
Abstract

We read with great anticipation the recent article in The Orthopaedic Journal of Sports Medicine by Kissenberth et al 2 entitled “Professional Pitchers Display Differences in UCL Morphology and Elbow Gapping During Moving Valgus Stress Testing After UCL Reconstruction.” We have some serious concerns about the data presented that, in the interest of science, we believe need to be reconciled.
Inconsistencies in the Reporting of Results
The data from Kissenberth et al 2 support increased thickness of the ulnar collateral ligament (UCL) in nondominant (ND) versus dominant (D) elbows. This is counterintuitive and does not coincide with their statement, “The average UCL thickness in UCLR was significantly greater in D elbows compared with ND elbows (1.1 ± 0.09 vs 1.65 ± 0.11 mm; P < .03).”2(p3) Based on the data presented in parentheses as well as in Figure 3 of their article, this should instead read “thickness in UCLR was significantly less in D elbows….”
Another source of inconsistency is found in the following statement: “Our study also showed that greater pitching elbow UCL thickness (3.4 mm [D arm] vs 2.8 mm [ND arm]; P < .001) was consistent with previous studies.”2(p4) These measurements of 3.4 and 2.8 mm are impossible based on the data reported throughout the results. Kissenberth et al 2 reported that the D UCL thickness of the UCL reconstruction (UCLR) and uninjured pitchers averaged 1.1 and 0.17 mm, respectively, while the ND UCL thickness averaged 1.65 and ∼0.17 mm, respectively. While the values mentioned in the discussion section (3.4 mm [D arm] vs 2.8 mm [ND arm]) do align with previously reported values in baseball players, these data points do not appear accurate relative to the values presented throughout the Results section.
Also, in Figure 3, there is an asterisk above the ND gapping data examining between-group comparisons, indicating that there are statistically significant differences between UCLR and uninjured pitchers. However, that is not possible based on the means and standard deviations presented in Figure 3. Instead of signifying differences between UCLR and uninjured pitchers, the authors may have been using the asterisk to represent this significant bilateral difference, which they mention in the Results section: “The D arm of uninjured pitchers demonstrated greater gapping compared with the ND arm (5.4 ± 1.2 vs 4.7 ± 0.86 mm; P = .001).”2(p3) However, this is inconsistent reporting of significant differences in Figure 3. The asterisk should be standardized to represent significant differences between UCLR and uninjured participants, and a separate symbol should be utilized to highlight bilateral differences within a group.
Last, the hypothesis in the abstract states that the ulnohumeral joint of UCLR pitchers will have greater gapping: “We hypothesized that the ulnohumeral joint will display greater gapping and the UCL graft will be thicker in pitchers after UCLR compared with uninjured pitchers.”2(p1) In contrast, the hypothesis in the introductory section states that the ulnohumeral joint of UCLR pitchers will have less gapping: “In the current study, we hypothesized that US evaluation during the moving valgus stress test arc in professional pitchers with a history of UCLR will display less ulnohumeral joint gapping and greater UCL graft thickness compared with the native ligament in pitchers without UCLR.”2(p2)
Validity of the Data
We are also confused as to the validity of the UCL thickness measurements. All the relevant studies cited within the Kissenberth et al 2 article found that the UCL thickness in baseball pitchers was at least 1 mm larger in the D arm compared with the ND arm (Table 1). However, the authors found that the D UCL was instead 0.55 mm smaller than the ND UCL in UCLR pitchers and that UCL thickness was similar bilaterally in uninjured pitchers. Kissenberth et al also found that the ND UCL thickness in UCLR pitchers was 10 times larger (1.65 vs ∼0.17 mm, respectively) than the ND UCL thickness in pitchers without a prior UCL injury, despite no history of throwing, injury, or surgery on the ND side in either cohort.
Bilateral UCL Thickness Measurements on Ultrasound From Relevant Studies a
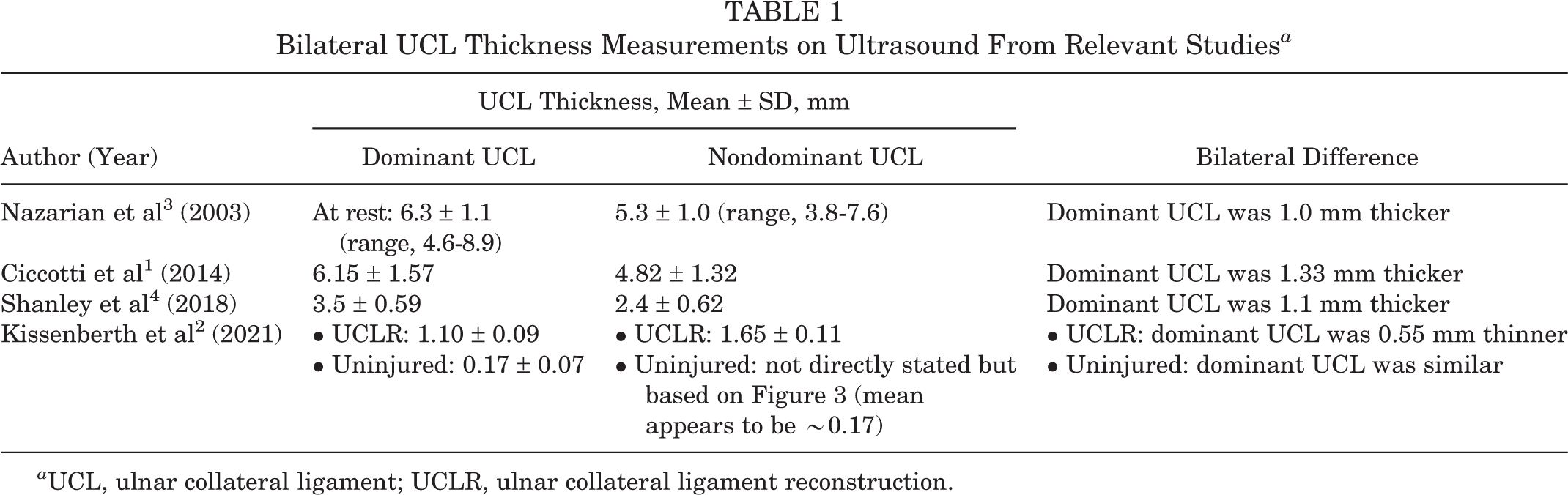
a UCL, ulnar collateral ligament; UCLR, ulnar collateral ligament reconstruction.
Statistically Versus Clinically Meaningful Differences
Because 2 researchers were used to perform the ultrasound evaluation, the interrater reliability minimal detectable change (MDC) should be considered (shown in Table 1 of the published article2). If those MDC values are considered, then some of the statistically significant differences are not clinically meaningful and should have been brought to light in their Discussion section. For example, the authors state that “the average ulnohumeral joint distance with valgus gravity stress was significantly greater in D elbows versus in ND elbows, respectively (4.1 ± 1.2 vs 3.6 ± 0.84 mm; P = .001).”2(p3) However, the MDC reported for valgus gravity stress of the D and ND elbows was 1.2 and 1.8 mm, respectively. These MDC measurements far exceed the bilateral difference of 0.5 mm (4.1 vs 3.6 mm, respectively).
Kissenberth et al 2 also state that “the average UCL thickness in UCLR was significantly greater in D elbows compared with ND elbows (1.1 ± 0.09 vs 1.65 ± 0.11 mm; P < .03).”2(p3) However, the MDC reported for UCL thickness of the D and ND elbows was 1.3 and 2.0 mm, respectively. These MDC measurements also far exceed the bilateral difference of 0.55 mm (1.1 vs 1.65 mm, respectively). Table 2 illustrates further examples of results in which clinical significance (represented by group differences being larger than the MDC) was lacking.
Interrater Reliability of Ultrasound Assessment for MDC of UCL Gapping and UCL Thickness per Kissenberth et al2 a

a Differences between groups that were smaller than the interrater minimal detectable change (MDC) values are in boldface. D, dominant; ND, nondominant; UCL, ulnar collateral ligament; UCLR, UCL reconstruction.
b Not directly stated in the article whether the difference between groups is with gravity valgus or loaded valgus.
c Not directly stated in the article whether the difference between groups is in the dominant or nondominant elbow.
Methodological Concerns
There is a methodological concern with the authors’ use of producing standardized valgus torque at the elbow. With this technique, the force of 5.5 lb is standardized along with the location of the force at the ulnar styloid of the wrist. The equation for torque is force × moment arm. Because the force is always applied to the ulnar styloid of the wrist, the resultant valgus torque applied to the elbow joint will be variable based on the length of the moment arm (the length of each participant’s forearm). Players with longer forearms, and thus longer moment arms, will have greater torque imposed on their elbow. UCL joint gapping is a measure of torque, not force, so players with longer forearms will have increased gapping. Without a standardized torque to the elbow joint, the joint gapping data cannot accurately be compared across participants, and therefore, the group comparisons are invalid.
The authors are commended for devising a technique that is clinically feasible and easy; however, UCL gapping is related to torque and not force. The authors, at a minimum, could have measured forearm length to show that lengths were (hopefully) similar across groups. An easy protocol that includes standardized torque would involve measuring the moment arm (forearm length) first, inputting that into a torque equation (torque = force × moment arm) and dividing the measured moment arm by a standardized torque. The output, a force, would then be applied using a dynamometer, and thus, torque would be standardized instead of force. Another option is to standardize both the force and the moment arm, for example, by applying 5.5 lb of force 10 inches distal to the medial epicondyle. In this example, all participants would be standardized to receive 6.2 N·m of valgus torque.
Thank you for taking the time to consider these questions. We look forward to your response!
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: J.D.K. has received consulting fees from Flexion Therapeutics and Heron Therapeutics and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.