accurately explain the condition of the involved joint, and there is still a lack of clear methods for measuring joint space narrowing. Thus, 2 authors (D.W.L. and J.K.L.) measured the JSW with reference to the lateral edge of the lateral compartment and calculated the median value. Third, graft extrusion was assessed only on MRI scans at 12 months postoperatively. Because this was a relatively short-term study, longer follow-ups are required to confirm OA progression because of the altered biomechanical environment caused by graft extrusion. Finally, patients in group B had a mean preoperative JSW of approximately 2 mm, which can lead to a misunderstanding that we expanded the indication for lateral MAT compared with previous studies. Even if there is joint space narrowing, the cartilage status can vary, and we initiated the present study on the assumption that the MAT prognosis can vary depending on the amount of preoperative joint space narrowing, focusing on this parameter rather than cartilage status.
Conclusion
Patients with less preoperative joint space narrowing had less graft extrusion and cartilage loss on 1-year postoperative MRI scans, as well as better radiological and clinical outcomes at midterm follow-up, compared with patients with greater preoperative narrowing.
Footnotes
Final revision submitted February 8, 2022; accepted March 23, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by Konkuk University Medical Center Research Grant 2021. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Konkuk University Medical Center (No. KUMC 2021-03-037).