
Abstract
We appreciate the interest in our study and the opportunity to respond to the issues raised. We agree that understanding the accuracy, reliability, and precision of the methodology of ultrasound (US) is critical to the appropriate interpretation and application of the results.
First, we apologize for the error in Table 1 of the original article, 2 which presented the reliability and precision data. We created confusion by combining the intraclass correlation coefficients, standard errors of measurement, and minimal detectable changes (MDCs) for both thickness and gapping, and we mistakenly switched the gapping data with the thickness reliability data in the rows. These have been corrected in Table 1 here.
Reliability of Ultrasound Measurements (Updates to Table 1 of Kissenberth et al 2 ) a

a ICC, intraclass correlation coefficient; MDC, minimal detectable change; SEM, standard error of measurement; UCL, ulnar collateral ligament.
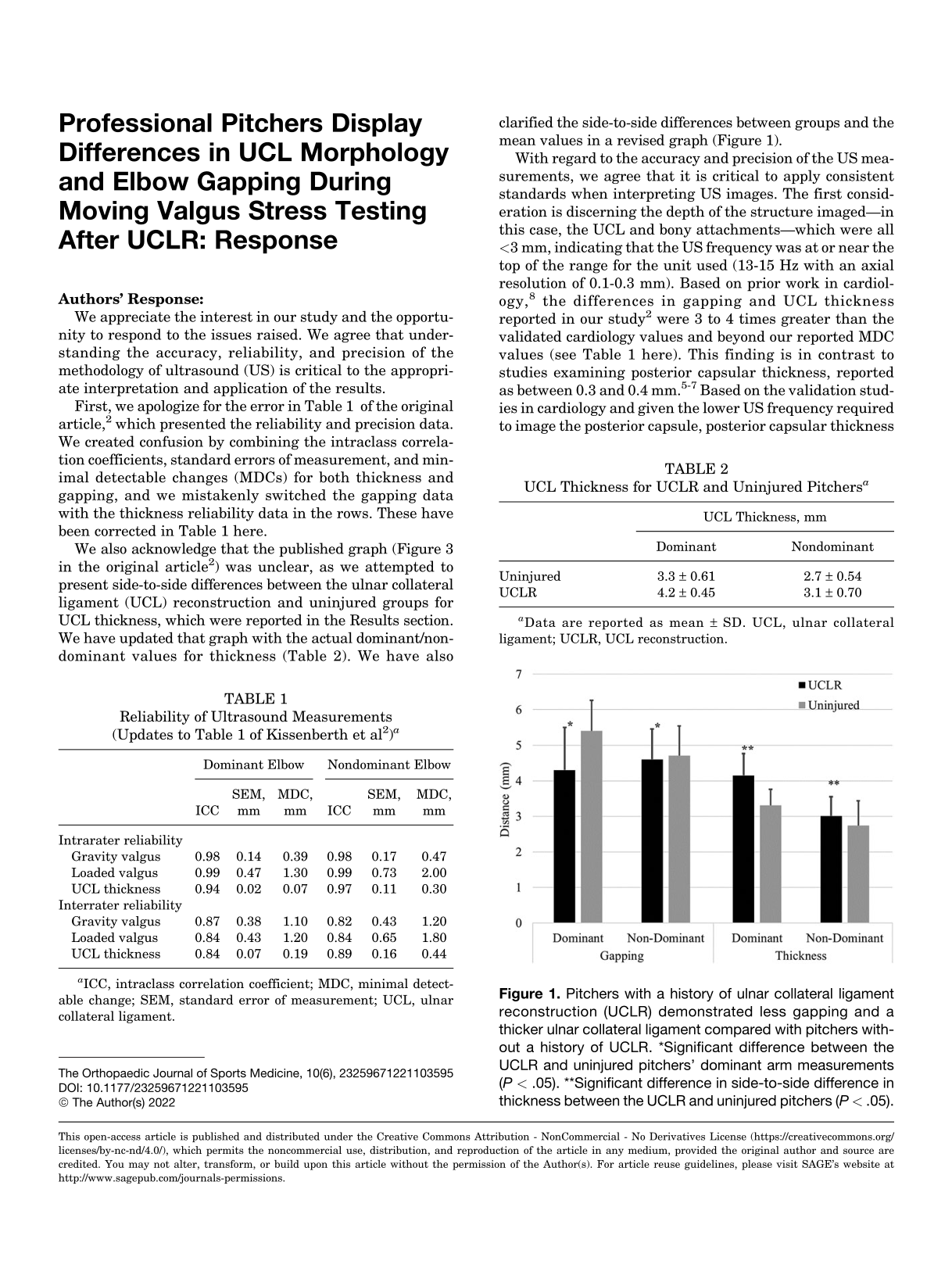
We also acknowledge that the published graph (Figure 3 in the original article 2 ) was unclear, as we attempted to present side-to-side differences between the ulnar collateral ligament (UCL) reconstruction and uninjured groups for UCL thickness, which were reported in the Results section. We have updated that graph with the actual dominant/nondominant values for thickness (Table 2). We have also clarified the side-to-side differences between groups and the mean values in a revised graph (Figure 1).
UCL Thickness for UCLR and Uninjured Pitchers a

a Data are reported as mean ± SD. UCL, ulnar collateral ligament; UCLR, UCL reconstruction.

Pitchers with a history of ulnar collateral ligament reconstruction (UCLR) demonstrated less gapping and a thicker ulnar collateral ligament compared with pitchers without a history of UCLR. *Significant difference between the UCLR and uninjured pitchers’ dominant arm measurements (P < .05). **Significant difference in side-to-side difference in thickness between the UCLR and uninjured pitchers (P < .05).
With regard to the accuracy and precision of the US measurements, we agree that it is critical to apply consistent standards when interpreting US images. The first consideration is discerning the depth of the structure imaged—in this case, the UCL and bony attachments—which were all <3 mm, indicating that the US frequency was at or near the top of the range for the unit used (13-15 Hz with an axial resolution of 0.1-0.3 mm). Based on prior work in cardiology, 8 the differences in gapping and UCL thickness reported in our study 2 were 3 to 4 times greater than the validated cardiology values and beyond our reported MDC values (see Table 1 here). This finding is in contrast to studies examining posterior capsular thickness, reported as between 0.3 and 0.4 mm. 5 –7 Based on the validation studies in cardiology and given the lower US frequency required to image the posterior capsule, posterior capsular thickness measurements are much more uncertain and prone to error compared with the UCL thickness measurements reported in our study.
Additionally, our gapping and UCL thickness measurements are consistent with those of Ciccotti et al. 1 While our gapping was less, it is most likely because of markedly less force and greater elbow flexion, which would approximate the medial elbow joint.
Finally, regarding the testing position, force, and methodology, as outlined in the introductory section and elaborated in the Discussion section, the purpose of our study was to evaluate a clinically applicable approach to using US to assess the throwing elbow. While the methods used by Ciccotti et al 1 work well in a research environment, they are not usable in a real-world setting. Additionally, when discussing using the Telos device/approach with the leadership of several baseball organizations, none was willing to have its pitchers participate. Thus, we used the most common UCL injury test (the “moving valgus stress test” 3 ) and imaged the UCL during this maneuver. Based on the reliability and precision reported and the face validity of the results here as well as the clinical utility of identifying pitchers at risk for UCL injuries in the subsequent season, 4 we are confident in the clinically applicable method and conclusions drawn in our study.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: C.A.T. has received research support from Arthrex and Neurotech, consulting fees from Breg, speaking fees from Arthrex, and stock/stock options in Players Health and Trex. M.J.K. has received educational support from Arthrex and Peerless Surgical, consulting fees from Arthrex, speaking fees from Arthrex, and hospitality payments from Exactech. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.