
Abstract
Background:
To completely eliminate an infection, the antibiotic concentration must exceed the minimum inhibitory concentration for the causative pathogens. The antibiotic-loaded collagen sponge (ALCS) has been used to manage an infection through a high local concentration of antibiotics.
Purpose:
To evaluate the clinical efficacy of ALCS in the arthroscopic treatment of patients with acute septic arthritis of the native knee.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The authors retrospectively reviewed the data for 132 consecutive patients with acute septic arthritis of the knee who underwent arthroscopic debridement between 2013 and 2019. Patients with a history of surgery in the affected joint, concomitant osteomyelitis, or accompanying medical infection were excluded. The study patients were divided into 2 groups based on the use of ALCS during surgery. C-reactive protein (CRP) levels were temporally measured to normalization and the duration of intravenous antibiotic administration was recorded, and the mean length of hospital stay was compared between the groups. Independent t test and chi-square test were performed to assess differences between the groups, and univariate analysis was used to analyze factors affecting recurrence of septic arthritis.
Results:
Of the 132 patients, 88 were ultimately included in this study; 51 patients were managed without ALCS and 37 were treated with ALCS. There were statistically significant differences between groups in the mean period for CRP-level normalization (15.2 ± 8.2 days [ALCS] vs 26.2 ± 14.7 days [without ALCS]; P = .004), mean duration of intravenous antibiotic use (18.4 ± 7.3 days [ALCS] vs 26.6 ± 16.1 days [without ALCS]; P = .046), and mean length of hospital stay (21.1 ± 11.6 days [ALCS] vs 30.3 ± 18.3 days [without ALCS]; P = .045). The preoperative CRP level was the only significant risk factor for recurrence or treatment failure after single arthroscopic debridement.
Conclusion:
The results of this study indicated that ALCS was able to reduce the duration of CRP-level normalization, intravenous antibiotic use, and hospitalization in patients who underwent arthroscopic irrigation and debridement for acute septic arthritis of the native knee.
The estimated incidence of septic arthritis in the general population is between 2 and 6 cases per 100,000 people per year. 21,28 Septic arthritis of a native joint (ie, without previous surgery or infection) is relatively rare but is still a challenging and important orthopaedic emergency that can lead to irreversible joint damage. 9 The most important factor in determining a patient’s prognosis is rapid diagnosis and treatment. 20 Proper joint drainage, the use of antibiotics, and early joint movement are necessary. 2 Treatment is usually administered for up to 6 weeks, and the first courses of antibiotics are administered intravenously, followed by a switch to oral treatment if an oral option exists and clinical signs, symptoms, and inflammatory markers improve. 9,10,15,16,21,24,25 Tissue penetration of the antibiotic is important in achieving proper local antibiotic concentrations. 8 To completely eliminate the infection, the antibiotic concentration must exceed the minimum inhibitory concentration for the causative pathogens. 14
Antibiotic-loaded collagen sponges (ALCSs) have been used to manage infection by delivering a high local concentration of antibiotics. There are many studies on the use of ALCS for treating osteomyelitis. 1,7,13,18,27 However, to our knowledge, there is no clinical study on using ALCS to treat septic arthritis. Therefore, this study aimed to evaluate the clinical efficacy of ALCS in the arthroscopic treatment of patients with acute septic arthritis of the native knee. We hypothesized that the period of normalization of laboratory values and hospitalization would be reduced in patients who underwent arthroscopic debridement with ALCS for acute septic arthritis in the native knee.
Methods
Study Design
Our institutional review board approved this retrospective study and waived the requirement for informed consent as this was a review of patient data. We retrospectively reviewed our hospital database for consecutive patients with acute septic arthritis of the native knee who underwent arthroscopic irrigation and debridement between January 2013 and January 2019. Arthroscopic treatment is preferentially performed in patients diagnosed with septic arthritis.
The inclusion criteria were as follows: (1) older than 18 years of age, (2) the presence of acute native septic knee arthritis, and (3) undergoing arthroscopic irrigation and debridement. The preoperative diagnosis of septic arthritis was determined by the following criteria: (1) clinical signs including joint swelling, pain, fever, and local heat; (2) enhanced magnetic resonance imaging findings of septic arthritis, such as joint effusion, abscess, synovial thickening, and periarticular soft tissue edema; and (3) aspirated synovial fluid with a white blood cell (WBC) count greater than 50,000 cells/mm3. Patients who met the following criteria were excluded: (1) a history of surgery in the affected joint, (2) coexisting osteomyelitis, and (3) accompanying medical infection (pneumonia, colitis, or cholecystitis).
Any of the following signs or symptoms were considered a recurrence of infection and failure of a single surgical debridement: (1) recurrent clinical manifestations including aggravated pain and fever; (2) rebounding laboratory evidence in the patient’s blood test, including an elevated WBC count and C-reactive protein (CRP) level; and (3) aspirated joint fluid in the patient that is suggestive of recurrent infection with a WBC count greater than 50,000 cells/mm3.
Patients included in the study were classified historically into groups based on the use of ALCS during surgery. ALCS was not used based on the degree of infection and was only used if the patient agreed to an additional fee (equivalent to US$160). CRP levels were temporally measured to normalization, and the duration of intravenous antibiotic administration was recorded. The recurrence rate, CRP normalization period, duration of antibiotic use, and length of hospital stay were compared between 2 groups.
Arthroscopic Debridement
All surgical procedures were performed by 3 experienced arthroscopic surgeons (H.S.J., K.J.K., and E.S.C.) with the patient in a supine position under general or spinal anesthesia. Patients were treated using standard arthroscopy with anteromedial, anterolateral, and superolateral portals. Joint lavage with at least 10 L of saline was performed routinely. Synovectomy was performed in patients with marked synovial hypertrophy and intrasynovial abscesses. 3 ALCS was inserted into the suprapatellar space of the joint through the superolateral portal in the ALCS group (Figure 1). Drains were placed in the notch and lateral gutter and usually removed 7 to 14 days after the surgical procedure, depending on the volume and color of drained fluid. Patients were allowed to bear weight as tolerated with a walker or crutch approximately 2 days after surgery. After removal of drains, active range of motion exercises were started. Quadriceps-strengthening exercises were started 8 weeks after surgery if there was no recurrence of infection.

An antibiotic-loaded collagen sponge (ALCS) is inserted into the joint through the superolateral portal in the ALCS group. (A) The ALCS is folded and inserted into the cannula tip, and the cannula tip is placed in the joint. (B) The ALCS is then inserted into the joint by pushing it through the trocar.
Postoperative Treatment
Weightbearing using a walker or crutch was permitted, as tolerated, approximately 2 days after surgery. After removing the drains, active range of motion exercises were introduced. Quadriceps-strengthening exercises were started 8 weeks after surgery if there was no recurrence of infection.
Antibiotic-Loaded Collagen Sponge
The 5 × 5–cm gentamicin-collagen sponge (Collatamp G; Schering-Plough) used in this study consists of a matrix of purified bovine collagen type 1 impregnated with 2.0 mg/cm2 gentamicin sulfate. The drug is released through a combination of diffusion and enzymatic breakdown of the collagen matrix, providing a high local concentration for at least 72 hours. 26 Collatamp G is approved in South Korea for use in wounds including surgical sites, and there are no restrictions on its intra-articular use. It is mainly used to prevent infection at the surgical site.
Antibiotic Management
Systemic antibiotic therapy was initially performed using a broad-spectrum antibiotic agent after intraoperatively collecting microbiological samples for tissue culture. The antibiotic agents were adjusted in accordance with the results of sensitivity testing. If there was no growth of culture, the use of broad-range antibiotics continued. In general, antibiotics were administered intravenously until the CRP levels and symptoms normalized, and the patient was discharged after switching to oral antibiotics for 4 weeks. If the CRP and symptoms were not normalized, intravenous antibiotics were extended until they normalized, followed by oral antibiotics for 4 weeks.
Statistical Analysis
Differences between study groups were assessed using independent t test for continuous variables and chi-square test with Fisher exact test for binary variables. Univariate analysis was used to analyze the factors affecting recurrence of septic arthritis. Statistical significance was set at P < .05 with 95% CIs. All statistical tests were performed using SPSS for Windows Version 25.0 (IBM).
Results
Of the 132 patients initially reviewed, 110 patients had acute septic arthritis of the native knee and underwent arthroscopic irrigation and debridement. Of these patients, 22 were excluded. Six patients had a history of undergoing surgical procedures on the affected joint, while 2 had a history of septic arthritis in the affected joint. Three patients had osteomyelitis of a bone contiguous with the affected joint, and 4 patients had multiple joint involvement. Seven patients were excluded because of the presence of another medical infection (4 pneumonia, 2 colitis, and 1 cholecystitis). Ultimately, 88 patients were included in the analysis. Overall, 51 patients were managed without ALCS (without-sponge group), and 37 were treated with ALCS (ALCS group).
The mean ages of patients in the ALCS and without-sponge groups were 58.0 ± 17.1 and 62.4 ± 17.3 years, respectively (P = .245). The preoperative durations of symptoms in both groups were 8.7 ± 10.8 and 11.9 ± 21.6 days, respectively (P = .451). The preoperative data of the 2 groups are listed in Table 1. There was no statistically significant difference in the preoperative patient data between the study groups.
Comparison of Preoperative Data Between the Study Groups a

a Data are reported as mean ± SD unless otherwise indicated. ALCS, antibiotic-loaded collagen sponge; CRP, C-reactive protein; WBC, white blood cell.
The postoperative failure rate after single arthroscopic debridement was 27.0% (10/37) in the ALCS group and 27.5% (14/51) in the without-sponge group (odds ratio, 1.022; 95% CI, 0.395-2.645; P = .965). The mean periods of CRP-level normalization were 14.5 ± 7.5 and 24.6 ± 15.2 days in the ALCS group and without-sponge group, respectively, and the CRP normalization period of the ALCS group was significantly shorter than that of the without-sponge group (P = .001). The mean duration of intravenous antibiotic use was 17.9 ± 17.2 days (range, 8-35 days) in the ALCS group and 25.4 ± 6.7 days (range, 5-80 days) in the without-sponge group (P = .017); the mean duration of oral antibiotic use was 27.7 ± 16.7 days (range, 7-73 days) in the ALCS group and 21.2 ± 16.2 days (range, 7-70 days) in the without-sponge group (P = .101). The mean length of hospital stay was 21.1 ± 11.6 days (range, 11-60 days) in the ALCS group and 30.1 ± 19.8 days (range, 7-85 days) in the without-sponge group (P = .025) (Table 2).
Comparison of Postoperative Data Between the Study Groups a

a Data are reported as mean ± SD unless otherwise indicated. Bolded P values indicate a statistically significant difference between groups (P < .05). ALCS, antibiotic-loaded collagen sponge, CRP, C-reactive protein.
We compared the patients with nonrecurrence and recurrence after a single arthroscopic surgery by analyzing the risk factors. The preoperative CRP was the only significant risk factor for recurrence or treatment failure after single arthroscopic debridement (P = .004; Fisher exact test) (Table 3).
Risk Factors for Recurrence or Treatment Failure After Single Arthroscopic Debridement a

a Data are reported as mean ± SD unless otherwise indicated. Bolded P value indicates a statistically significant difference between groups (P < .05). CRP, C-reactive protein; OR, odds ratio; WBC, white blood cell.
b Four cases of methicillin-resistant Staphylococcus aureus, 1 case of methicillin-sensitive Staphylococcus aureus, and 1 case of Candida parapsilosis.
Causative organisms were cultured in 25 patients (28.4%). Methicillin-sensitive Staphylococcus aureus was found in 8 joints, and methicillin-resistant Staphylococcus aureus was found in 7 joints. Other causative organisms included Staphylococcus chromogenes, Streptococcus pneumoniae, Streptococcus agalactiae, Pseudomonas aeruginosa, Escherichia coli, Streptococcus mitis, Candida parapsilosis, and Serratia marcescens (Table 4).
Causative Organisms Detected in Cultures of Joint Fluid a
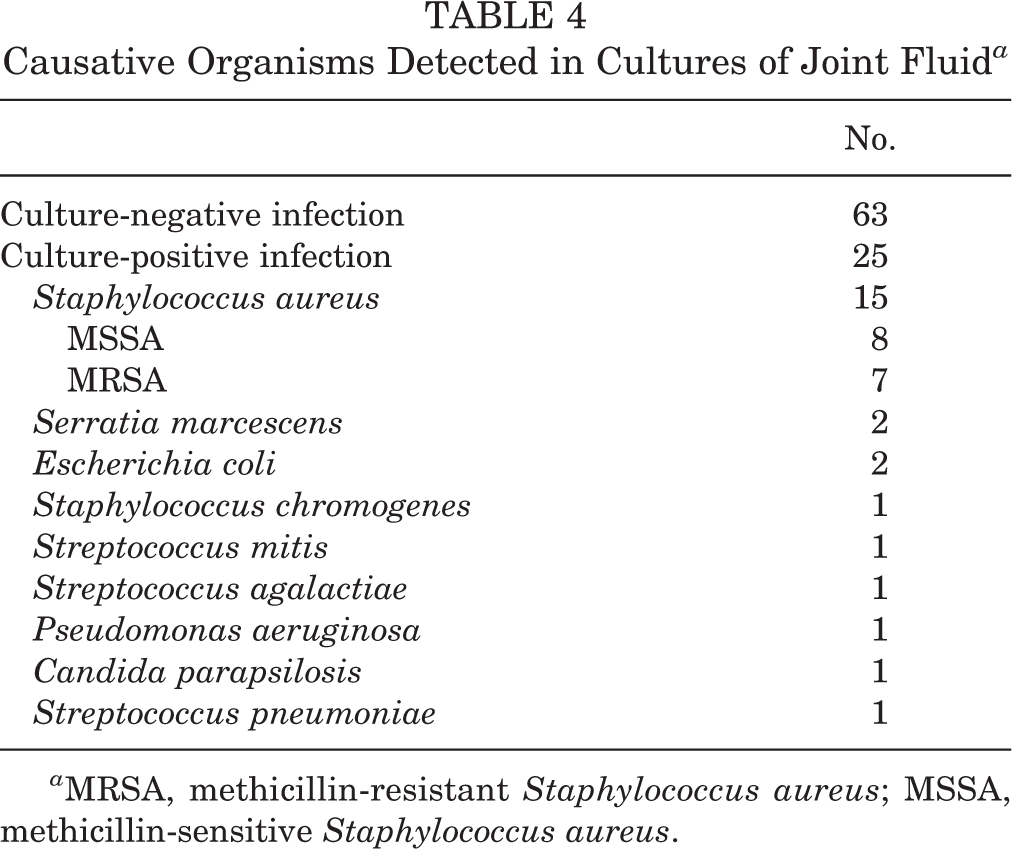
a MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-sensitive Staphylococcus aureus.
Discussion
Our study showed that the use of ALCS was able to reduce the duration of CRP-level normalization (ALCS vs without-sponge groups, 14.5 ± 7.5 vs 24.6 ± 15.2 days; P = .001), intravenous antibiotic use (17.9 ± 17.2 vs 25.4 ± 6.7 days; P = .017), and hospitalization (20.84 ± 11.6 vs 30.1 ± 19.8 days; P = .025). Preoperative CRP was the only significant risk factor of treatment failure after single arthroscopic debridement (with recurrence vs without, 10.3 ± 5.0 vs 6.2 ± 5.2 ng/µL; P = .004).
A considerable number of studies have shown the usefulness of ALCS in diminishing incidences of infectious complications in a wide variety of surgical applications. 5,6,12,19,29 ALCS has been successfully used in reducing wound infection after vascular surgery. 12 Adjuvant therapy with collagenous gentamycin in combination with surgical debridement yielded excellent results in the treatment of deep sternal wound infections. 19 A systematic review of gentamicin-collagen implants reported that ALCS could decrease the rate of surgical-site infection. 5 To our knowledge, there has been no study of arthroscopic surgery with ALCS and no study of the usefulness of ALCS for septic arthritis. In the present study, arthroscopic debridement with ALCS resulted in a shorter period of CRP-level normalization, intravenous antibiotic use, and hospital stay than without ALCS. These results are similar to previous reports in other fields. Zawadzki et al 29 reported that the use of ALCS shortened systemic antibiotic treatment duration and accelerated hospital discharge in cases of craniofacial osteomyelitis and osteitis. De Bruin et al 6 reported that ALCS reduced the length of hospital stay by 40% in patients undergoing gastrointestinal surgery. Shorter use of intravenous antibiotics and hospital stays could be cost-effective and reduce the problems caused by the use of intravenous antibiotics, such as bleeding, thromboembolic events, and line-related infections.
In this study, 72.7% (64/88) of the joint infections were successfully managed with a single debridement. The failure rate of septic arthritis by single arthroscopic debridement was 27.0% in the ALCS group and 27.5% in the without-sponge group. There was no difference between the 2 groups (P = .380). This outcome is similar to the results of other studies that have reported success rates of single debridement ranging from 50% to 87% in various joints. 11,16,17,23 The use of ALCS did not affect the treatment success rate in this study, which is thought to be because of the antibiotic release period of ALCS. In a previous systematic review, pharmacokinetic profiles showed an average local antibiotic concentration that was above the minimum inhibitory concentration for only 5 days. Therefore, it was thought that it might have a positive effect at the beginning of treatment but not on recurrence or treatment failure. The only significant risk factor of the treatment failure was preoperative CRP in this study; however, in several previous studies, preoperative CRP was not the risk factor of the treatment failure. 11,16,17 Further large studies are required to assess the accurate risk factors.
In this study, the most common causative organism for septic arthritis was Staphylococcus aureus, which is similar to the findings of previous studies. 11,17,22 The causative organism was cultured in only 25 cases (28.4%) of patients with septic arthritis identified using synovial fluid analysis and intraoperative findings. This was lower than the 38% to 80% rate reported by the aforementioned studies. The high culture-negative rate is thought to be because of antibiotics already administered in other hospitals or departments.
There may be concern that the insertion of ALCS inside the joint may have a detrimental effect on the inside of the joint. However, the inserted ALCS was not found in 10 patients who underwent arthroscopic reoperation between 2 and 12 weeks after first debridement, and this may indicate that the ALCS had degraded. This finding was similar to that of a previous study that reported degradation of collagen sponge within 2 to 8 weeks, depending on local vascularization. 26
This is, to our knowledge, the first study to evaluate the effect of gentamycin-containing collagen sponge in the arthroscopic treatment for septic arthritis of native joints. Arthroscopic debridement is known to have the same therapeutic effect as open surgery. 4,16 ALCS, which has hitherto been used in open surgery, can be also used in arthroscopy, which can be considered as an option for arthroscopic debridement.
Limitations
The current study has several limitations. First, this is a retrospective study. The allocation to treatment was not random and not powered. Thus, a selection bias may be present in this study. However, consecutive patients were included and strict exclusion criteria were applied to reduce the selection bias. Second, we did not evaluate the clinical outcomes such as functional scores. Third, the preoperative use of antibiotics was performed in 30% of cases, which may have had a negative effect on the culture result. Thus, the culture-negative rate was higher than that seen in other studies. Strain-specific antibiotics were not used in 71.6% of patients, and broad-spectrum antibiotics were used because of negative cultures. However, the failure rate after a single surgery was similar to that seen in other studies. 11,16,17,23 The results of statistical analysis showed that there were no significant differences in the ratio of culture-positive samples between the groups with and without recurrence.
Conclusion
Study findings indicated that the use of ALCS can reduce the duration of CRP level normalization, intravenous antibiotic use, and hospitalization in arthroscopic irrigation and debridement for acute native septic knee arthritis.
Footnotes
Final revision submitted December 13, 2021; accepted January 10, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Chungbuk National University Hospital (reference No. CBNUH 2021-04-024-001).