
Abstract
Background:
Anterior cruciate ligament (ACL) tears are often associated with other ligamentous injuries. The side-to-side difference in heel height can represent a valuable diagnostic tool in the setting of multiligamentous injuries.
Purpose:
To assess in a cadaveric model how sequential sectioning of the static stabilizing structures of the knee (ACL, fibular collateral ligament [FCL], popliteus tendon [PLT], popliteofibular ligament [PFL], and medial collateral ligament [MCL]) influences heel-height measurements when comparing groups undergoing initial transection of the ACL versus FCL and to assess posterior tibial slope after sequential sectioning.
Study Design:
Controlled laboratory study.
Methods:
A total of 16 fresh cadaveric knees were carefully dissected to expose the ACL, FCL, PLT, PFL, and MCL. Each knee was randomized to either the ACL-first or FCL-first group based on the initial structure sectioned. The sectioning order was as follows: (1) ACL or FCL, (2) FCL or ACL, (3) PLT, (4) PFL, and (5) MCL. Heel height was measured with a standardized superiorly directed 12-N·m force applied to the knee while stabilizing the femur; heel height was also measured with a clinician-applied force. The measurements were compared between and within groups for each sectioned state. The correlation between tibial slope and heel-height measurements was analyzed.
Results:
There were no significant differences in heel-height measurements between the ACL-first and FCL-first groups (P = .863). Combined ACL-FCL injuries led to a 2.85 ± 0.83–cm increase in heel height compared to the intact state. Significant increases in heel height occurred after all sectioned states, except the PFL sectioned state. Combined ACL–posterolateral corner (PLC) injuries resulted in a 3.72 ± 1.02–cm increase in heel height, and additional sectioning of the MCL resulted in a 4.73 ± 1.35–cm increase compared to the intact state. Tibial slope was not correlated with increases in heel height after each sectioning (P = .154).
Conclusion:
Combined ACL-FCL, ACL-PLC, and ACL-PLC-MCL injuries resulted in increasing mean heel-height measurements (2.85, 3.72, and 4.73 cm, respectively) compared to the intact state. Tibial slope was not found to influence increases in heel height.
Clinical Relevance:
The side-to-side difference in heel height may be a clinically relevant examination tool for diagnosing multiligament knee injuries.
A common multiligament knee injury pattern involves the anterior cruciate ligament (ACL) and structures of the posterolateral corner (PLC), 5,14 generally requiring ACL reconstruction with concurrent PLC reconstruction to restore knee stability and function. 16,17 Previous biomechanical studies 12,13 have investigated the relationship between the ACL and PLC, reporting that the fibular collateral ligament (FCL) possesses the most significant effect of forces across the ACL, with FCL sectioning resulting in increased forces across the ACL and medial compartment. As such, injuries to the FCL should be properly identified and treated to avoid increased forces on the ACL graft, which can lead to surgical failure after reconstruction. Similarly, the medial collateral ligament (MCL) warrants a careful examination in multiligament knee injuries, as untreated MCL injuries with valgus instability are associated with up to a 17 times higher risk of ACL graft failure. 1,23 While the integrity of the MCL is typically evaluated through applying valgus stress to the knee, injuries to the MCL may be present on magnetic resonance imaging (MRI) in up to 67% of patients with normal valgus physical examination findings. 25 In an attempt to optimize patient outcomes after ACL reconstruction, a thorough review of physical examination and imaging findings should be performed to identify concomitant PLC or MCL injuries.
Nevertheless, an accurate diagnosis of multiligamentous injuries, primarily in the acute setting, remains difficult. Although MRI is generally performed to aid in the diagnosis of combined injuries to the ACL and FCL, this imaging modality has been reported to possess low sensitivity (48%-57.6%) for the diagnosis of FCL tears. 3 Cinque et al 3 reported on the performance of the heel-height test to improve the recognition of combined injuries by comparing 158 patients with isolated ACL injuries to 117 patients with combined ACL-FCL injuries. When evaluating side-to-side differences in heel height, the authors found a difference of ≥3 cm in 8.2% (13/158) of patients with isolated ACL tears compared to 71.8% (84/117) of patients with combined ACL-FCL injuries. Moreover, the overall specificity in diagnosing combined injuries to the ACL and FCL was 92%, demonstrating the heel-height test to be an effective and inexpensive physical examination tool.
However, other investigations have noted contributions from additional structures in preventing knee hyperextension, namely, the popliteus tendon (PLT) and popliteofibular ligament (PFL), 19 while potential contributions from the MCL have not been evaluated. The purpose of this investigation was to assess how sequential sectioning of the static stabilizing structures of the knee (ACL, FCL, PLT, PFL, and MCL) influences heel-height measurements in a cadaveric model when comparing groups undergoing initial transection of the ACL versus FCL, along with an assessment of posterior tibial slope. The null hypothesis was that although heel-height measurements would increase after sequential sectioning, no significant differences would be appreciated, regardless of sectioning sequence or posterior tibial slope.
Methods
A total of 16 cadaveric knees were tested, including 12 paired knees, from whole-body specimens. All cadaveric specimens had been donated for the purposes of medical research. Paired knees were not tested in all specimens because of the contralateral knees of some specimens meeting exclusion criteria (history of knee injuries or knee surgery, instability on a ligamentous examination before study testing, or the presence of flexion contracture). Specimens were refrigerated until the day of testing and allowed to come to room temperature for at least 4 hours before testing. This study was exempt from ethics committee approval because of the use of deidentified cadaveric specimens.
Specimen Preparation
Before any sectioning, the knees were dissected to expose the ACL, FCL, PLT, PFL, and MCL. The ACL was accessed with a mini-arthrotomy using a medial parapatellar approach; the FCL, PLT, and PFL were accessed with a fascia-splitting posterolateral approach; and the MCL was accessed with a fascia-splitting medial approach. A safety belt was used to secure the distal femur of each cadaveric specimen to a standard dissection table (Figure 1). The belt was positioned just proximal to the superior pole of the patella and fastened in such a manner so as to ensure that no movement of the thigh occurred during testing. K-wire was inserted through the distal aspect of the hallux and attached to a custom jig that allowed for the application of a superiorly directed 12-N·m extension moment with an S-type load cell (Interface) through the use of a pulley system. This load value was chosen based on previous studies comparing clinician-applied and standardized forces on the knee. 10,18

Application of (A) standardized and (B) clinician-applied extension forces. The application of a standardized 12-N·m force was accomplished by securing the distal femur of each cadaveric specimen to a standard dissection table, attaching the distal aspect of the hallux to a custom jig with K-wire, and applying an extension force through a pulley system.
Specimen Testing
Lateral radiographs of each knee were initially obtained to measure posterior tibial slope utilizing previously described methods. 6 Each knee was randomized to 1 of 2 groups based on the initial structure sectioned: ACL or FCL. In the ACL-first group, the sectioning order was as follows: (1) ACL, (2) FCL, (3) PLT, (4) PFL, and (5) MCL. The PLT was sectioned proximal to the PFL. Both the superficial and deep MCLs were sectioned. The FCL-first group followed the same sectioning order, except for the FCL being sectioned first, followed by the ACL. In the intact state and after each sectioning, heel height was measured with a caliper from 0 to 30 cm (with markings to the tenth of a centimeter) with a clinician-applied force 3 and a 12-N·m extension moment (Figure 1). The caliper was placed perpendicular to the table, and the distance between the table and the lowest point of the skin overlying the calcaneus was recorded. The clinician-applied force was performed by the same board-certified orthopaedic surgeon throughout the duration of the study.
Statistical Analysis
Statistical analyses were performed with SPSS software (Version 26; IBM). A 2-way mixed analysis of variance was performed to evaluate the interaction between the sectioned state and order of sectioning on the measured heel height. The within-specimen and between-specimen factors were sectioned state (intact, section 1, section 2, PLT, PFL, and MCL) and order of sectioning (ACL first vs FCL first), respectively. Assumptions of normality and sphericity were evaluated. The Box test for equivalence of covariance matrices demonstrated no violation of heterogeneity of variance-covariance matrices. The Mauchly test of sphericity indicated that the assumption of sphericity had been violated (χ2 = 58.1; P < .001). Because of the violation of the assumption of sphericity, and an epsilon (ε) of 0.352, the Greenhouse-Geisser correction was used to evaluate the interaction. Adjusted post hoc Bonferroni analyses were conducted when significant differences were noted. The level of significance was set at P < .01 based on the total number of comparisons. Correlation analysis of the tibial slope and increase in heel height with each sectioned state was performed by calculating the Spearman correlation coefficient and the 1-tailed P value.
Results
All structures were present in all 16 knees tested. None of the knees had a history of injuries or surgery. All knees were stable on a ligamentous examination before testing. The mean specimen age was 87.7 years (range, 76-103 years), with half of the specimens being female and 56% (9/16) of knees being left-sided.
Increases in Heel Height
In the intact state, the mean heel heights with standardized 12-N·m and clinician-applied forces were 3.95 ± 1.66 cm and 3.51 ± 1.66 cm, respectively. Descriptive statistics of the mean heel height for each group for all sectioned states are displayed in Table 1 and Figure 2.
Heel Height With a Standardized 12-N·m Applied Force for Each Group for Each Sectioned State a

a ACL, anterior cruciate ligament; FCL, fibular collateral ligament; MCL, medial collateral ligament; PFL, popliteofibular ligament; PLT, popliteus tendon.

Heel height with the application of a 12-N·m standardized force by sectioned state for each group (ACL first vs FCL first). Gray shading represents the overlap of 95% CIs between the groups. ACL, anterior cruciate ligament; FCL, fibular collateral ligament; MCL, medial collateral ligament; PFL, popliteofibular ligament; PLT, popliteus tendon.
A 2-way mixed analysis of variance was performed to determine the interaction of the sectioned state and group on heel height. There was a significant main effect of sectioned state on heel height (F(5,70) = 140.17; P < .001). Pairwise comparisons with Bonferroni adjustment indicated a significant increase in heel height after all sectioned states (P < .01), with the exception being the comparison between the PLT and PFL sectioned states (Table 2). The main effect of group was not significant (F(1,14) = 0.031; P = .863). Tibial slope was not associated with the increases in heel height observed after each sectioned state using the standardized applied force (P = .154). Tibial slope measurements ranged from 5.1° to 12.5° (mean, 7.0°). Post hoc analysis of the association between tibial slope and increases in heel height revealed 31.6% power.
Change in Heel Height Between Intact State and Subsequent Sectioned States With a 12-N·m Applied Force a

a Data are reported as mean ± SD (in cm). Bolded P values indicate statistical significance (P < .01). Section change is the change in heel height relative to the intact state (section 1) or prior sectioned state. Total change is the change in heel height relative to the intact state. ACL, anterior cruciate ligament; FCL, fibular collateral ligament; MCL, medial collateral ligament; PFL, popliteofibular ligament; PLT, popliteus tendon.
Standardized (12-N·m) Versus Clinician-Applied Force
In the intact state, the standardized force demonstrated a greater heel height compared to the clinician-applied force (3.95 ± 1.66 vs 3.51 ± 1.66 cm, respectively; P = .017) (Table 3). There were no differences in heel height when comparing standardized and clinician-applied forces for any other sectioned state (Table 3).
Heel Height by Sectioned State Comparing 12-N·m and Clinician-Applied Forces a
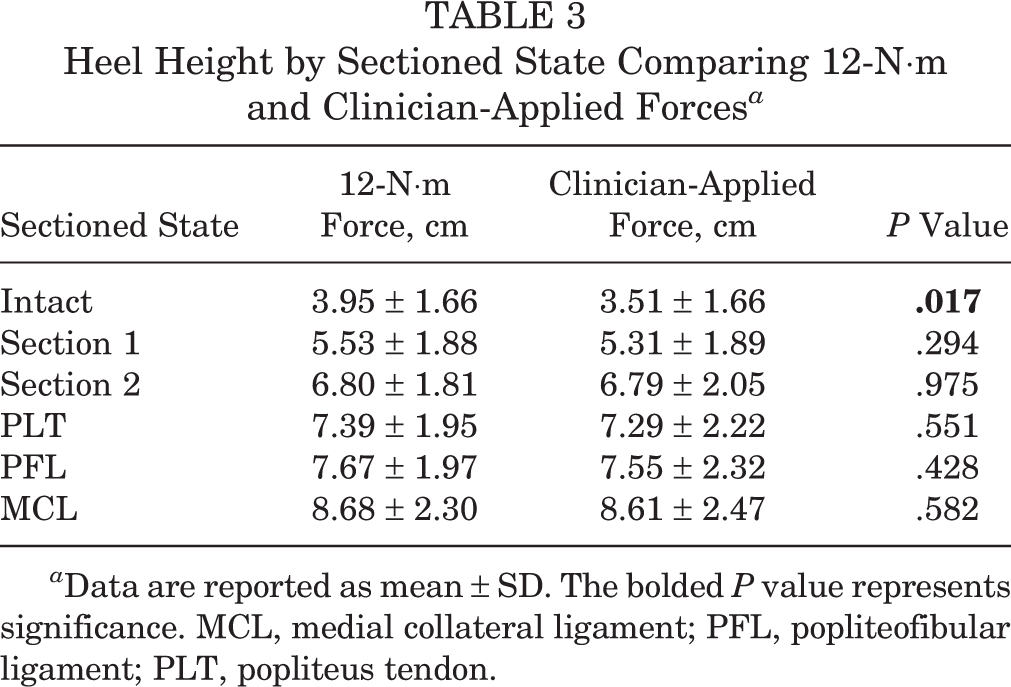
a Data are reported as mean ± SD. The bolded P value represents significance. MCL, medial collateral ligament; PFL, popliteofibular ligament; PLT, popliteus tendon.
Discussion
The main findings from this study were that significant increases in heel height were appreciated with sequential sectioning of the ACL, FCL, PLT, and MCL, regardless of the order of sectioning of the ACL and FCL. PFL sectioning did not significantly increase the heel-height value. Combined ACL-FCL injuries led to a 2.85 ± 0.83–cm increase in heel height compared to the intact state, while combined ACL-PLC injuries led to a 3.72 ± 1.02–cm increase, and combined ACL-PLC-MCL injuries led to a 4.73 ± 1.35–cm increase. Tibial slope was not found to significantly influence heel-height measurements with sequential sectioning.
Because of the low reported sensitivity of MRI in diagnosing FCL tears (48%-57.6%), particularly in chronic injuries because of the lack of edema or acute signs of an injury, multiple clinical and imaging modalities are generally necessary to ensure an accurate diagnosis of combined ACL-FCL injuries. As a result, clinicians should seek to incorporate varus stress radiographs during patient evaluations, which have been reported to demonstrate good interobserver and intraobserver reliability in diagnosing isolated FCL or full PLC tears in addition to a clinical examination and the varus stress test. 7,10 Performance of the heel-height test may therefore serve as a complementary assessment in association with the external rotation recurvatum 11 and dial tests to improve diagnostic accuracy. While the external rotation recurvatum test was originally described to detect PLC injuries, 8 current investigations have demonstrated that combined ACL-PLC injuries are more likely to be recognized with a positive test result. 11 Recognition of combined injuries is critical to ensure prompt referral for a surgical intervention, minimizing the risk for ACL graft failure secondary to unrecognized FCL or PLC injuries and effectively improving clinical outcomes. 9,12,13 Nevertheless, clinicians should be aware that the utility of these diagnostic examinations may be limited in the acute setting because of possible flexion contracture.
In our investigation, sequential sectioning led to increased heel-height measurements, while the mean total heel height was found to increase by 2.85 ± 0.83 cm after transection of both the ACL and FCL compared to the intact state. In their investigation evaluating side-to-side differences in heel height in 158 patients with isolated ACL tears and 117 patients with combined ACL-FCL injuries, Cinque et al 3 reported a cutoff of 2.5 cm (determined through the creation of a receiver operating characteristic curve) to correlate with 72% sensitivity and 92% specificity in identifying combined ACL-FCL injuries, leading the authors to declare such a value as a “positive” heel-height test finding. Meanwhile, a “negative” heel-height test result was found to exclude an associated FCL injury in the presence of an ACL tear with a negative predictive value of 92%. 3 Cinque et al 3 reported that FCL tears were diagnosed preoperatively using clinical and imaging findings and confirmed via examination under anesthesia. De Carlo and Sell 4 previously described normative values of degrees of hyperextension using a goniometer in 578 healthy high school athletes without ligamentous injuries, reporting mean values of 5° in male participants and 6° in female participants. To understand the extent of an injury’s contribution to hyperextension, it is imperative to compare the injured extremity to the extent of hyperextension in the contralateral extremity. Schlegel et al 21 reported that every 1-cm change in heel height corresponds with a 1.2° change in knee extension, lending support to the validity of the heel-height test. Heel height may therefore provide a more objective reporting measure of hyperextension than approximating knee range of motion in degrees. As such, the findings of our investigation provide further support for the use of heel-height measurements to help diagnose combined ligamentous injuries. Per the results of Cinque et al 3 and our investigation, a heel-height increase of at least 2.5 cm will likely allow for adequate identification of combined ACL-FCL injuries. To our knowledge, the impact of the MCL on heel-height measurements has not previously been investigated.
No significant differences in heel-height measurements were appreciated, regardless of the initial ligament transected (ACL vs FCL), for all sectioned states. Morgan et al 19 similarly evaluated the contribution of multiple ligaments (oblique popliteal ligament, fabellofibular ligament, ligament of Wrisberg, ACL, PLC, posterior cruciate ligament [PCL]) in knee hyperextension resistance utilizing 20 fresh-frozen human knees grouped based on initial transection of either the oblique popliteal ligament (group 1; n = 10 knees), ACL (group 2; n = 5 knees), or PCL (group 3; n = 5 knees). The authors reported that the increase in knee hyperextension was greatest after sectioning of the oblique popliteal ligament compared to all other structures, which was not sectioned in our investigation. Morgan et al 19 reported that both the ACL and PLC resulted in increases in hyperextension in all groups tested after sectioning. While the authors reported similar contributions of the ACL and PLC to increases in hyperextension, the contributions of the FCL were not reported. As such, when considering the 2 studies, it is important to note that variations in the contributions of individual structures may be secondary to differences in loading. Namely, Morgan et al 19 re-created hyperextension by applying moments of 14 N·m and 27 N·m to the tibia using loads of 44 N and 88 N at a distance 30.5 cm distal to the joint line. In contrast, Bizot et al 2 utilized 12 pairs of fresh human cadaveric knees, reporting that with progressive forced hyperextension, the posterior capsular structures were noted to fail first, followed by the PLC structures and then the PCL before complete dislocation, with no injury to the ACL or MCL appreciated. While the ACL and FCL appear to contribute to the prevention of knee hyperextension, further studies utilizing standardized methods and extension forces are warranted to better understand the extent of the contributions of the ACL, FCL, PLT, PFL, and oblique popliteal ligament while also determining whether injury to the oblique popliteal ligament occurs in the setting of isolated ACL or combined ACL-PLC injuries.
Tibial slope was not found to be associated with an increase in heel height with each subsequent sectioned state. This is in contrast to Morgan et al, 19 who reported in their investigation of 20 cadaveric knees in which the posterior sagittal tibial slope was measured on lateral knee radiographs (mean, 6.6° [range, 1.1°-12.5°]) that a lower amount of hyperextension was correlated with a higher degree of posterior tibial slope (P < .02; R 2 = 0.35). The authors theorized that patients with higher tibial slopes may be anatomically predisposed to compensate against hyperextension while patients possessing lower posterior tibial slopes may be less able to tolerate injuries to the static extension restraints of the knee. 19 Given that an increased posterior tibial slope (>12°) has been associated with recurrent ACL graft failure, 20,22,24 further investigations are necessary to determine the clinical role of posterior tibial slope in knee hyperextension resistance.
Limitations
This study is not without limitations. The utilization of cadaveric specimens cannot account for the potential voluntary muscle contractions that would be anticipated in live patients undergoing heel-height testing in the clinical setting secondary to discomfort. 3 Testing after ligament transection was performed in only a single plane, and no other test evaluating additional joint behaviors during dynamic joint loading or functional activities was conducted. No side-to-side analysis between limbs undergoing testing versus healthy, contralateral limbs was performed. Not all static restraints to knee hyperextension were accounted for in our model. Namely, as reported by Morgan et al, 19 sectioning and analysis of the oblique popliteal ligament were not performed. In addition, although all specimens were secured to the testing table with a safety belt, we were unable to account for any contribution of the soft tissue envelope to the amount of fixation that was applied. The heights and weights of the included specimens were not recorded, prohibiting the ability to evaluate the relationship between body mass index and heel-height increases. Throughout testing, the contribution of soft tissue hysteresis may have affected measurements between specimens, as no cyclic preconditioning was performed. Furthermore, no reliability test evaluating our fixation method was performed. In the assessment of the relationship between tibial slope and changes in heel-height measurements, our analysis was underpowered at 31.6% power. However, it is unlikely that tibial slope impacted the increases observed in heel height for each specimen because of the tibial slopes of all included specimens being within normal range (5.1°-12.5°). Lastly, further investigations analyzing the effect of leg length and tibial length as they relate to knee hyperextension are needed to better understand the variability in measurements and further validate the use of heel-height measurements in diagnosing combined injuries in the knee. 15
Conclusion
Combined ACL-FCL, ACL-PLC, and ACL-PLC-MCL injuries resulted in increasing heel-height measurements compared to the intact state (mean of 2.85, 3.72, and 4.73 cm, respectively), regardless of sectioning order of the ACL and FCL. Tibial slope was not found to significantly influence increases in heel height with sequential sectioning.
Footnotes
Final revision submitted December 17, 2021; accepted January 10, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.M.K. has received grant support from Arthrex and education payments from Medwest and Smith & Nephew. N.N.V. has received consulting fees from Arthrex, Medacta, Smith & Nephew, and Stryker; speaking fees from Arthrex; royalties from Smith & Nephew; and hospitality payments from Relievant Medsystems. R.F.L. has received education payments from Arthrex, consulting fees from Arthrex and Smith & Nephew, speaking fees from Smith & Nephew, and royalties from Arthrex and Smith & Nephew. J.C. has received education payments from Arthrex and Smith & Nephew; consulting fees from Arthrex, DePuy, Linvatec, and Smith & Nephew; speaking fees from Linvatec; and hospitality payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.