
Abstract
Background:
The isometric characteristics of nonanatomic and anatomic posterolateral corner (PLC) reconstruction techniques under weightbearing conditions remain unclear.
Purpose:
To (1) simulate graft elongation patterns during knee flexion for 3 different PLC reconstruction techniques (Larson, Arciero, and LaPrade) and (2) compute the most isometric insertion points of the fibular collateral ligament (FCL) graft strands for each technique and report quantitative radiographic landmarks.
Study Design:
Descriptive laboratory study.
Methods:
The authors performed a 3-dimensional simulation of 10 healthy knees from 0° to 120° of flexion using weightbearing computed tomography (CT) scans. The simulation was used to calculate ligament length changes during knee flexion for the PLC reconstruction techniques of Larson (nonanatomic single-bundle fibular sling reconstruction), Arciero (anatomic reconstruction with additional popliteofibular ligament graft strand), and LaPrade (anatomic reconstruction with popliteofibular ligament graft strand and popliteus tendon graft strand). The most isometric femoral insertion points for the FCL graft strands were computed within a 10-mm radius around the lateral epicondyle (LE), using an automatic string generation algorithm (0 indicating perfect isometry). Radiographic landmarks for the most isometric points were reported.
Results:
Median graft lengthening during knee flexion was similar for the anterior graft strands of all 3 techniques. The posterior graft strands demonstrated significant differences, from lengthening for the Arciero (9.9 mm [range, 6.7 to 15.9 mm]) and LaPrade (10.2 mm [range, 4.1 to 19.7 mm]) techniques to shortening for the Larson technique (−17.1 mm [range, −9.3 to −22.3 mm]; P < .0010). The most isometric point for the FCL graft strands of all techniques was located at a median of 2.2 mm (range, −2.2 to 4.5 mm) posterior and 0.3 mm (range, −1.8 to 3.7 mm) distal to the LE.
Conclusion:
Overconstraint can be avoided by tensioning the posterior graft strands in the Larson technique in extension, and in the Arciero and LaPrade techniques at a minimum of 60° of knee flexion. The most isometric point was located posterodistal to the LE.
Clinical Relevance:
The described isometric behavior of nonanatomic and anatomic PLC reconstruction techniques can guide optimal surgical reconstruction and prevent graft lengthening and overconstraint of the lateral compartment in knee flexion. Repetitive graft lengthening has been found to be associated with graft failure, and overconstraint favors lateral compartment pressure and cartilage degeneration.
The anatomy of the posterolateral corner (PLC) and its clinical relevance has become of high interest in reconstructive knee surgery. 6,19,20 In the context of often combined injuries of the anterior cruciate ligament (ACL), 26 posterior cruciate ligament, 13 and the association with ACL graft failure, 12 the anatomy of the PLC has been described in increasing detail and various surgical techniques have been developed to restore its function. 11,19,29
The PLC consists of three main anatomic structures: the fibular collateral ligament (FCL), the popliteofibular ligament (PFL), and the popliteus tendon (PLT). 4 While the FCL primarily resists varus forces, 13 the PFL has been recognized as an important restraint to varus and external rotation forces 18,28 and the PLT as an additional dynamic stabilizer. 25
Compared with a nonanatomic single-bundle fibular sling reconstruction, as described by Fanelli and Larson 5 (Larson technique), modifications toward a more anatomic reconstruction of the PLC intend to restore the anatomy of the PFL and PLT, as described by Bicos and Arciero 2 (Arciero technique) and LaPrade et al 10 (LaPrade technique). Overall, restoration of rotatory stability has been reported with the use of nonanatomic 9 and anatomic techniques. 21,22,27
LaPrade et al 14 and McCarthy et al 15 highlighted the importance of an additional PFL and PLT reconstruction to fully restore native knee motion and stability. Overall, the influence of the technical variations on functional outcome remains controversial. 6,19,30 Previous studies mainly focused on the biomechanical behavior of these reconstruction techniques, 10,27 whereas the isometric behavior has not been described throughout a full range of motion (ROM) under weightbearing conditions. Concerns remain regarding potential overconstraint and subsequent limitation of external rotation. 15,16,21 As an anisometric graft placement can lead to overconstraint of the lateral compartment, decreased ROM, and even potential graft failure, a detailed understanding of the length changes of the individual graft strands throughout a full ROM under weightbearing conditions would be highly desirable to guide surgical reconstruction.
The primary aim of this study was to analyze the graft elongation patterns of 3 PLC reconstruction techniques (Larson, 5 Arciero, 2 and LaPrade 10 ) during knee flexion. The secondary aim was to compute the most isometric insertion points of the FCL graft strand, around the lateral epicondyle (LE), in a weightbearing 3-dimensional (3D) computed tomography (CT) model and to report radiographic landmarks that allow clear identification of the optimal insertion points. We hypothesized that nonanatomic PLC reconstruction (Larson technique) will demonstrate decreased graft elongation in flexion compared with the Arciero and LaPrade techniques. We also hypothesized that a femoral insertion point can be computed for the FCL graft strand of each technique, in proximity to the LE, that will demonstrate the most isometric characteristics during knee flexion.
Methods
Weightbearing CT data of 10 healthy volunteers, obtained for a previous study, 3 were used for the 3D simulation. The participants had a mean age of 35 years (range, 25-42 years), a mean weight of 83 kg (range, 62-85 kg), and a mean height of 180 cm (range, 169-190 cm). No volunteer reported previous knee pain or surgery. High-resolution CT images were obtained in a standing position with increasing knee flexion (0°, 30°, 60°, and 120°) using an open extremity CT scanner (Verity, Planmed; slice thickness, 0.4 mm). The study protocol was approved by the local ethics committee, and written informed consent was obtained from all patients.
We computed 3D triangular surface models with manual threshold segmentation and region growing using MIMICS software (MIMICS, Materialize, Belgium). The models were imported into the in-house planning software CASPA (Balgrist, Zurich). The femur remained fixed as a reference, and the motion of the tibia was defined relative to the femur during flexion. The femur models of each participant were superimposed using an iterative closest point surface registration algorithm. 1 Five defined knee flexion angles (0°, 30°, 60°, 90°, and 120°) were interpolated to minimize the effect of variable degrees of flexion among individuals during data acquisition. A coordinate system was adjusted according to Grood and Suntay, 8 with the proximal directing vector (z→) being the neutral vector (y→) of the tibia joint plane, the anterior directing vector in direction of the medial border of the tibial tuberosity, and (x→) toward the fibular tip.
Using the 3D simulation, we analyzed the ligament length changes in the Larson, 5 Arciero, 2 and LaPrade 10 PLC reconstruction techniques and determined the most isometric femoral insertion points for the FCL graft strand of each technique.
Definition of the Anatomic Femoral Insertion Points and PLC Reconstruction Techniques
For all 3 techniques, the femoral insertion points of the FCL were defined at the most prominent point of the LE. This simplifying assumption was made because of missing quantitative definitions of the exact femoral FCL insertion around the LE in the Arciero 2 and Larson 5 techniques, and its direct proximity to the LE as described by LaPrade et al. 11 The popliteus insertion was defined at the anterior fifth and proximal half of the popliteus sulcus with approximately 18.5-mm distance to the LE, as quantitatively described by LaPrade et al 11 (Figure 1A). The graft fixation points at the fibula and tibia according to the Larson technique and the Arciero 2 and LaPrade 10 techniques are shown in Figure 1, B and C, respectively. To ensure a safe tunnel trajectory, without violation of the tibiofibular joint, a mean tunnel diameter of 7 mm was simulated at the fibula and 9 mm at the tibia. 23

Definition of femoral, tibial, and fibular, insertion points. (A) Definition of the fibular collateral ligament insertion at the lateral epicondyle (LE) (dark blue circle) and the popliteus insertion (green circle); the shaded circle delineates 18.5-mm distance from the LE. (B) Illustration of the Larson tunnel trajectory (purple rods), the Larson pointant and Larson pointpost (pink spheres in left image), the Arciero tunnel (aqua rod in right image), and Arciero/LaPrade pointant (aqua sphere in right image). (C) The Arciero/LaPrade pointant (aqua sphere in left image) is located 8.2 mm from the most anterior fibular point (yellow circle) and 28.4 mm (indicated by shaded circle) from the fibular styloid tip (dark blue circle). Additional posterior view (right image) demonstrating the LaPrade pointtibia at the popliteal sulcus (dark blue circle), with surrounding shaded circle delineating a tunnel diameter of 9 mm, and the Arciero pointpost (aqua sphere). ant, anterior; post, posterior.
Larson Technique
Larson described an anteroposterior tunnel placement in the fibular head at the location of the greatest anteroposterior diameter. 5 The tunnel was defined with the same directional vector as (y→) at the largest anteroposterior diameter of the fibular head in a strict lateral view. To compensate for the posterior tibial slope, the tunnel was angulated 10° proximally in the sagittal plane. The anterior and posterior tunnel centers were defined at the location of the fibula surface and referred to as the Larson pointant and Larson pointpost, respectively (Figure 1B, pink spheres).
Arciero Technique
The modification of Arciero intended a more anatomic reconstruction of the FCL and an additional PFL graft strand. The described tunnel trajectory is angulated in a posteromedial direction, compared with the Larson technique, to exit close to the PFL insertion at the fibular styloid. 2 To define the Arciero pointant and Arciero pointpost, the trajectory of the Larson tunnel was angulated 20° proximally and 30° medially around its own geometric center (Figure 1B). Its starting point was defined anteriorly to the anatomic FCL insertion (Figure 1C), 28.4 mm from the fibular styloid tip and 8.2 mm from the most anterior fibular point based on quantitative analysis of the posterolateral anatomy 11 (Figure 1C). If a tunnel perforation at the tibiofibular joint occurred, the reference spheres of the fibular styloid tip and the anterior fibular point were scaled equally to define a more distal starting point without tunnel perforation.
LaPrade Technique
The LaPrade technique aimed to reconstruct the FCL, PFL, and the PLT with 2 separate graft strands. 10 The anterior fibular tunnel center was defined as being identical to the Arciero pointant and is described here as the Arciero/LaPrade pointant. In addition, a 9-mm tibial tunnel at the location of the popliteus sulcus, 10 mm distal to the tibial joint plane at the posterior tibia surface, was defined and referred to as the LaPrade pointtibia (Figure 1C).
Definition of Ligament Elongation Patterns and the Most Isometric Points on the Lateral Femoral Surface
Ligament length changes were defined as the maximum length change of a generated ligament during full knee flexion compared with the initial length of the simulated ligament in extension. A string generation algorithm, as described by Graf et al, 7 simulated ligament lengths throughout the full ROM for each graft strand of the Larson, Arciero, and LaPrade techniques (Figure 2). Positive values indicated relative ligament lengthening, and negative values indicated relative ligament shortening during flexion.
The isometry of each graft strand for all surgical techniques was computed from the defined points at the femur to the fibula and tibia within the 0° to 60°, 0° to 90°, and 0° to 120° ROMs. The sum of the relative mean squared errors of all string lengths among the respective ROM defined the isometric score (0 = perfect isometry; the higher the more anisometric). 7
Calculation of the Isometric Score
The isometric score of each string (Is ) was defined as the relative mean squared error of a string (s) over all flexion positions and was calculated using the following equation:

where P is the set of all flexion positions, lp,s is the length of string s in flexion position p, ls is the average length of the string over all flexion positions, and |P| is the number of measured flexion positions. Then, the isometric score of the graft was defined as the average of the isometric scores of all strings. 7
The automatic string generation algorithm according to Graf et al 7 was used to calculate the most isometric points for the FCL graft strands of each technique on the lateral surface of the femur. The femoral points were limited within a sphere (10-mm radius) centered at the LE for the Larson pointant,/post and the Arciero/LaPrade pointant (Figure 2). We aimed to find the femoral points for the FCL graft strands of each technique close to the LE, which demonstrated the most isometric behavior throughout a full ROM. As the posterior graft strands in the Arciero and LaPrade techniques are intended to be taut in flexion to restore varus and rotational stability, we did not attempt to compute the most isometric points for these graft strands because of limited clinical relevance. The location of the most isometric points was reported as the distance (in millimeters) to the LE.
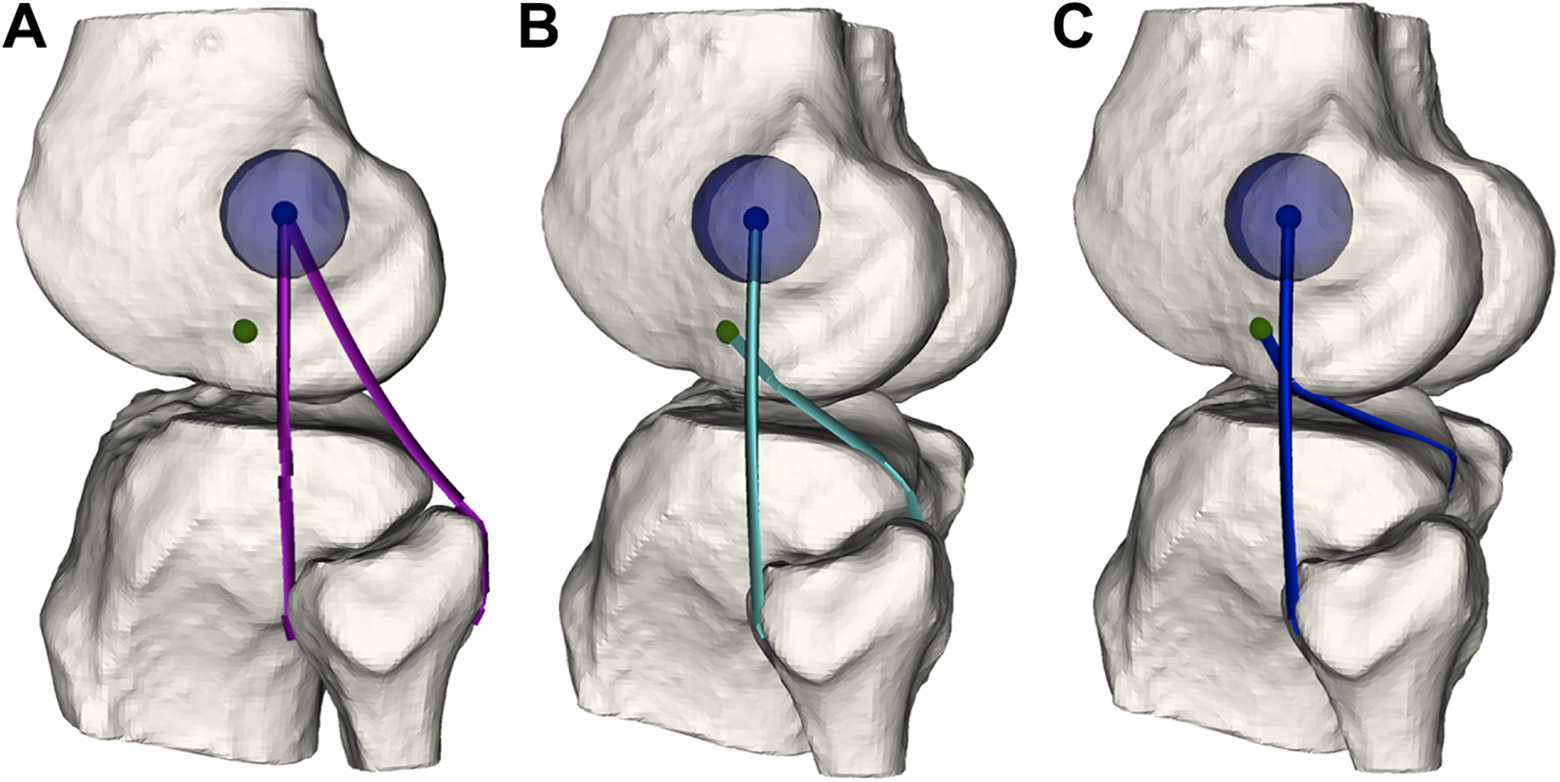
String generation from the defined femoral to the fibular and tibial points defined the anterior and posterior graft strands for the (A) Larson, (B) Arciero, and (C) LaPrade techniques. Definition of femoral insertions of the fibular collateral ligament (FCL) at the lateral epicondyle (LE) (blue circle) and popliteus tendon (green circle). The most isometric point of the FCL graft strand was computed around the LE for each technique (10-mm radius, blue semitransparent circle).
Statistical Analysis
Normal distribution was assessed using the Shapiro-Wilk test and histograms. Medians (ranges) were reported for mainly non-normally distributed data. Differences between ligament length changes of PLC techniques were assessed using the Friedman test and post hoc Dunn-Bonferroni test to correct for multiple testing. The significance was set at < .05. Data were analyzed with SPSS version 23 (SPSS Inc, Chicago, IL, USA).
Results
Ligament Length Changes According to PLC Reconstruction Technique
Lengthening of the ligaments during flexion occurred for all graft strands, except for the Larson pointpost, which shortened during flexion in all individuals. For the anterior graft strands, more lengthening occurred for the Larson technique compared with the techniques of Arciero and LaPrade (P = nonsignificant) during flexion. For the posterior graft strands of Arciero and LaPrade, similar lengthening occurred during flexion, with much of the lengthening starting at 30° of knee flexion (Figure 3 and Table 1).

Ligament length for each posterolateral corner reconstruction technique throughout knee flexion (A: Larson, B: Arciero, C: LaPrade). The solid line depicts anterior graft strand and dotted line depicts posterior graft strand for each technique according to the previously defined points.
Ligament Length Changes for Each Graft Strand Throughout Knee Flexion a
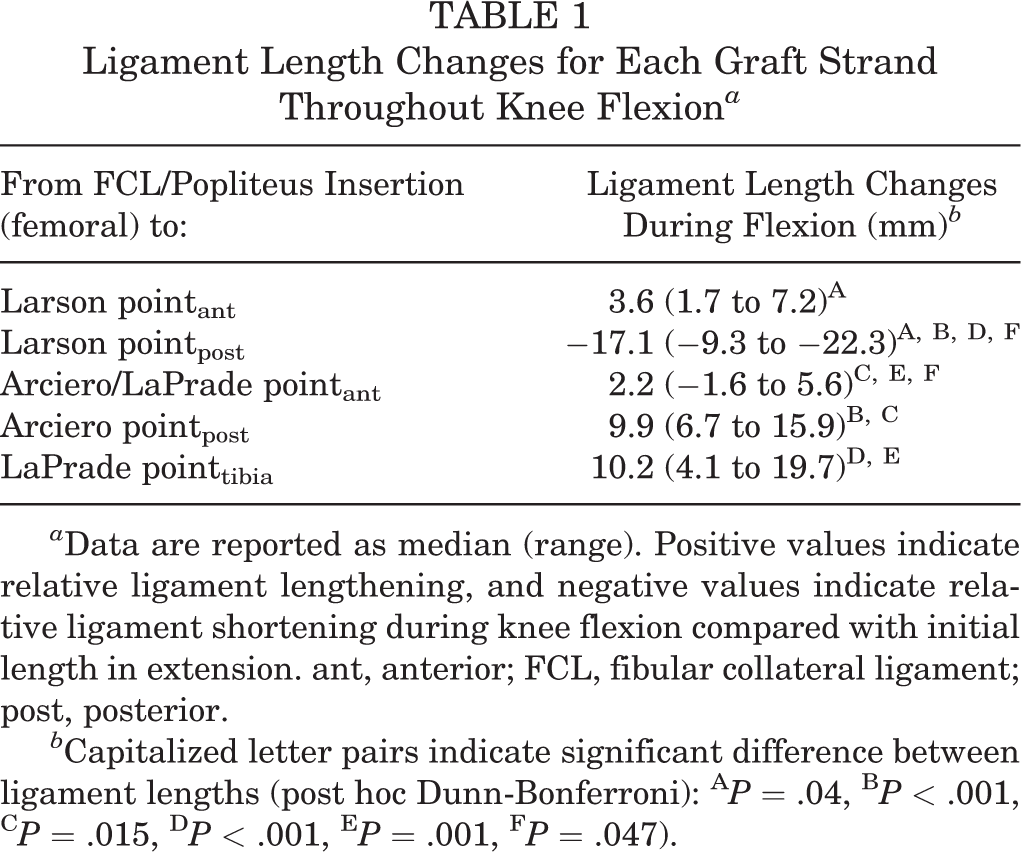
a Data are reported as median (range). Positive values indicate relative ligament lengthening, and negative values indicate relative ligament shortening during knee flexion compared with initial length in extension. ant, anterior; FCL, fibular collateral ligament; post, posterior.
b Capitalized letter pairs indicate significant difference between ligament lengths (post hoc Dunn-Bonferroni): A P = .04, B P < .001, C P = .015, D P < .001, E P = .001, F P = .047).
Isometric Scores and Most Isometric Points According to Technique
The anterior graft strands (Larson pointant and Arciero/LaPrade pointant) showed similar isometric scores in all subgroups of ROM among the 3 techniques. For the posterior graft strands, the Larson pointpost demonstrated superior isometric behavior compared with the Arciero and the LaPrade techniques. The LaPrade pointtibia demonstrated the highest anisometry, but this was statistically not significant compared with the Arciero pointpost. All isometric scores are summarized in Table 2.
Isometric Score According to PLC Reconstruction Technique and Knee Flexion Angle a

a Data are reported as median (range). ant, anterior; FCL, fibular collateral ligament; PLC, posterolateral corner; post, posterior.
The most isometric femoral insertion point was defined for each of the FCL graft strands (Larson pointant and Arciero/LaPrade pointant). The most isometric point of the Larson pointant demonstrated a median ligament lengthening of 2.8 mm (range, −0.6 to 4.1 mm). The most isometric Arciero/LaPrade pointant demonstrated a ligament lengthening of 1.5 mm (range, −2.3 to 3.6 mm) during flexion.
The location of the most isometric points with reference to the LE are summarized in Table 3 and visualized in Figure 4.
Location of the Most Isometric Femoral Points for the FCL Graft Strand of Each PLC Reconstruction Technique With Respect to the LE a

a Values are reported as median (range). Positive values indicate a relative posterior and distal position to the LE, and negative values indicate a relative anterior and proximal position. Bold type indicates the location of the most isometric femoral FCL insertion point (0°-120° of knee flexion). FCL, fibular collateral ligament; LE, lateral epicondyle; PLC, posterolateral corner.

The most isometric femoral point for the fibular collateral ligament (FCL) graft strand of each posterolateral corner reconstruction technique through a full range of motion. The most isometric insertion point was located posterodistal to the lateral epicondyle for all 3 techniques: (A) Larson (pink circle), (B) Arciero (aqua circle), and (C) LaPrade (dark blue circle). The shaded circles depict the mean computed FCL insertion at the lateral epicondyle.
Discussion
The most important finding of our study was that significant lengthening of the posterior graft strands of the Arciero and LaPrade PLC reconstruction techniques could be demonstrated during knee flexion compared with shortening of the posterior graft strand of nonanatomic PLC reconstruction (Larson technique). Overconstraint can be avoided by tensioning the posterior graft strands in the Larson technique in extension, and in the Arciero and LaPrade techniques at a minimum of 60° of knee flexion. For the FCL graft strands of each technique, we were able to define the most isometric point, which prevented ligament length changes greater than 6% during knee flexion in all individuals.
This study analyzed the isometric behavior of nonanatomic and anatomic PLC reconstruction techniques, using full weightbearing 3D CT, which enabled the simulation of the isometric behavior of PLC reconstruction techniques in vivo throughout a full ROM. As controversy persists regarding the optimal technique for PLC reconstructions, we were able to add further evidence to describe the ligament length changes and isometric characteristics for 3 commonly used surgical procedures.
We were able to confirm our primary hypothesis that the nonanatomic technique demonstrated an altered elongation pattern compared with the Arciero and LaPrade techniques for the posterior graft strands. The posterior graft strand for the Larson technique demonstrated shortening in all individuals during flexion, as opposed to substantial lengthening of the posterior graft strands for the Arciero and LaPrade techniques. This is in line with the intended function of the posterior graft strand of the Arciero and LaPrade techniques as a rotational and varus stabilizer in deep flexion, as described previously. 10 To allow an adequate tensioning in flexion without overconstraint, fixation of the posterior graft strand at a minimum of 60° of knee flexion is supported by our data, as the main lengthening occurred between 30° and 60° of knee flexion for the Arciero and LaPrade techniques (see Figure 3, B and C). This finding is of high clinical relevance, as correct tensioning prevents repetitive lengthening and eventual graft failure or slackening in flexion resulting in a biomechanically insufficient reconstruction. In the Larson technique, tensioning of the posterior graft strand should be performed in extension to avoid overconstraint. However, this results in relative slackening of the posterior graft strand in flexion and therefore leads to a potentially insufficient varus and rotational restraint. In contrast, the anterior graft strands of all 3 techniques showed similar isometric behavior throughout the full ROM with only limited graft lengthening.
The second hypothesis, that the most isometric points for the FCL graft strands could be identified, has been confirmed as well. An isometric femoral insertion point, which prevented ligament length changes greater than 6%, could be defined for the anterior graft strands of all techniques, respecting a radius of 10 mm centered at the LE. The posterior strands of the Arciero and LaPrade techniques that intend to reconstruct the function of PFL and PLT do not demonstrate isometry throughout the full ROM because of the nature of their anatomic location, which was confirmed by our study. However, isometry is not the primary goal of the anatomic reconstruction techniques but rather the restoration of posterolateral native knee biomechanics. 27 Nevertheless, based on our results, the most isometric point for the anterior graft strands can be determined and the merits of both techniques can be applied, using an isometric anterior graft strand and an anatomic posterior graft strand. Therefore, we defined quantitative radiographic landmarks, with reference to the LE, which can be reproduced when using intraoperative fluoroscopy.
Regarding the length changes reported, the shortening of the posterior graft strand in the Arciero and LaPrade techniques restores varus and rotational stability in flexion as demonstrated biomechanically in previous studies. 10,27 Sigward et al 24 investigated the isometry of the PLC and found similar results for the FCL graft strand. They found that the most isometric femoral insertion for the FCL graft strand was in direct proximity (<2 mm) to the anatomic insertion, which could be confirmed by our findings. Regarding the PFL and PLT graft strands, Sigward et al 24 found an overconstraint during knee extension and slackening during flexion. This contradicts our findings and previous biomechanical findings that intend a taught PFL and PLT graft strand in flexion and suggested a tensioning in 30° 2 and 60°. 10 The contradicting finding is most likely the result of the chosen definition of the femoral popliteus insertion posterior to the FCL insertion by Sigward et al. 24
Overall, the various technical alterations such as a biceps tenodesis, 17 a sling reconstruction 5 or reconstructions using 2 graft strands 2,10 demonstrated a satisfactory clinical outcome. 6,19,30 This may suggest a sufficient restoration of rotational stability provided by the FCL graft strand alone.
Limitations
Several limitations should be considered. First, the sample size of only 10 participants is relatively small. Second, the defined anatomic landmarks were computed on the 3D models according to described quantitative measurements, and morphometric intraindividual variances may not have been reproduced exactly. However, in clinical reality the exact anatomic insertions may not be identifiable because of scarring, and the reconstruction of the insertion sites relies on radiographic landmarks, which we reported in our study. One needs to keep in mind that the model used included intact cruciate ligaments that are likely to affect the PLC isometry but can often be injured concomitantly in the clinical setting. Furthermore, the use of the described string generation algorithm simplifies the true course of the ligaments, ignoring other soft tissues (eg, the joint capsule and PLT) as well as biomechanical properties, including fiber orientation and graft stiffness.
Conclusion
Significant lengthening of the posterior graft strands of the Arciero and the LaPrade PLC reconstruction techniques occurred compared with shortening of the posterior graft strand of the Larson technique during knee flexion. Overconstraint can be avoided by tensioning the posterior graft strands in the Larson technique in extension, and in the Arciero and LaPrade techniques at a minimum of 60° of knee flexion. The most isometric point for the FCL graft strands of each PLC reconstruction technique was located posterodistal to the LE. The described isometric behavior of nonanatomic and anatomic PLC reconstruction techniques can guide optimal surgical reconstruction and prevent graft lengthening and overconstraint of the lateral compartment in knee flexion. Repetitive graft lengthening has been found to be associated with graft failure, and overconstraint favors lateral compartment pressure and cartilage degeneration.
Footnotes
Final revision submitted December 22, 2021; accepted January 21, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.F.F. has received consulting fees from Medacta SA (Switzerland), Smith & Nephew (United Kingdom), and Karl Storz SE & Co. KG (Germany). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics committee (ref No. KEK-ZH-Nr 2013-074).