
Abstract
Background:
Isolated pediatric lateral ankle injuries, including ankle sprain (AS) and nondisplaced Salter-Harris type 1 (SH-1) distal fibular fracture, are common orthopaedic sports-related injuries. Variability in treatment is suspected among pediatric orthopaedic surgeons. Complications from medical treatment or lack thereof have not been reported in this population.
Purpose:
The purpose of this study was to investigate treatment variability and associated complications after pediatric AS and SH-1 via a survey of members of the Pediatric Orthopaedic Society of North American (POSNA).
Study Design:
Cross-sectional study. Level of evidence, 5.
Methods:
A voluntary, anonymous survey was distributed to POSNA membership (approximately 1400 members) via email. Survey questions, specific to both grade 1 or 2 AS and nondisplaced or minimally displaced SH-1 injuries in skeletally immature patients, focused on initial evaluation, immobilization, return to sports, and complications. We analyzed variability both in treatment between AS and SH-1 injury and in respondent characteristics. For statistical analysis, chi-square or Fisher exact test was used for categorical variables, and analysis of variance was used for continuous variables.
Results:
The survey response rate was 16.4% (229/1400). Of the respondents, 27.7% used examination only to distinguish between AS and SH-1, whereas 18.7% performed serial radiography to aid with diagnosis. A controlled ankle motion boot or walking boot was the most common immobilization technique for both AS (46.3%) and SH-1 (55.6%); the second most common technique was bracing in AS (33.5%) and casting in SH-1 (34.7%). Approximately one-third of all respondents recommended either outpatient or home physical therapy for AS, whereas only 11.4% recommended physical therapy for SH-1 (P < .01). Results showed that 81.2% of respondents reported no complications for SH-1 treatment and 87.8% reported no complications for AS treatment. Cast complications were reported by 9.6% for SH-1 and 5.2% for AS. Rare SH-1 complications included distal fibular growth arrest, infection, nonunion, late fracture displacement, and recurrent fracture.
Conclusion:
Significant variability was found in primary treatment of pediatric AS and SH-1 injuries. Rare complications from injury, treatment, and neglected treatment after SH-1 and AS were reported.
Keywords
Lateral ankle injuries, including grade 1 or 2 ankle sprain (AS) or nondisplaced Salter-Harris distal fibular fracture, are some of the most frequent injuries treated in pediatrics, 7 especially in young athletes. In 2013, the National Athletic Trainers' Association published a position statement regarding the treatment of ASs that included compression, protected weightbearing for grade 3 ASs, and early mobilization 15 ; however, these recommendations were primarily for injuries that occur in skeletally mature high school students and were not designed for pediatric ankle injuries.
An anatomic distinction in pediatric lateral ankle injuries is the presence of the distal fibular physis. Along with a sprain of the anterotalofibular ligament and the calcaneofibular ligament, the distal fibular physis can be injured in the form of a Salter-Harris type 1 (SH-1) or type 2 fracture during an inversion injury. The diagnosis of SH-1 has been thought to be based on clinical examination alone 4 ; however, according to Sankar et al, 26 18% of suspected distal fibular SH-1 fractures had evidence of periosteal reaction indicative of a fracture 3 weeks after injury. Boutis et al 5 performed magnetic resonance imaging (MRI) on all pediatric patients with low-energy, radiographic-negative lateral ankle injuries and found that just 4.4% had evidence of a distal fibular physeal fracture. Although the clinical distinction and incidence of pediatric AS and SH-1 remain in question, optimization of clinical decision making remains pertinent for this common injury.
Although low-energy lateral ankle injuries in pediatric patients are often radiographically indistinguishable, their treatment remains variable. Gill and Klingele 9 recommended against immobilization and advocated for early functional rehabilitation for grade 1 or 2 AS, whereas 3 to 4 weeks of immobilization in a walking boot or cast was recommended for SH-1 fractures. A similar recommendation was proposed by Halstead 12 and Wuerz and Gurd 34 ; however, Halstead also considered return to sports 5 to 6 weeks after SH-1 while recommending that a patient with AS undergo physical therapy before returning to sports. Gruskay et al 11 recommended formal physical therapy with a 3-phase program for pediatric lateral ankle instability without noting a difference between a physeal and a soft tissue injury. Olgun and Maestre 22 recommended immobilization and protected weightbearing for all nondisplaced fractures about the ankle in a pediatric patient, including SH-1, for 4 to 6 weeks. In a retrospective review of a referral to a single orthopaedic surgery service, immobilization for SH-1 was longer than for AS (26.1 days compared with 17.3 days, respectively; P < .001), and only 33% of those with AS were referred for physical therapy. 32
Little to no evidence or consensus is available regarding the treatment of this high-incidence injury in pediatrics. As such, there is little understanding of the rationale between treatment recommended for AS versus SH-1. A recent systematic review suggested that low-energy lateral ankle injuries in pediatric patients are underrepresented in the medical literature and that perhaps SH-1 may be overtreated. 3 Treatment options vary from no immobilization to cast immobilization with restricted weightbearing; all variations have potential complications that have not been reported.
The purpose of this study was to survey the active membership of the Pediatric Orthopaedic Society of North America (POSNA) regarding management of these injuries. A secondary purpose was to describe complications from initial injury, medical treatment, and lack of treatment after pediatric AS and SH-1 injuries. We hypothesized that there would be significant treatment variability between AS and SH-1 injuries.
Methods
An electronic survey was developed via the POSNA Quality, Safety, and Value Initiative Sports Committee for querying of the active membership of POSNA via a Research Data Capture (REDCap) electronic database (survey available as Supplemental Material). The survey was approved by the POSNA Evidence Based Practice Committee and was distributed in February 2019 via email among the active members of POSNA (approximately 1400 members). Voluntary participation was requested via email, with no compensation for participation. At 3 weeks after the initial emails were sent, a second reminder was sent for a total active survey collection that occurred over 6 weeks. Ethics committee approval was not required for this study, given that no patient-related information was collected.
The anonymous survey was developed in order to answer specific questions about experiences with lateral ankle injuries in pediatric patients. Included were questions regarding the participant’s age, sex, location, practice type, years in practice, and volume of low-energy lateral ankle injuries treated annually. Similar questions were asked for both AS and SH-1 regarding diagnostic criteria and preferred treatment, including immobilization and weightbearing status. We also queried for experience with complications associated with each fracture, complications associated with treatments (ie, complications associated with bracing and casting), and complications associated with neglected treatment. We excluded injury recurrence as a complication, as this has been described previously as a known sequela of lateral ankle injuries and is not exclusive to pediatrics. 1,14,17,20,23,30
Statistical Analysis
Comparisons of paired responses to survey questions for AS and SH-1 were performed using the McNemar test. Variables were compared between responses regarding AS and SH-1 as independent responses from each participant. Comparisons of treatment variation were made based on respondents’ years in practice, sex, age (30s, 40s, 50s, or ≥60 years), region of the United States (East, Midwest, South, or West), institution type (academic hospital or private/solo practice), and annual volume of lateral ankle injuries (high [≥10 patients] or low [<10 patients]). Chi-square or Fisher exact test was used for categorical variables, and analysis of variance was used for continuous variables. Data were summarized, and descriptive statistical analysis was performed for complications. For all statistical comparisons, the threshold for significance was set at P < .05.
Results
Study Participants
A total of 229 surveys were collected over the 6-week study period, for a response rate of 16.4%. The characteristics of the survey respondents are shown in Table 1. The mean age of participants was 49.9 years, 24% were women, female respondents were younger than male respondents (44.23 vs 51.64 years, respectively, the participants had been in practice for a mean of 16.9 years, and half of them practiced at an academic pediatric hospital.
Characteristics of the Survey Respondents (N = 229) a
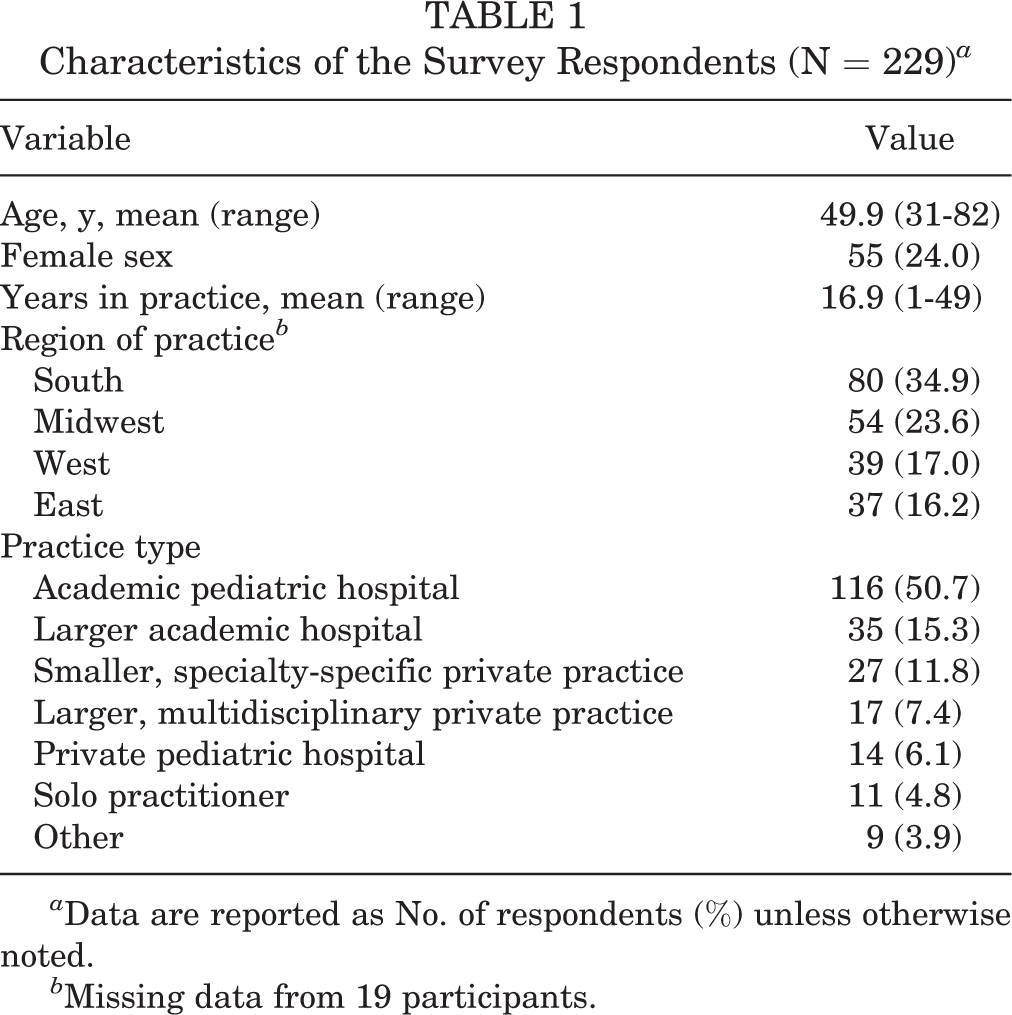
a Data are reported as No. of respondents (%) unless otherwise noted.
b Missing data from 19 participants.
Clinical Diagnosis of AS and SH-1
A majority of respondents used physical examination (n = 223; 97.4%) to assist with the diagnosis of AS versus SH-1, although only 25.7% used physical examination exclusively to make the distinction (Table 2). MRI and ultrasonography were rarely used to aid in the diagnosis of both AS and SH-1.
Responses Regarding Clinical Diagnosis of Ankle Sprain Versus Salter-Harris Type 1 Injury a

a Data are reported as No. of respondents (%).
Variation in Treatment Between AS and SH-1 Injury
Immobilization was more likely to be the preferred primary treatment for SH-1 versus AS (94.8% vs 78.2%, respectively; P < .01); 17.9% of respondents used immobilization for SH-1 but not for AS (Table 3). Crutches were not used for either AS or SH-1 in 58.1% of participants. The majority of respondents did not recommend physical therapy (outpatient or home program) for either injury (66.4%); however, 32.8% recommended physical therapy for AS compared with only 11.4% for SH-1 (P < .01). Most participants preferred weightbearing as tolerated for both injuries; however, ASs were significantly more likely to be treated with weightbearing as tolerated (P < .01). A controlled ankle motion (CAM) or walking boot was the most commonly reported form of preferred immobilization for both AS (46.3%) and SH-1 (55.6%). The majority of respondents indicated return to play in 3 to 4 weeks for AS (60.2%); almost half recommended 5 to 6 weeks for SH-1 (48%; P < .01).
Responses Regarding the Evaluation and Treatment of a First-Time Ankle Sprain or Salter-Harris Type 1 Injury a
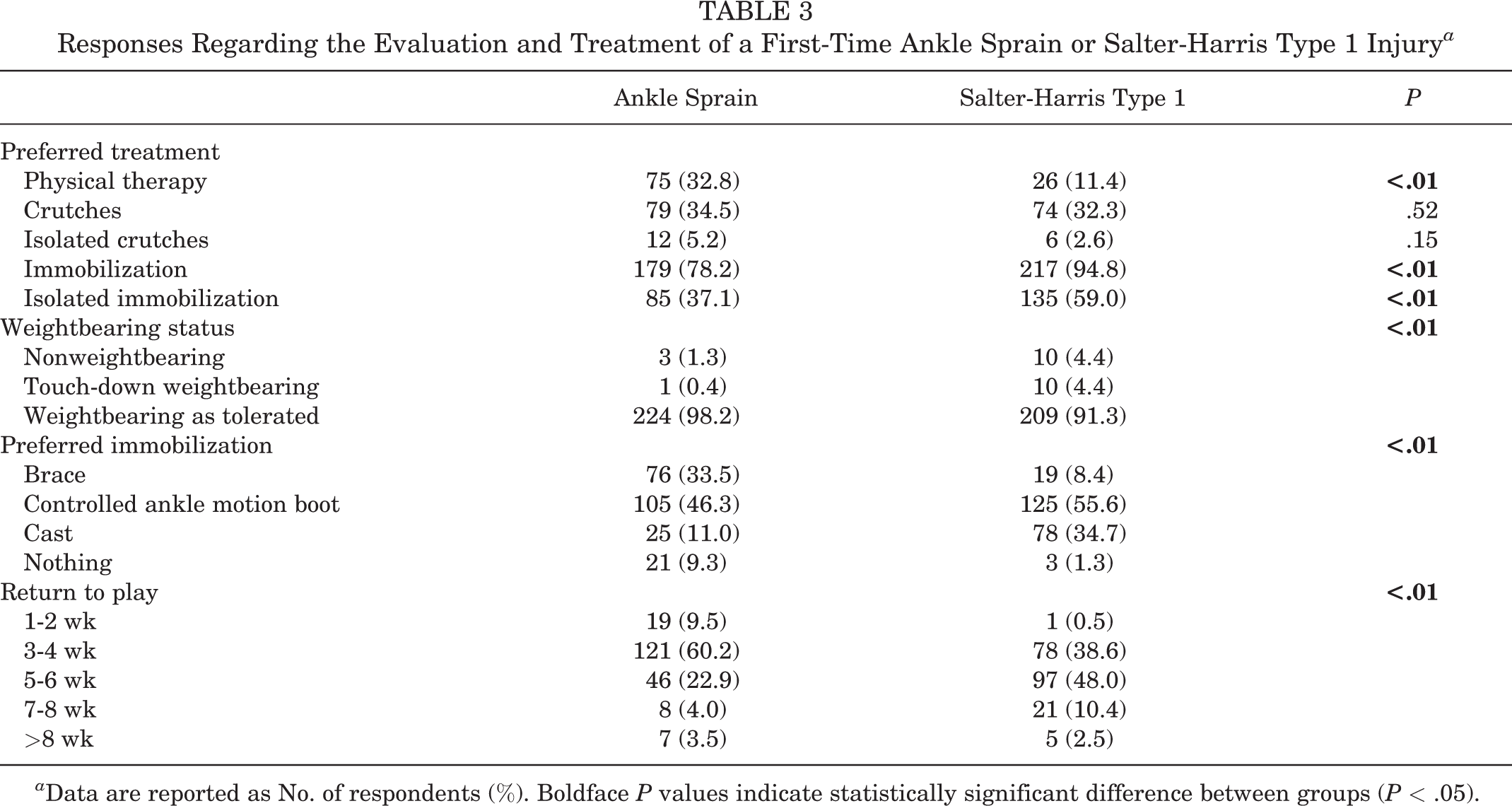
a Data are reported as No. of respondents (%). Boldface P values indicate statistically significant difference between groups (P < .05).
Variation by Respondent Sex and Age
Female respondents were significantly more likely to recommend physical therapy than were male respondents for both AS (47.3% vs 28.7%, respectively; P = .01) and SH-1 (20.0% vs 8.8%, respectively; P = .02). All of the female respondents (100%) recommended immobilization as primary treatment for SH-1, and 93% of male respondents recommended this (P = .04) (Table 4). Respondents in their 30s were most likely to report physical therapy as a primary form of treatment for AS when compared with participants in their 40s, 50s, or 60s and older (P < .03) (Table 5). No other age- or sex-based differences in primary treatment or weightbearing status were noted. The only significant regional treatment variation was in weightbearing status; respondents from the East and Midwest were more likely to restrict weightbearing after SH-1 than were those from the South or West (East, 10.8%; Midwest, 13.0%; South, 0; West, 2.6%; P = .01).
Treatment Variation by Respondent Sex a

a Data are reported as No. of respondents (%). Boldface P values indicate statistically significant difference between groups (P < .05).
Treatment Variation by Respondent Age a

a Data are reported as No. of respondents (%). Boldface P value indicates statistically significant difference between groups (P < .05).
Variation in Preferred Immobilization Type
Regarding AS injuries, the only significant difference in immobilization preference occurred between high- and low-volume practitioners (Table 6). The majority of low-volume participants preferred CAM boot immobilization over brace or cast (CAM, 53.8%; brace, 27.7%; cast, 7.6%); however, greater variation was seen among high-volume participants (CAM, 38.0%; brace, 39.8%; cast, 14.8%) (P = .02). For AS, all age groups were most likely to prefer CAM boot immobilization (30s, 45.6%; 40s, 52.3%; 50s, 55.1%) except for respondents ≥60 years, who preferred bracing (48.2%) (P = .16). Regarding SH-1 fractures, the CAM boot remained the primary form of immobilization (30s, 68.4%; 40s, 53.1%; 50s, 60.4%) except among those ≥60 years of age. For SH-1, unlike AS, almost half of participants ≥60 years of age preferred cast immobilization (42.9%; P = .03). On average, participants who preferred brace immobilization were older (55.84 ± 12.16 years) than participants who preferred cast (51.77 ± 12.70 years), CAM boot (48.12 ± 11.22 years), or nothing (40.67 ± 6.51 years) (P = .01). No significant differences were found regarding immobilization preference for AS or SH-1 based on region or type of institution (Table 6).
Variation in Type of Immobilization According to Respondent Characteristics a

a Data are reported as No. of respondents (%). Boldface P values indicate statistically significant difference between groups (P < .05). CAM, controlled ankle motion.
b Number of low-energy lateral ankle injuries treated annually.
Variation in Return-to-Play Times
The only significant variation in recommended time to return to play was by institution type for AS injury, in which there was greater variation among participants at academic institutions (1-2 weeks, 6.0%; 3-4 weeks, 60.2%; 5-6 weeks, 24.1%; 7-8 weeks, 6.0%; >8 weeks, 3.8%) than those in private or solo practice (1-2 weeks, 15.9%; 3-4 weeks, 63.5%; 5-6 weeks, 20.6%; 7-8 weeks, 0%; >8 weeks, 0%) (P = .03) (Table 7).
Variation in Return-to-Play Times According to Respondent Characteristics a

a Data are reported as No. of respondents (%). Boldface P value indicates statistically significant difference between groups (P < .05).
Injury-Related Complications
Injury-related complications were reported by 8.7% of those treating SH-1 injuries and 6.6% of those treating AS injuries, with almost twice as many injury-related complications being reported for SH-1 versus AS (32 vs 17 injuries, respectively). Table 8 summarizes the injury-related complications reported.
Injury-Related Complications Reported During Treatment a

a Data are reported as No. of respondents (%).
Treatment-Related Complications
Reported complication rates were low, with 81.2% of participants reporting no complications from SH-1 treatment and 87.8% reporting no complications from AS treatment. When treating SH-1, 9.6% of participants reported cast complications, whereas 2.6% reported brace complications. When treating AS, 5.2% of participants reported cast complications, and 3% reported brace complications (Table 9).
Treatment-Related Complications a

a Data are reported as No. of respondents (%).
Complications Due to Neglected Treatment
Previously undescribed complications from neglected treatment of SH-1 and AS were reported, with SH-1 having nearly twice the complication rate of AS (32 vs 17 complications, respectively). Displacement of fracture, growth disturbance, and nonunion were reported by participants when treating SH-1 injuries. One participant each reported an ankle fracture/dislocation and osteochondritis dissecans/nonunion after AS. Chronic pain was the most commonly reported complication in both injuries (Table 10).
Complications Due to Neglected Treatment a
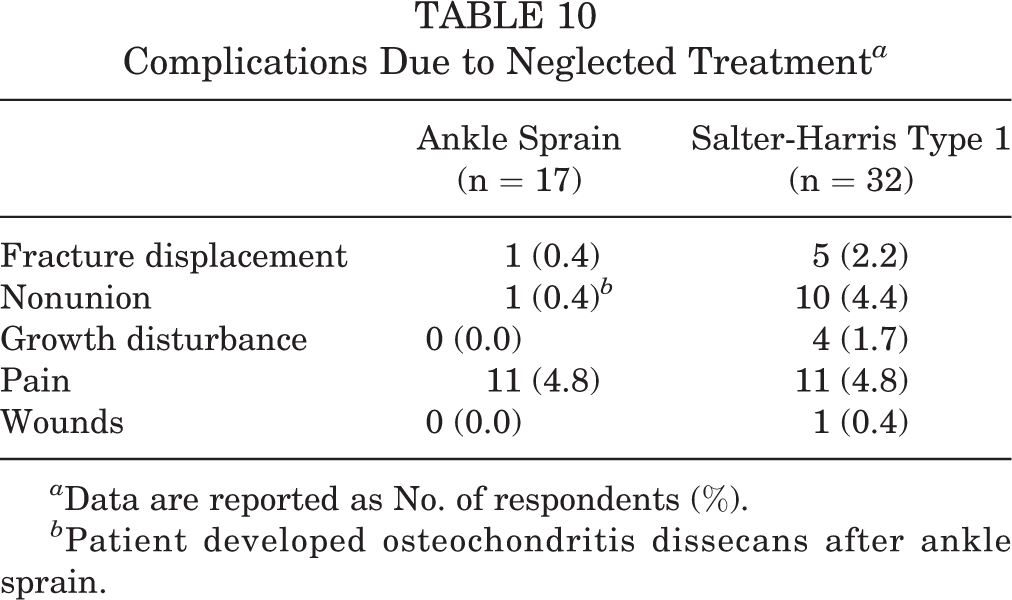
a Data are reported as No. of respondents (%).
b Patient developed osteochondritis dissecans after ankle sprain.
Discussion
Although lateral ankle injuries are among the most common injuries in pediatric patients, this study revealed significant variability in both the diagnostic method and the treatment of these injuries. Of 229 respondents, 27.7% of participants distinguished between AS and SH-1 by using examination only, whereas 18.7% of participants performed serial radiography to aid with diagnosis, demonstrating a differing standard of care for patients with lateral ankle injury dependent on treating physician. A CAM or walking boot was the most common immobilization technique for both AS (46.3%) and SH-1 (55.6%); however, bracing was the second most common in AS (33.5%), and casting was the second most common in SH-1 (34.7%), again displaying the variability in physician discretion on injury management. Furthermore, physical therapy treatment was recommended by one-third of all participants for AS, whereas only 11.4% recommended physical therapy for SH-1 (P < .01). Complication rates after treatment varied by type of lateral ankle injury as well. AS treatment had a higher rate of no complications reported (87.8%), whereas SH-1 treatment had no complications 81.2% of the time. These varying treatments and subsequent complication rates are important to understand in order to expand future research questions as well as improve the quality and value of the diagnosis and treatment of this injury.
Low-energy, lateral ankle injuries in pediatric patients are commonly diagnosed and treated within the pediatric orthopaedic community; however, there is very little understanding and consensus on diagnosis, treatment, and outcomes of these injuries. 3,5,9,11 In an effort to improve quality, safety, and value for pediatric athletes, this study has provided information about injury complications, various treatment complications, and complications from neglected treatment. Before we can understand how to improve our treatment of these injuries, the pediatric orthopaedic community must understand the risk of under- or overtreatment. SH-1 injuries had higher rates of reported injury complications compared with AS injuries (Table 9). Increased complications with cast treatment were noted in both injury types. Continued pain or reflex sympathetic dystrophy was the most common complication in both AS and SH-1 (Table 8). Distal fibular growth arrest, fracture displacement, postinjury infection, and nonunion after SH-1 have not been previously reported.
Although rare, significant complications from pediatric ASs and nondisplaced fibular fractures do occur. Even though they consider these injuries minor and routine with short-term follow-up, pediatric orthopaedic surgeons should carefully evaluate patients for these complications, be vigilant about explaining potential complications, provide reasons for return for evaluation, and assist in prevention of these adverse outcomes. Numerous studies have reported on risk factors for recurrence, such as body mass index, sport choice, height, sex, use of artificial turf, and poor balance, 10,13,16,20,23,28,31 which should be evaluated and discussed with each patient. Collaboration with athletic trainers, coaches, and athletic directors should emphasize lateral ankle injury prevention techniques including neuromuscular training for strength, balance, and agility as part of sports participation. 18,19 Unfortunately, not enough research has been completed to evaluate the use of ankle braces in primary ankle injury prevention. However, use of ankle braces has been shown to prevent recurrence of lateral ankle injuries in pediatric football players. 19
A recent systematic review determined there is a lack of high-quality, high-level evidence on SH-1 and AS injuries in pediatric patients. 3 The authors of that review discussed overdiagnosis, excessive imaging (radiography, ultrasonography, and MRI), and overtreatment, with the resulting conclusion that AS injuries have a much higher percentage of actual diagnosis than do SH-1 injuries. Additionally, data showed that treatment with limited immobilization had outcomes that were equal to or better than outcomes of cast immobilization. A high recurrence rate of AS was found, and several risk factors for initial and recurrent injury, such as high body mass index, increased height, artificial turf, poor single-leg balance and hop testing, and poor Star Excursion Balance Test results, were identified. 10,13,16,20,23,28,31 However, none of the studies found complications, except recurrence, that were attributable to the actual injury, medical treatment, or neglected treatment. The paucity of literature regarding both outcomes and complications associated with this frequent injury has led to significant variability in practice, which has given rise to inconsistent treatment, unmet patient expectations, and overall potential loss in quality and value of care. 24 Survey responses indicated that variation exists in the treatment of both AS and SH-1 that may be associated with the practitioner’s sex, age, or volume of practice. A reduction of clinical practice variation should be considered for this common condition, yet evidence-based literature is needed to reduce this variation.
CAM boot immobilization was the most commonly reported immobilization method for AS and SH-1 in our survey, especially within early and midcareer respondents. Boutis et al 6 performed a randomized controlled trial comparing the use of a CAM/walking boot with a short leg cast after a pediatric lateral ankle injury. Primary outcomes in this series were short-term (4-week) physical function and patient preference. Patients treated with the walking boot returned to activity sooner and had higher activity scores than did those treated with a cast. That study demonstrated a strong preference for the walking boot but no complications in treatment with either option. 6 A second randomized controlled trial compared the use of the Air-Stirrup ankle brace versus a posterior splint and did not find a difference in functional outcomes; however, the ankle brace had more favorable outcomes in the older patients (11-15 years old) whereas the posterior splint was more favorable in the younger group (5-10 years old). 2 Despite the clear results from randomized controlled trials, variability continues to exist regarding immobilization, weightbearing status, and return to sports according to this survey and other published opinions. 3,9,11,12,22,34 For such a common injury, further high-level studies or the development of clinical pathways should be considered for these low-energy lateral ankle injuries.
Differences in treatment based on sex of respondents was a surprising finding, as female respondents were more likely to prescribe physical therapy in both AS and SH-1 injuries. This difference may be associated with the patient populations that female respondents treat; a recent systematic review suggested that female sex was a predictor of a poor recovery after an acute ankle injury. 29 In the current survey, female respondents were younger than male respondents (44.23 vs 51.64 years, respectively), which may have influenced their recommendations to pursue physical therapy, as younger respondents were more likely to recommend physical therapy compared with older respondents. Thus, an early career stage of pediatric orthopaedic surgeons along with the understanding that young female athletes are more likely to sustain recurrent ankle injuries and have worse outcomes may explain this clinical decision making. 21,28
SH-1 injuries entailed a longer timeline for return to sports, and casts were used more often in SH-1 compared with AS injuries. These differences in treatment remain peculiar. The accuracy of diagnosis between SH-1 and AS is in question; most lateral ankle injuries, regardless of location of tenderness, are confirmed on MRI scans as AS without physeal involvement.4,5 At least for some physicians, parents, and patients, a fracture diagnosis may warrant aggressive treatment in a cast as opposed to a removable walking brace, given beliefs that injury to a bone is more serious than injury to a ligament. Nondisplaced SH-1 fractures have a stable fracture pattern with late displacement not previously reported. Immobilization is essentially used to treat patients’ symptoms, as these injuries heal quickly with few complications. A synonymous injury in the upper extremity, because of its frequency and benign nature, is the buckle fracture of the distal radius. Two large, randomized controlled trials evaluated the use of a removable volar splint compared with a cast. 25,33 In both of these series, the removable volar splint proved to be convenient and cost-effective, yield higher satisfaction, and minimize clinical follow-up. The known timeline for complete healing of this injury is thought to be 3 weeks. Similar, larger randomized clinical trials are needed in order to determine standardized and cost-effective treatment of SH-1 distal fibular fractures.
Biological healing of a ligament alters collagen structure in comparison with bone healing, meaning that injury to the anterior talofibular ligament and calcaneofibular ligament may be an adequate rationale for a delayed return to play. Whereas SH-1 distal fibular fractures return to normal anatomic status, ligament injuries typically heal in an elongated fashion with disorganization of collagen, proteoglycans, and glycoproteins reducing the tissue’s overall tensile strength. 3 This can lead to chronic ankle instability, which can be a significant concern in the adolescent athlete. 1,16 The use of an ankle brace upon return to activity is an effective strategy to prevent future instability. 8 An emphasis for function over timing should be encouraged among young athletes before return to sports. Athletes should regain full motion and strength and undergo balance and proprioception training of the injured ankle, which will prevent recurrent ankle injuries. 27 Return-to-sports criteria should continue to evolve and be formalized based on risk for recurrence.
A cost-effective model, knowledge of intermediate-term outcomes, and understanding of complications associated with treatments still need to be developed. Based on 1 study, use of a walking boot compared with a cast was a cost-effective treatment option for pediatric lateral ankle instability. 6 Intermediate outcomes and return-to-play outcomes are unclear, especially with AS, because most of the existing literature pertains to the skeletally mature athlete and not the pediatric patient. Standardization of treatment and return-to-play criteria may help decrease complications and improve outcomes.
Study Limitations
Limitations of this study include those inherent to a survey in which respondent participation is voluntary and not controlled. This may present bias in those willing to participate based on interest in pediatric lateral ankle injuries. Another limitation is the response rate of 16.4%, which, although low, appears to be consistent with other published surveys. Also, comparative analysis of treatment differences among the respondents, although interesting, may not provide a true reflection of the specified group. The survey format limited effective explanation of some reported complications, such as ankle fracture/dislocation and osteochondritis dissecans/nonunion after AS. Additionally, these injury types may be treated by nonorthopaedic surgery colleagues, resulting in missing data. Despite these limitations, this is the only study to report on these complications. The survey was intended to determine rare complications and not address recurrence. The survey questions were intended to be broad and nonspecific rather than pertain to discrete clinical scenarios. Although clinical vignettes may have more clearly described the exact patients in question, the purpose of this survey was to develop a broad, generalizable understanding of the current variation in treatment of lateral ankle injuries. These limitations identify several areas for future research.
Conclusion
We found significant variability in primary treatment and immobilization of pediatric AS injuries and SH-1 distal fibular physeal fractures, and this variability appeared to be primarily based on age, sex, and experience of the treating surgeon. Pediatric patients with AS were more likely to undergo physical therapy and receive a recommendation for earlier return to sports, whereas patients with SH-1 were more likely to undergo cast immobilization. Increased complications with cast treatment were noted in both injury groups. Continued pain/reflex sympathetic dystrophy was a common complication in both AS and SH-1. Participants reported rare complications, such as nonunion, growth arrest, recurrent fracture, and infection, due to injury, treatment, and neglected treatment after SH-1 and AS.
Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/232596712211000223.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221100223 - Treatment Variability and Complications Associated With Pediatric Lateral Ankle Injuries: A POSNA Quality, Safety, and Value Initiative Survey
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221100223 for Treatment Variability and Complications Associated With Pediatric Lateral Ankle Injuries: A POSNA Quality, Safety, and Value Initiative Survey by Jennifer J. Beck, Connor M. Carpenter, Nicole West, Meagan J. Sabatino and Henry B. Ellis in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgment
The authors thank Chan-Hee Jo, PhD, senior biostatistician, Department of Research, Scottish Rite for Children, for her assistance with the organization and interpretation of the data collected in this survey. The authors also thank the POSNA Quality, Safety and Value Initiative Committee for providing feedback for the survey design and assisting with survey distribution. Finally, the authors thank the POSNA members who participated in the survey.
Final revision submitted January 26, 2022; accepted February 17, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.J.B. has received education payments from Arthrex and hospitality payments from Smith & Nephew. H.B.E. has received education payments from Pylant Medical; speaking fees from Pylant Medical, Smith & Nephew, and Synthes; and hospitality payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.