
Abstract
Background:
There remains no consensus regarding which repair technique provides the most optimal results for unstable distal clavicle fractures.
Purpose:
To compare radiologic and clinical outcomes between locking plate fixation and anatomic coracoclavicular (CC) ligament reconstruction for patients with unstable distal clavicle fractures.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The study included 41 patients with Neer type 2B distal clavicle fracture. In group A (n = 15), patients were treated using CC ligament reconstruction with autologous palmaris longus tendon, artificial tape, and Steinmann pin fixation; in group B (n = 26), patients were treated using anatomic locking plate fixation. All patients had a minimum 2 years of follow-up. CC distance and arthrosis of the acromioclavicular joint were assessed radiographically. Clinical outcomes—including range of motion, visual analog scale for pain, American Shoulder and Elbow Surgeons rating scale, and Constant score—were compared between the groups using the paired Student t test and Fisher exact test.
Results:
Bone union was attained in all patients. In both groups, the CC distance decreased significantly from presurgery to final follow-up: group A, from 16.25 ± 4.75 to 7.66 ± 2.61 mm (P < .001); group B, from 17.3 ± 4.07 to 9.33 ± 2.01 mm (P < .001). The final CC distance was significantly greater in group B (7.66 vs 9.33 mm in groups A and B, respectively; P = .028). Osteoarthritis of the acromioclavicular joint occurred in 13 of 41 patients (3 in group A and 10 in group B). At final follow-up, there was no statistical significance between the groups in range of motion, and clinical outcome scores were satisfactory in both groups, with no statistical difference between them.
Conclusion:
Anatomic locking plate and anatomic reconstruction of the CC ligament showed good clinical results, so both techniques can be considered reliable for restoring stability. However, CC ligament reconstruction had better CC distance on radiologic assessment and did not require removal surgery, so it may be the preferable surgical option to treat unstable distal clavicle fractures (Neer type 2B).
Keywords
Fractures of the clavicle are a common upper extremity injury, and fractures of the distal third of the clavicle account for 10% to 15% of all clavicle fractures. 19,20,28 Fractures of the distal clavicle with injury to the coracoclavicular (CC) ligament are classified as Neer type 2B 22 and are considered unstable fractures; delayed union or nonunion is more common after nonsurgical treatment vs other types of distal clavicle fractures. 5,19,28 Therefore, surgical treatment is more widely accepted to promote solid bone union and good clinical outcomes for this type of fracture classification. 18
For the surgical treatment of unstable Neer type 2B distal clavicle fractures, several techniques have been introduced, such as Steinmann pin (S-pin) or Kirschner wire fixation from acromion to clavicle, tension band wiring, anatomic locking plate fixation, hook plate fixation, CC screw fixation, or reconstruction of the CC ligament. 1,6,9,13,16 Despite various surgical methods, no consensus has been reached regarding which technique provides the most optimal results for unstable distal clavicle fractures. Amid several types of fixation methods, plate fixation is currently widely used, and several studies have reported good clinical results. 1,10,11,33 Recently, the hook plate has been commonly used, and several studies have reported favorable outcomes 14,34 ; however, it has a potential risk of damaging the acromion (by osteolysis or fractures) as well as the acromioclavicular (AC) joint. Because of the shortcomings of the hook plate, we do not prefer to use this technique, and we typically use a distal clavicle anatomic locking plate for these unstable distal clavicular fractures.
As an alternative to plate fixation, anatomic CC ligament reconstruction has been described in recent studies. 4,16,30 This technique is believed to recover the position and integrity of CC ligaments, and CC reconstruction can reinforce internal fixation or be the primary stabilizer of distal clavicle fractures. 3,10 Although solid bone union may overcome the dysfunction of a ruptured CC ligament, successful reconstruction of the CC ligament can improve the clinical result of shoulder function. 18
The purpose of the present study was to compare the clinical and radiologic outcomes of anatomic locking plate fixation vs reconstruction of the CC ligament using an autologous palmaris longus (PL) tendon and Mersilene tape (Ethicon) with S-pin fixation for type 2B distal clavicle fractures. This comparative study was designed on the hypothesis that better clinical results could be expected if fracture union and reconstruction of the ligament were combined, rather than only treatment of the fracture, in unstable distal clavicle fractures.
Methods
Patients
After receiving institutional review board approval, we retrospectively reviewed the data of 41 patients treated for Rockwood Neer type 2B distal clavicle fractures from March 2005 to March 2017. Inclusion criteria were as follows: (1) Neer type 2B fractures confirmed with plain radiographs and computed tomography; (2) acute fractures treated within 2 weeks after injury; (3) magnetic resonance imaging to evaluate injury of the CC ligament and other soft tissue injuries; (4) treatment with CC ligament reconstruction using autologous PL tendon and Mersilene tape (Ethicon) with fixation of S-pins (group A) or anatomic locking plate fixation (3.5-mm anatomical locking plate; DePuy Synthes) (group B); and (5) follow-up≥ 2 years.
Before surgery, computed tomography was used to measure the size of the distal clavicle fragment and the presence of comminution at the fracture site. The criterion for determining the surgical method was the size of the distal clavicle fragment. If the distal fragment was <2 cm in length, CC reconstruction was considered because fixation with our selected plate might not have been feasible.
Surgical Technique
In group A, the PL tendon was harvested from the ipsilateral forearm using a tendon stripper interweaved with Mersilene tape (12 inches in length, 5 mm in width) (Figure 1A). Patients were placed in the beach-chair position under general endotracheal anesthesia. A skin incision approximately 10 cm long was made over the distal clavicle, including the AC joint, and the deltotrapezial fascia was elevated subperiosteally to expose the clavicle, AC joint, and coracoid process. After dissection around the coracoid process, a wire passer was passed under the coracoid process with a 23-gauge rolled wire (Figure 1B). The tip of roll wire was captured by a mosquito forceps, and the wire passer was removed, leaving the roll wire underneath the coracoid process through which to pass the grafting tendon (Figure 1C). The prepared tendon was passed beneath the coracoid process using the roll wire as a guide, and the opposite end of the tendon was passed posteriorly to prevent making a figure-of-8 (Figure 2). The fracture site was reduced and fixed with 2 S-pins (diameter, 2.4 or 2.8 mm) (Figure 1D). The interwoven tendon was tightly sutured with a nonabsorbable suture material. The deltotrapezial fascia was closed securely for additional stability, and the operation wound was closed layer by layer (Figure 3). S-pins were removed 5 weeks postoperatively under local anesthesia in an outpatient office.

(A) Harvested palmaris longus tendon interwoven with Mersilene tape. (B) Rolled wire (23 gauge) prepared with a wire passer. (C) The wire is placed under the coracoid process (black arrow). (D) The fracture site is reduced and fixed with 2 Steinmann pins.

A schematic drawing of coracoclavicular ligament reconstruction.
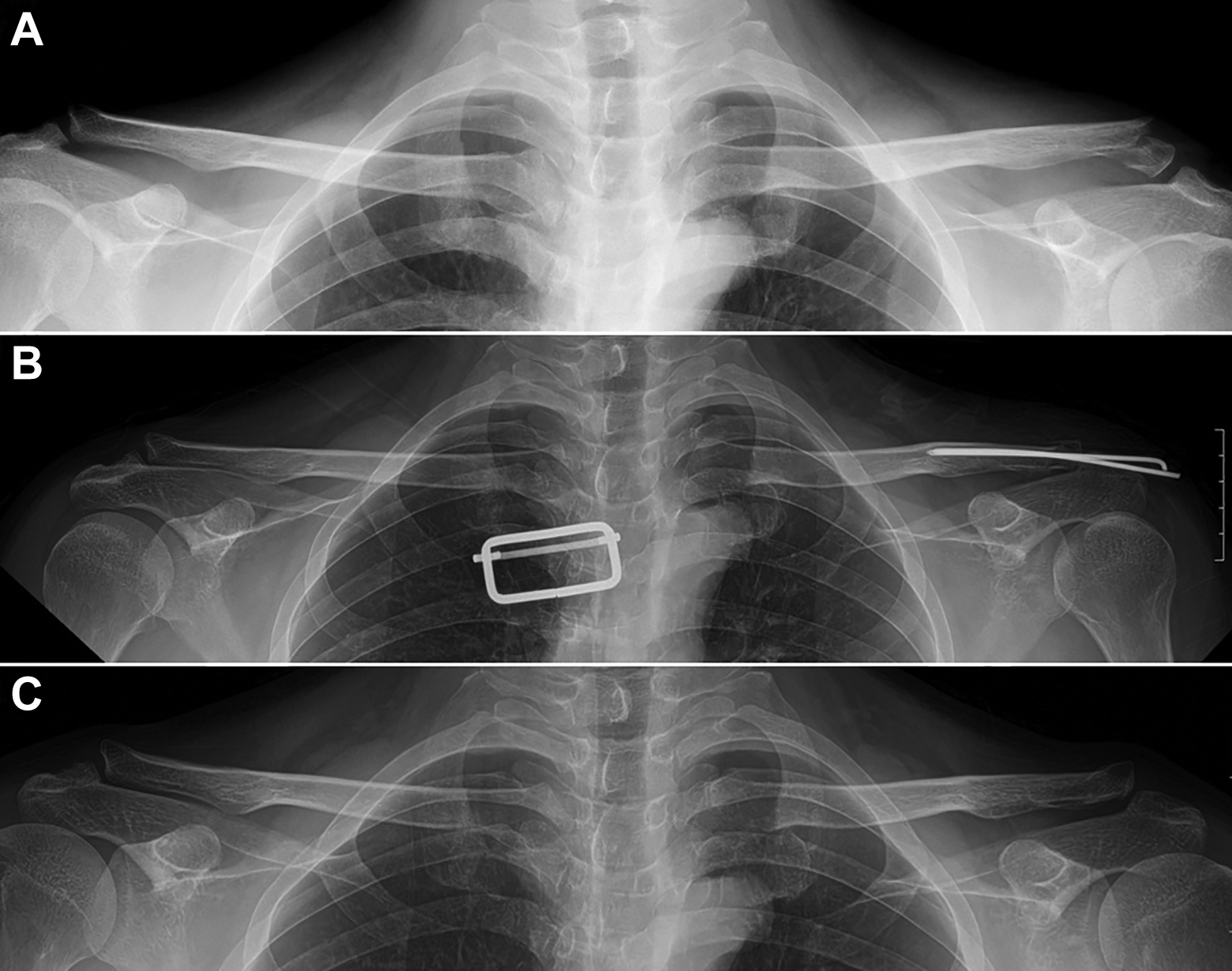
Radiographs of a 40-year-old man with Neer type 2B distal clavicle fracture treated with coracoclavicular (CC) reconstruction. (A) Preoperative radiograph of distal clavicle fractures accompanied with injury of the CC ligament (left shoulder). (B) Postoperative radiograph after anatomic CC reconstruction and Steinmann pin fixation. (C) Final radiograph at 1-year follow-up.
In group B, patients were placed in the beach-chair position under general endotracheal anesthesia, and the same longitudinal skin incision was made over the clavicle and AC joint. After the soft tissue and deltotrapezial fascia were elevated, the fracture site was reduced and fixed with the anatomic locking plate and screws. The AC joint was identified before placing the plate to avoid penetrating it with the screws. One S-pin was inserted from the acromion to the clavicle when additional stability was required, and the operation wound was closed layer by layer (Figure 4). The additional S-pin was removed 4 to 5 weeks postoperatively under local anesthesia in an outpatient office.

Radiographs of a 50-year-old man with type 2B distal clavicle fracture treated using locking plate fixation. (A) Preoperative radiograph of distal clavicle fractures accompanied by injury of the coracoclavicular ligament (right shoulder). (B) Postoperative radiograph after locking plate fixation. (C) Final radiograph at 2-year follow-up.
Postoperative Care
In both groups, the injured arm was immobilized for 5 weeks with a Velpeau brace. Afterward, pendulum exercise and passive stretching exercises of the shoulder joint were allowed. Patients were allowed to start active range-of-motion exercise over the shoulder range and strengthening exercise 9 weeks after the surgery. Return to work and light sports activities were allowed 12 weeks after surgery.
Patient Demographics a
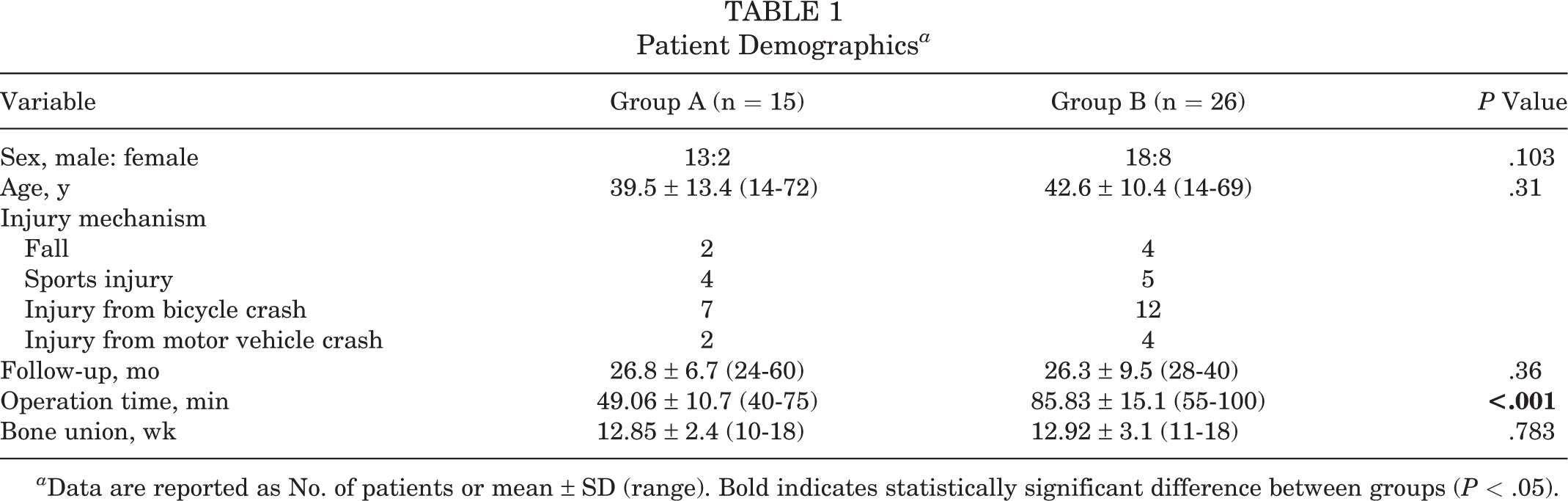
a Data are reported as No. of patients or mean ± SD (range). Bold indicates statistically significant difference between groups (P < .05).
Clinical Assessment
Patients were contacted at least 2 years after the surgery (range, 24-60 months) and scheduled for a clinical examination by the surgeon (Y.M.L.). Using a joint goniometer, an operating surgeon checked the range of motion in the following planes: flexion, abduction, and internal and external rotation at 90° of shoulder abduction and extension. For clinical outcome assessment, the visual analog scale for pain, American Shoulder and Elbow Surgeons (ASES) rating scale, and Constant score were evaluated at final follow-up.
Radiologic Assessment
Radiologic outcomes were evaluated pre- and postoperatively and at final follow-up. The operating surgeon (Y.M.L.) and 1 experienced orthopaedic surgeon (D.J.K.) reviewed the plain clavicle radiograph. The CC distance was assessed in an anteroposterior view of both clavicles as described by Zanca 33 (x-ray beam tilted upward 10°). The CC distance was defined as the distance between the most superior point of the coracoid process and the nearest point of the inferior surface of the clavicle. To reduce measurement errors, radiologic measurements were obtained twice by each author, and average values were used. AC joint arthrosis and bone union were assessed at final follow-up by comparison with preoperative radiographs. Subchondral sclerosis, presence of osteophytes, and reduced joint space of the AC joint were evaluated to diagnose AC joint arthrosis. Bone union was defined as restoration of cortical continuity and progressive loss of fracture lines.
Statistical Analysis
Univariate analysis was performed when data were normally distributed and nonparametric analysis when data were not normally distributed. The paired Student t test and Fisher exact test were used to detect differences in clinical outcomes between presurgery and final follow-up. The Levene test and independent t test were used to detect differences in radiologic outcomes between presurgery and final follow-up. Statistical analysis was performed with PASW software (version 21; SPSS Inc). P values <.05 were considered significant.
Results
Group A consisted of 15 patients (13 men and 2 women) with a mean age of 39.5 ± 13.4 years (range, 14-72 years). The mean follow-up period was 26.8 ± 6.7 months (range, 24-60 months). Group B consisted of 26 patients (18 men and 8 women) with a mean age of 42.6 ± 10.4 years (range, 14-69 years) and a mean follow-up period of 26.3 ± 9.5 months (range, 28-40 months). Osseous union was achieved postoperatively in all patients by 12.85 weeks (range, 10-18 weeks) in group A and 12.92 weeks (range, 11-18 weeks) in group B. The locking plate and screws were removed on average 14 months (range, 8-38 months) after surgery, except for 1 patient who refused additional surgery. All patient, injury, and surgery characteristics were similar between the groups except for operation time, which was significantly longer in group B (P < .001) (Table 1).
The range-of-motion and clinical outcome data at final follow-up are summarized in Table 2. There were no significant differences between groups A and B in range of motion or visual analog scale, ASES rating, and Constant score.
Clinical Outcomes at Final Follow-up a

a Data are presented as mean ± SD (range). ASES, American Shoulder and Elbow Surgeons.
Table 3 compares radiologic outcomes between groups at final follow-up. The mean CC distance in the uninjured shoulder was 7.44 ± 2.26 mm (range, 3-12.92 mm) in group A and 6.76 ± 1.57 mm (range, 4.52-9.81 mm) in group B (P = .53). The mean preoperative CC distance was 16.25 ± 4.75 mm (range, 11.29-29.36 mm) in group A and 17.3 ± 4.07 mm (range, 10.54-24.45 mm) in group B (P = .46). In group A, the mean CC distance decreased significantly to 7.91 ± 3.05 mm (range, 3.79-12.44 mm) on immediate postoperative radiographs (P < .001 vs preoperatively) and 7.66 ± 2.61 mm (range, 4.86-11.78 mm) on the final follow-up radiographs (P < .001 vs preoperatively). No statistically significant differences existed between the immediate postoperative period and final follow-up (P = .734) or between uninjured shoulder and final follow-up (P = .729). In group B, the mean CC distance decreased to 8.79 ± 2.0 mm (range, 6.4-12.84 mm) in immediate postoperative radiographs and 9.33 ± 2.01 mm (range, 5.43-13.11 mm) in the final follow-up radiographs (P < .001). No statistically significant differences existed between the immediate postoperative period and final follow-up (P = .060), but there was a significant difference between the uninjured shoulder and final follow-up (P < .001). Immediately after surgery, the mean CC distance between groups A and B was not significantly different (P = .33); however, at final follow-up, it was significantly greater in group B (9.33 vs 7.66 mm; P = .028).
Radiologic Outcomes at Final Follow-up a

a Data are presented as mean ± SD (range). Bold indicates statistically significant difference between groups (P < .05). CC, coracoclavicular.
b Levene and independent t tests.
Complications related to internal fixation, pin migration occurred in 1 patient in Group A. There were no donor site complications attributed to PL harvest. Two patients in group B showed widening of the AC joint in the final follow-up radiographs, but they did not cite any clinical symptoms of the AC joint (Figure 5). Osteoarthritis of the AC joint occurred in 13 patients: 3 in group A and 10 in group B. When assessing its association with S-pins, osteoarthritis occurred in 9 of 31 patients (29%) with S-pins and 4 of 10 patients (40%) without. Although a higher rate of occurrence of osteoarthritis of the AC joint was seen in patients treated without S-pins, the association was not statistically significant (P = .698). When its association with type of surgical method was assessed, osteoarthritis occurred in 3 of 15 patients (20%) with anatomic CC ligament reconstruction and 10 of 26 patients (38.5%) with locking plate fixation. A higher occurrence rate was seen with the locking plate than with anatomic CC ligament reconstruction, but the association was not statistically significant (P = .305) (Table 4).

Radiograph of the left shoulder of a 50-year-old man treated with anatomic locking plate shows widening of the acromioclavicular joint at final follow-up.
Complications Between the Groups a

a Data are presented as No. (%). Bold indicates statistically significant difference between groups (P < .05). AC, acromioclavicular.
b Protrusion of distal clavicle or foreign body sensation of the implants.
Discussion
Our major findings revealed that patients undergoing CC reconstruction with PL had better outcomes vs the anatomic locking plate. In this study, group A had better radiologic results and a lower final complication rate in AC joint problems (P = .032) and cosmetic complaints (P = .001), but clinical outcomes at final follow-up were similar between the groups. Therefore, both surgical techniques can be relied on for restoring stability and bone union in Neer type 2B distal clavicle fractures.
Neer type 2B distal clavicle fractures are considered unstable because of an accompanying CC ligament injury and have a nonunion rate up to 25% with nonoperative treatment. 18 Although several surgical methods have been reported, consensus regarding the most optimal surgical treatment has not been reached, similar to AC joint dislocations. Plate fixation is a reliable technique for direct osteosynthesis of fractured distal clavicles, and it may restore stability immediately after surgery. 1,17,34 To achieve successful fixation, the distal fragment should be large enough to hold at least 2 or 3 bicortical screws, so distal plate fixation cannot be used in cases of comminuted fracture or fracture with short lateral fragment. 1,34 As an alternative, a hook plate is used in cases where the distal fragment is not big enough to be held by screws, but various complications have been reported, such as subacromial impingement, implant failure, acromial fracture or osteolysis, a higher reoperation rate attributed to hardware removal, and rotator cuff tear. 14,17 With the advent of improved anatomic locking plates, many studies have noted excellent results with fewer complications. 7,8,34 In the present study, we preferred anatomic locking plates over hook plates to avoid the aforementioned plate-related complications. In cases when the distal fragment was too small for fixation, an additional S-pin was inserted and removed 5 weeks postoperatively to prevent complications of the acromion or AC joint.
After bone union is achieved with plate fixation, it is assumed that the CC ligament might heal primarily and restore normal length and tensile strength. However, it is doubtful that fibrous scar tissue healing could lead to normal strength. To overcome this problem, some studies reported more favorable results by performing plate fixation with additional CC augmentation. 3 –5,10,15,24,26,27,31,32 Numerous types of surgical techniques are currently used for CC augmentation, such as screw fixation, 26,31 suture buttons, 4,5,24 synthetic materials, 3,10 and tendon grafts. 15,27,32 Although better clinical outcomes can be achieved using these augmentation techniques, each has its own shortcomings and complications. Bosworth screw fixation was noted to have the disadvantage of limited range of shoulder motion and early postoperative complications, such as loosening or failure of screw fixation. 26,31 Cho et al 4 indicated that CC stabilization using a suture button has some complications, including fixation failure, loss of reduction, loosening of the implant, osteolysis of the acromion, subacromial impingement, AC joint arthritis, and erosion of the coracoid process. Similarly, implant failures were reported with suspensory fixation devices. 5 On this basis, anatomic reconstruction of CC ligament using synthetic materials or tendon grafts was introduced. 3,10,15,27,32 Largo et al 10 stated that locking plate fixation with polydioxanone cord ligament augmentation led to excellent results, with a 95% union rate. Chen et al 3 used Mersilene tape for CC ligament repair and wire fixation for fracture fragments. They achieved satisfactory outcomes and emphasized the advantages of stable fixation, early mobilization, and early return to work.
Tauber et al 25 reported that CC ligament reconstruction using a semitendinosus allograft resulted in significantly better clinical and radiologic outcomes. The mean ASES score improved from 52 to 92 postoperatively, and the mean Constant-Murley score improved from 66.6 to 94.7 postoperatively, reflecting improvement in pain levels and function. 2 Some studies also noted good clinical results in CC ligament reconstruction with an autologous free tendon graft. 23,35 We perform CC ligament reconstruction with autologous PL tendon for AC joint dislocations, the same method used in group A. With S-pin fixation, a fractured clavicle can obtain bone union, whereas, with the reconstruction of the CC ligament, more anatomic soft tissue healing can be achieved. Several techniques use bone tunnels to augment or reconstruct CC ligaments, which sometimes cause fractures or erosions at the clavicle or coracoid process. 2,10,15,27,32 To prevent these complications, our study did not use bone tunnels for graft passage, and 2 S-pins were inserted to maintain stability. No complications occurred, such as loss of reduction or erosion and fractures of the clavicle and coracoid.
A study regarding previous surgical techniques demonstrated that AC joint arthrosis could be the cause of persistent postoperative pain. 21,29 Some authors argue that the AC joint is not a pain generator since concomitant distal clavicle excision does not relieve pain. 2,29 Whichever is true, AC joint arthrosis may result from incomplete reduction of the AC joint, an unstable CC ligament, and hardware-related complications. In this study, AC joint arthrosis occurred in 13 of 41 patients (31%), although no patients complained of clinical symptoms. These results showed no statistical significance between groups, which is likely owing to the small number of patients in this study and may require future research.
We believe that of the numerous surgical options for the treatment of unstable distal clavicle fractures, anatomic CC ligament reconstruction provides an important role in obtaining secure stability and improving clinical and radiologic outcomes. The reconstruction of the CC ligament in distal clavicle fractures with this technique offers a few advantages. First, graft passage without a bone tunnel allows successful fracture union with the recuperation of normal clavicle movements. Normal motion of the clavicle during arm elevation is known to have 2 directions: posterior rotation and elevation. Posterior rotation is the predominant rotation action of the clavicle relative to the thorax, and it is achieved by the actions of muscles that attach to the CC and AC joint ligaments, which exert action on the scapula. 12 Our technique, which spares bone tunnel or screw fixation, allows the graft to be fully tightened over the clavicle, locating it at the isometric point of clavicle motion. Second, this technique is free from complications related to plate fixation, such as stress shielding, refracture by plate, and additional operation for hardware removal. Finally, our study showed that CC distance was better maintained in the CC ligament reconstruction group vs the locking plate fixation group. Yet, the effect of vertical CC distance widening on AC joint arthrosis or long-term clinical outcomes may require study in the future.
In the current study, the groups showed similar clinical results at final follow-up, but cosmetic dissatisfaction attributed to the protrusion of the distal clavicle or foreign body sensation of the implants was significantly higher in patients with locking plate fixation (P < .001). This is not surprising, as the skin and soft tissue over the clavicle are relatively thin, leading to foreign body sensation and bony protrusion of the distal clavicle. Many surgeons do not routinely remove plate and screws because removal surgery can be a burden to the patients. Additionally, some surgeons may think that removal surgery confirms that a complication has occurred. We tend to remove the plate because patients complain of discomfort. In addition, when the plate and screws are removed, the bone receives adequate stress and can restore strength and elasticity, so we think that removing the plate and screws is not always an unnecessary procedure. For these reasons, we concluded that it may be beneficial for patients to undergo removal surgery.
Given that the operation time showed no significant difference between the groups and that no additional surgery is required for our technique, the reconstruction of the CC ligament with autologous PL is a more preferable surgical procedure for type 2B fractures in which the CC ligament is completely ruptured.
Limitations
This study had some limitations, as it is a retrospective design with a relatively small cohort. We also could not figure out the correlations between clinical and radiologic outcomes, such as CC distance widening and AC joint arthrosis, because of the small case numbers. However, under the assumption that better radiologic results are related to better clinical results, further studies are needed to figure out this association. Despite these limitations, we believe that this study clearly shows the advantages of CC ligament reconstruction over classic plate fixation. Several multicenter studies should be carried out in a prospective randomized design in the future.
Conclusion
Locking plating fixation and anatomic CC ligament reconstruction with autologous PL tendon for treatment of Neer type 2B distal clavicle fractures can achieve satisfactory clinical and radiologic outcomes. Although the 2 surgical techniques showed a difference in radiologic results, they do not prove clinical superiority. Because the CC ligament reconstruction technique can simultaneously restore fractured bone and ruptured ligament, it can be regarded as advantageous. Therefore, we recommend this technique as a surgical option to obtain favorable results in unstable distal clavicle fractures.
Footnotes
Final revision submitted November 16, 2021; accepted January 6, 2022.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Yeouido St Mary’s Hospital, The Catholic University of Korea (SC20RISI0078).