
Abstract
Background:
Arthroscopic debridement of the extensor carpi radialis brevis (ECRB) tendon is a widely accepted procedure used in refractory lateral epicondylitis. However, residual pain occurs in some patients.
Purpose:
To investigate the clinical effectiveness of arthroscopic extended debridement (ECRB tenotomy and debridement) in the treatment of lateral epicondylitis.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients with refractory lateral epicondylitis were consecutively recruited for this study. They underwent traditional ECRB debridement (control group) or extended ECRB debridement (ED group) under arthroscopy. The Disabilities of the Arm, Shoulder and Hand (DASH) score, visual analog scale (VAS) for pain, and Mayo Elbow Performance Score (MEPS) were used to compare elbow function between the groups at 3, 6, and 12 months postoperatively. Magnetic resonance imaging (MRI) was also performed to evaluate pathology at 12 months.
Results:
A total of 69 patients participated in the study (33 patients in the ED group and 36 in the control group). After surgery, all patients showed improvement on all 3 outcome scores. Compared with the control group, the ED group had significantly better postoperative MEPS and VAS scores at 3 months (P ≤ .001 for both) and 6 months (P ≤ .03 for both) but similar values at 12 months. DASH scores between groups were similar at all time periods. At the 12-month follow-up, no patients in the ED group reported pain with strenuous work. Return-to-work (RTW) times were also shorter in the ED group compared with the controls (8 ± 4 vs 18 ± 8 weeks; P < .001). Postoperative MRI assessments revealed no high signal intensities on the lateral epicondyle in the ED group, while there was an increased internal signal intensity on the lateral epicondyle in 83% of the controls.
Conclusion:
Collectively, the extended ECRB debridement technique resulted in enhanced pain relief in the early postoperative period as well as providing faster RTW times compared with the traditional debridement technique. At 1 year follow-up, there were no differences in outcome measures between groups, but residual abnormal MRI findings were more common in the traditional debridement group.
Lateral epicondylitis, referred to as “tennis elbow,” is the most common elbow disease in middle-aged patients, with an approximate prevalence rate of 1% to 3%. 3,36 The extensor carpi radialis brevis (ECRB) is the elbow tendon most frequently involved due to overuse and repetitive stress activities. 12,26 Histopathological studies of the ECRB in lateral epicondylitis have revealed a degenerative process characterized by tendon fibers showing microtears, angiofibroblastic hyperplasia, fibrosis, disorganized loose collagen, and osseous calcification. 1 A recent review reported that nonsurgical treatments might fail for some refractory cases. 23 The available evidence shows that 10% to 16% of patients may need surgical treatment if symptoms are not resolved within 6 months of onset. 18,35,38
Various surgical techniques have been reported for the treatment of lateral epicondylitis. 9,11,22,29,34,40,43 An increasingly popular, and less invasive, alternative involves arthroscopic debridement of the ECRB origin, which is also able to address some concomitant intra-articular pathologies. 5,17,20,33 Indeed, some studies have reported that arthroscopic ECRB debridement is effective in terms of both restoring elbow function and providing pain relief. 7,25,39 Other reported advantages of arthroscopic surgery include the improvement of symptoms, earlier return to work (RTW), and shorter recovery periods compared with open surgery. 4,13,32 However, it is evident that some patients still experience pain after arthroscopic debridement surgery. 4,14,21 Kwon et al 19 found that 2 patients (6.9%) still had poor outcomes after arthroscopic debridement treatment of chronic lateral elbow tendinopathy at a mean follow-up of >31 months. They proposed that arthroscopic debridement could not completely remove the tendinosis at the ECRB origin, as visualization of the full extent of the ECRB insertion at the lateral epicondyle was difficult using a 30° arthroscope. Moreover, Cummins 8 reported that residual microscopic tendinopathy was frequently present after arthroscopic debridement and, notably, this was associated with affected patients reporting worsened pain levels. Such reports have driven an ongoing controversy regarding the necessity to remove more pathologic tissue during the arthroscopic debridement of the ECRB.
In addition, magnetic resonance imaging (MRI) is the noninvasive tool used most widely for diagnosing lateral epicondylitis, showing excellent accuracy for the evaluation of ECRB tendon origin abnormalities. 6 Therefore, the purpose of the current study was to investigate the clinical effectiveness of the extended debridement (ED) technique (ECRB tenotomy and debridement) and to evaluate the ECRB tendon origin in the treatment of lateral epicondylitis. Our hypothesis was that extended ECRB debridement would provide better functional outcomes in patients with lateral epicondylitis compared with conventional debridement, along with reductions in postoperative recovery times. The second hypothesis was that there would still be an increased internal signal intensity on the lateral epicondyle of the traditional debridement group based on MRI scans.
Methods
Study Population
This prospective study was approved by the institutional review board of our hospital. All patients who underwent arthroscopic treatment of refractory lateral epicondylitis between April 2014 and April 2020 were recruited in this study. Surgical treatment was suggested for patients who still had pain after at least 6 months of conservative management. All patients signed informed consent.
The inclusion criteria were as follows: (1) clinical diagnosis of lateral epicondylitis (a characteristic history of activity-related pain, palpable tenderness, and provoked pain at the lateral epicondyle), (2) full range of motion at the elbow and wrist, (3) age >18 years, (4) a minimum of 6 months of failed conservative treatment (including brace, steroid injection, shock wave, physical therapy, etc), and (5) follow-up time of 1 year after surgery. Participants were excluded if they had any of the following: (1) previous surgical treatment for lateral epicondylitis, (2) elbow osteoarthritis, (3) large-sized osteochondral defect (OCD), or (4) neurological symptoms.
Surgical Techniques
A senior surgeon (X.Z.) with extensive experience in elbow surgery performed all operations. Procedures were performed with the patient in a lateral position with the affected elbow at 90° of flexion. The limb was prepared and draped free in the usual manner. A proximal anteromedial portal (2 cm proximal and 1 cm anterior to the medial epicondyle) and a proximal anterolateral portal (2 cm proximal and 1 cm anterior to the lateral epicondyle) were used to assess the joint.
First, a full intra-articular joint inspection was performed via the proximal anteromedial portal with simultaneous assessment of the intra-articular pathology. Using the medial portal, the surgeon visualized the lateral capsule and ECRB tendon via a 30° arthroscope. The pathologic findings in the capsule and ECRB tendon were classified into 3 types (type I, smooth capsule; type II, capsule tear; type III, complete rupture and retraction of the capsule with fraying of the ECRB tendon) according to a previously reported scheme. 3 Next, arthroscopic ECRB debridement or ED was performed according to the following procedure. The traditional debridement ECRB technique was performed mainly at the beginning of the study period. The chief surgeon had concerns after limited debridement that some patients had residual pain so he switched to the ED technique. The ED ECRB technique (tenotomy and debridement) technique was introduced gradually.
In the traditional debridement group (control group), the capsule overlying the ECRB was debrided using a shaver to expose the proximal part of the extracapsular ECRB. Pathologic or degenerated tissue on the lateral epicondyle was debrided at the proximal ECRB tendon origin using a radiofrequency wand and shaver. Debridement was limited anteriorly to the midline of the radial head to avoid injuries to the lateral ulnar collateral ligament (LUCL). Finally, the skin incisions were closed using sterile bandages.
In the ED group, the capsule overlying the ECRB was first debrided using a shaver to expose the ECRB. Thereafter, the ECRB tendon was transected completely using scissors or radiofrequency wand at approximately 5 to 10 mm from the origin site. Then, the remnant ECRB tendon origin tissue on the lateral epicondyle was debrided completely. Finally, the skin incisions were closed using sterile bandages (Figure 1).

Arthroscopic images. (A) Debridement technique. Pathologic or degenerated tissue on the lateral epicondyle was debrided via the lateral portal at the proximal ECRB tendon origin of a right elbow. (B) Arthroscopic appearance (anterior medial portal) after debridement technique in a right elbow. (C) Extended debridement technique. The extensor carpi radialis brevis (ECRB) tendon was completely transected and ECRB remnant tissue was debrided via the lateral portal on the lateral epicondyle of a right elbow. (D) Arthroscopic appearance (anterior medial portal) after extended debridement technique in a right elbow.
Postoperative Management
Postoperative standard rehabilitation protocols were the same in both groups. Surgical sites were initially covered in soft wound dressings. Range of motion elbow exercises were started at day 2 after surgery if there was no pain. Strengthening and resistance activities were allowed 6 weeks postoperatively. Patients were allowed to RTW at 4 to 6 weeks after surgery.
Assessment of Clinical Function
Elbow function was evaluated at 3, 6, and 12 months after surgery for both groups. The primary outcome measures involved Mayo Elbow Performance Score (MEPS) and the Disabilities of the Arm, Shoulder and Hand (DASH) outcome score. 16 The DASH questionnaire is a widely used region-specific questionnaire that has shown reliability, validity, and responsiveness in both proximal and distal disorders of the upper extremity. 30 Subjective pain was ranked by the patients on a visual analog scale (VAS), where 0 indicated that the functional condition of the elbow had worsened after surgery and 10 indicated that the recovery perfectly met or even exceeded expectations. Patient-administered elbow function was evaluated using the MEPS, which consists of 4 parts: pain, stability, ulnohumeral motion, and the ability to perform 5 functional tasks. 2,24 For MEPS, the best possible score is 100, with scores >90 points indicating excellent elbow function. Grip strength, expressed in kilograms, was measured using an electronic hand dynamometer (EH101; KYTO Fitness Technology), and strength was measured via maximum force on the affected side at 12 months after surgery. Grip strength was measured 3 times at 30-second intervals and averaged.
MRI Scan and Analysis
MRI of the affected elbow was performed preoperatively and at final follow-up with the elbow in a relaxed extended position using a 1.5-T MRI scanner (GE Medical Systems). The sequences included mainly oblique sagittal T1, oblique coronal proton density-fat saturation (PD-FS), oblique coronal T2 FS, and oblique axial T2 FS. All images were imported into Radi-Ant DICOM viewer 4.0.3 software (Medixant) for analysis.
Preoperative and postoperative MRI evaluation focused mainly on evaluation of the ECRB tendon origin (usually on the anterior slice) and abnormalities as well as LUCL injuries (usually on the posterior slice) on the lateral epicondyle according to a previous study. 6 The ECRB tendon insertion was classified as follows: grade 0, complete homogenous low signal intensity without tendon thickening; grade 1, tendon thickening or thinning with increased internal signal intensity; grade 2, a fluid-filled gap affecting 20% to 80% of the thickness; and grade 3, a fluid-filled gap affecting >80% of the thickness (Figure 2). 6 The LUCL was classified as follows: grade 0, complete homogenous low signal intensity with normal LUCL; grade 1, a thickened LUCL characterized by normal to increased signal intensity without interruption; grade 2, ligament thinning with increased signal intensity in and surrounding the ligament; and grade 3, a complete rupture and discontinuity of the fibers with fluid-like intensity (Figure 3).
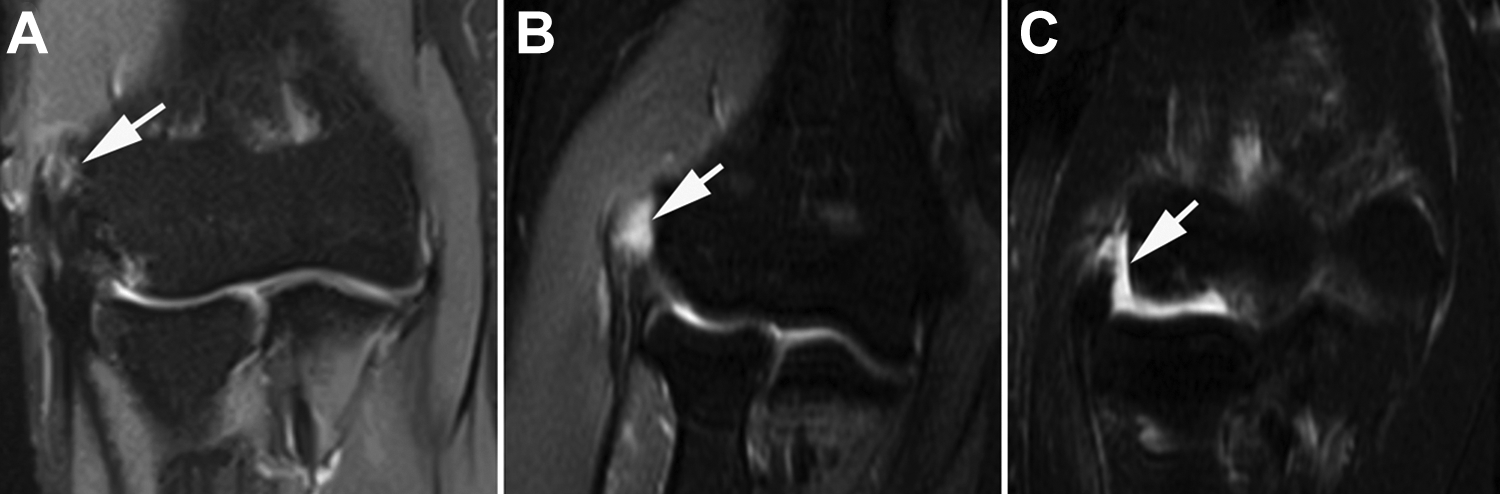
Extensor carpi radialis brevis classification based on magnetic resonance imaging scans of right elbows. (A) Grade 1, tendon thickening or thinning with increased internal signal intensity (white arrow). (B) Grade 2, a fluid-filled gap (white arrow) affecting 20% to 80% of the thickness. (C) Grade 3, a fluid-filled gap (white arrow) affecting >80% of the thickness.

Lateral ulnar collateral ligament classification based on magnetic resonance imaging scans of right elbows. (A) Grade 0, complete homogenous low signal intensity (white arrow) without ligament thickening.; (B) Grade 1, thickened ligament characterized by normal to increased signal intensity (white arrow) without interruption.; (C) Grade 2, ligament thinning with increased signal intensity (white arrow) in and surrounding the ligament.; (D) Grade 3, a complete rupture and discontinuity of the fibers with fluid-like intensity (white arrow).
Statistical Analysis
Data analysis was performed using Stata 10.0 software (Stata Corp). A post hoc power analysis was performed based on the functional score (MEPS) data. A difference of at least 3 points in MEPS between the groups was considered significant. 22 Based on the standard deviation of the MEPS, power calculation analysis indicated that a sample size of at least 23 patients in each group would be required to identify a difference of 3 points in the MEPS at a power of 0.80. 22 Comparisons between groups were made using Student t test or 2-sample Wilcoxon rank sum test for continuous variables according to the normality and homogeneity of variances. The chi-square test or Fisher exact test was used to compare categorical variables. Spearman correlation coefficients were calculated between the postoperative VAS scores and preoperative characteristic data. A 2-tailed P value <.05 was set for statistical significance.
Results
A total of 76 patients (36 in the ED group and 40 in the control group) underwent arthroscopic treatment of refractory lateral epicondylitis between April 2014 and April 2020. Of these, 3 patients in the ED group and 4 in the control group were lost to follow-up. Ultimately, 69 patients were recruited and completed the follow-up: 33 patients in the ED group and 36 in the control group.
The characteristic data of the study participants are shown in Table 1. No significant differences were found on any characteristic between the groups. Concomitant injuries were identified at arthroscopy, and these lesions were treated with debridement only. There were 2 patients in the ED group with small-sized OCDs and 1 patient with loose elbow bodies. In the control group, 3 patients had small-sized OCDs, and 1 presented with elbow plica. No significant difference was found between the ED and control groups regarding OCD incidence (6% vs 8%; P = .92).
Characteristic Data of the Study Groups a
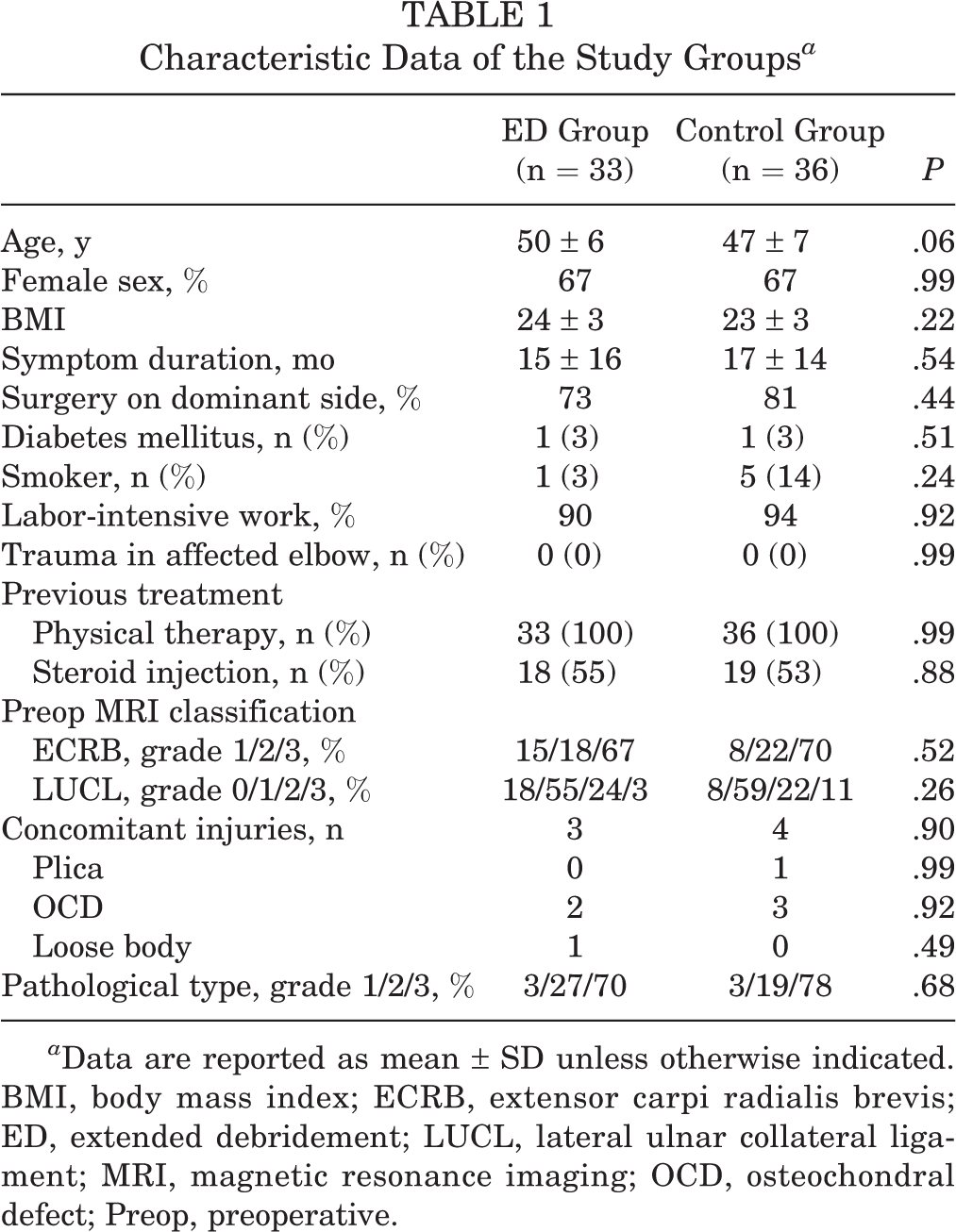
a Data are reported as mean ± SD unless otherwise indicated. BMI, body mass index; ECRB, extensor carpi radialis brevis; ED, extended debridement; LUCL, lateral ulnar collateral ligament; MRI, magnetic resonance imaging; OCD, osteochondral defect; Preop, preoperative.
Complications
At final follow-up, no operative complications were noted for any patients, and all reported normal elbow range of motion. No patient in either group required revision surgery.
Clinical Outcomes
Importantly, there were no significant differences between the ED and control groups regarding preoperative DASH score (66 ± 4 vs 65 ± 2; P = .19), MEPS (59 ± 4 vs 60 ± 2; P = .22), or VAS score (5 ± 1 vs 5 ± 1; P = .50). After surgery, both groups exhibited clinical improvement, with increased MEPS along with decreases in DASH and VAS scores (Figure 4).

Pre- and postoperative outcomes for the (A) DASH, (B) MEPS, and VAS for pain. DASH, Disabilities of the Arm, Shoulder and Hand; ED, extended debridement; MEPS, Mayo Elbow Performance Score; VAS, visual analog scale.
At 3 months after surgery, there was no significant difference in DASH scores between the ED and control groups (45 ± 12 vs 50 ± 12; P = .16). However, compared with the control group, the ED group exhibited higher MEPS (86 ± 6 vs 81 ± 8; P = .001) and lower VAS score (2 ± 1 vs 3 ± 1; P < .001). At this time point, 1 patient in the ED group and 4 patients in the control group still reported pain with strenuous work (P = .41).
Similarly, at the 6 month follow-up, DASH scores for the ED and control groups remained the same (38 ± 11 vs 38 ± 9; P = .88), and the differences between groups observed at 3 months were maintained, with significantly higher MEPS (91 ± 7 vs 87 ± 8; P = .03) and lower VAS score (1 ± 1 vs 2 ± 1; P = .01) for the ED group. Only 1 patient in the control group now reported pain resulting from strenuous work.
At the final follow-up at 12 months, there were no significant differences found between the ED and control groups for DASH score (39 ± 12 vs 34 ± 7; P = .06), MEPS (91 ± 7 vs 89 ± 8; P = .36), or VAS score (1 ± 1 vs 1 ± 1; P = .06). Based on postoperative VAS scores, 33 patients in the ED group and 35 in the control group obtained improvement in pain. Again, only 1 patient in the control group reported pain resulting from strenuous work, whereas no patients in the ED group reported pain from strenuous work (P = .99).
There were no significant differences in grip power between the ED and control groups (31 ± 9 kg vs 34 ± 11 kg; P = .25) at 12 months. The RTW time for the ED group was 8 ± 4 weeks, which was significantly lower than that of the control group (18 ± 8 weeks) (P < .001).
MRI Scan Evaluation
In 83% of the control group, the ECRB insertional site had somewhat increased internal signal intensity (grade 1) on the lateral epicondyle postoperatively (Figure 5). In the patient who still experienced pain during work, MRI scans revealed that the ECRB insertional site had high-intensity signal on the lateral epicondyle (Figure 6). However, in the ED group, there was no covering pathological tissue on the epicondyle (Figure 7). There was a significant difference of ECRB tendon signal intensity between groups (P < .001).

Preop and 1-year Postop MRI scans of a right elbow from the control group. Two consecutive slices (AS and PS) were chosen to reveal the extensor carpi radialis brevis (short white arrow) and LUCL. AS, anterior slice; LUCL, lateral ulnar collateral ligament; MRI, magnetic resonance imaging; Postop, postoperative; Preop, preoperative; PS posterior slice.

One-year Postop MRI scans of a left elbow experiencing work-related pain from the control group. Two consecutive slices (AS and PS) were chosen to reveal the extensor carpi radialis brevis insertional site (short arrow) and lateral ulnar collateral ligament (long arrow). AS, anterior slice; MRI, magnetic resonance imaging; Postop, postoperative; PS posterior slice.

Preop and 1-year Postop MRI scans of a right elbow from the ED group. Two consecutive slices (AS and PS) were chosen to reveal ECRB (short white arrow) and LUCL. AS, anterior slice; ED, ECRB debridement; ERCB, extensor carpi radialis brevis; LUCL, lateral ulnar collateral ligament; MRI, magnetic resonance imaging; Postop, postoperative; Preop, preoperative; PS posterior slice.
Discussion
Consistent with our hypothesis, we made the important finding that the ED technique resulted in slightly better improvements in pain relief during the first 6 months after surgery compared with the classic ECRB origin debridement technique. DASH scores were similar at all time points, and MEPSs showed improved function only at 3 months. Furthermore, postoperative MRI assessments revealed that the ECRB insertional site had increased internal signal intensity on the lateral epicondyle in the control group while there was no covering pathological tissue on the epicondyle in the ED group. There was a significant difference in ECRB tendon signal intensity between groups. In addition, the extended ECRB technique (tenotomy and debridement) resulted in shorter RTW time. All the functional scores were similar at 12 months after surgery.
A previous study by Ertem et al 13 involving 28 patients reported that the mean DASH score decreased from 81.1 ± 17.5 to 34.7 ± 26.8 at 20.5 months after ERCB tendon debridement. Moreover, Baker and Baker 2 reported that the long-term mean pain scores after arthroscopic debridement of lateral epicondylitis were 0 at rest, 1.0 with daily activities, and 1.9 with work or sports (mean follow-up, 130 months). We also observed that both treatment groups showed postsurgical improvements in MEPS, along with decreases in DASH and VAS scores. Together, these findings indicate that arthroscopic removal of pathologic tendinosis tissue is a reliable long-term treatment for recalcitrant lateral epicondylitis.
Kwon et al 19 compared the Nirschl technique (open tenotomy technique) against arthroscopic debridement and found that significant differences remained in postoperative pain scores during hard work after 2 years (VAS, 1.6 ± 1.3 for Nirschl vs 2.2 ± 2.0 for arthroscopy). In the present study, we found that postoperative assessments at 3 months and 6 months indicated higher MEPS and lower VAS score for patients in the ED group versus those in the control group. These findings suggest that the extended ECRB debridement technique resulted in enhanced pain relief in the early postoperative period as well as faster RTW times compared with the traditional debridement technique. Furthermore, Solheim et al 41 found no statistically significant difference in any outcome parameters between arthroscopic tenotomy and debridement at a mean follow-up of 4 years. However, the different result might be due to procedural differences where they released the ECRB tendon from its bony insertion, which might not remove all pathological tissue.
Oki et al 27 found that pain levels (VAS), DASH score, and grip strength continuously improved during the first 3 months after arthroscopic debridement of lateral epicondylitis. Lee et al 22 investigated arthroscopic release treatment of lateral epicondylitis and reported a trend of decreasing differences in VAS score over time: at 3 months (3.27 ± 1.07), 6 months (2.14 ± 1.25), 12 months (1.82 ± 1.10), and 24 months (1.41 ± 1.14). Similarly, Clark et al 7 reported that DASH score decreased from 52.6 ± 2.6 preoperatively to 33.0 ± 3.2 at 3 months, 27.6 ± 3.7 at 6 months, and 23.5 ± 4.1 at 12 months after arthroscopic ECRB release surgery. Here, we also found time-dependent decreases and increases in VAS score and MEPS, respectively, in both the ED and control groups. Our findings were consistent with the studies cited, indicating that the lateral ECRB insertional site after debridement might have a gradual healing process with time.
Owens et al 28 performed arthroscopic release of the ECRB origin and reported that the average return to unrestricted work was 6.0 days (range, 0-28 days). Grewal et al 14 also performed arthroscopic release of the ECRB and reported an average of 18.5 weeks’ RTW period. In their study, patients performing heavy or repetitive work averaged 23.9 weeks before RTW, whereas those performing light work averaged only 6.4 weeks. In the study by Solheim et al, 41 the mean RTW time was 7 weeks after tenotomy and 5 weeks after debridement. The authors suggested that 2 to 4 weeks of recovery may be sufficient for office workers not restricted to continual computer work whereas heavy manual workers usually required 8 to 12 weeks and sometimes more. Our investigation of outcomes also established that the RTW time was reduced in the ED group compared with the control group (8 ± 4 weeks and 18 ± 8 weeks, respectively). The RTW time of the ED group in our study appears similar to that in the reported studies, while the recovery time of the control group was somewhat longer. This was presumably because a longer tissue healing time was required for the control group.
With regard to complications, we found no significant reportable problems associated with either surgical approach used. Using an open technique for lateral elbow tendinopathy, Cusco et al 9 reported that immediate complications included infection (n = 1), seroma (n = 1), cicatricial fibrosis (n = 10), radial neuritis (sensory) (n = 4), and reactive dermatitis (n = 2). Late complications included Frohse arcade syndrome (n = 1) and carpal tunnel syndrome (n = 2). In this study, all operations were performed via arthroscopy, and our experience is consistent with a recent study showing that the complication rates for arthroscopic lateral epicondylitis management are very low (1.1%). 31
Previous studies have identified a number of different risk factors associated with residual microscopic tendinopathy, albeit weak predictors of poor outcome, such as female sex, younger age, long duration of symptoms, as well as smoking. 8,15,40,42,44 Degen et al 10 also indicated that having ≥3 preoperative steroid injections was the most significant risk factor for revision surgery after operative treatment for lateral epicondylitis. Assessment of our cohort found there was no significant correlation between postoperative VAS and other preoperative/intraoperative findings in the control group. Furthermore, MRI scans of 1 patient who still had pain during work showed that the ECRB insertional site had high-intensity signal and possible injury to the LUCL. Shim et al 37 recommended that simultaneous surgical treatment including open debridement and ligament reconstruction provided satisfactory pain relief and functional improvement in patients with LUCL insufficiency.
Limitations
This study has several limitations that must be considered. First, this study did not investigate the clinical outcomes for >2 years. Since longer follow-up times are related to a better outcome, 15 one could question whether outcomes would be influenced with longer follow-up times. However, the main purpose of this study was to investigate clinical outcomes at early time after surgery (3-12 months). Our results indicated that the extended technique produced better elbow function at earlier times with shorter time frames for RTW. Second, some cases with LUCL grade 3 were noted during preoperative MRI assessment; however, during surgery, we did not find problems with the LUCL, and the posterolateral rotatory drawer test under anesthesia proved negative. Therefore, LUCL repair or reconstruction was not performed for these cases. Third, we did not measure wrist extension strength (which theoretically could be weaker with tenotomy in ED group). Finally, the traditional debridement ECRB technique was performed mainly at the beginning of the study period, whereas the ED ECRB technique (tenotomy and debridement) technique was introduced gradually. The assignment of the 2 surgical techniques to patients was not random and not blind but was related to the comparison of 2 periods of the study. We acknowledge that this is a potential selection bias.
Conclusion
Collectively, the extended ECRB debridement technique resulted in enhanced pain relief in the early postoperative period as well as provided faster RTW times compared with the traditional debridement technique. At 1 year follow-up, there were no differences in outcome measures between groups, but residual MRI findings were more common in the traditional debridement group.
Footnotes
Acknowledgment
Final revision submitted January 22, 2022; accepted February 8, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by National Natural Science Foundation of China (No. 81572209), Shanghai Excellent Talents Program (No. 201609), and Shanghai Sports Science and Technology “Comprehensive Plan” Project (18Z004). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Taizhou Hospital (ref. No. K20190802).