
Abstract
Background:
Femoroacetabular impingement (FAI) is an increasingly recognized cause of hip pain in young athletes. Although there are multiple studies that describe the radiographic prevalence of FAI in athletes, its true incidence within this population is unknown.
Purpose:
To report on the overall and sport-specific incidence of symptomatic FAI in National Collegiate Athletic Association (NCAA) Division I athletes. Return-to-sport times were reported for patients treated operatively.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective review was conducted to identify all reported hip injuries within a large, multisport NCAA Division I institution. Hip injuries were stratified into FAI, general pain/dysfunction, musculotendinous, ligament, bursitis, bone stress, contusion, and other. FAI was diagnosed based on history, physical examinations, imaging, and symptomatic relief after a diagnostic injection. Descriptive statistics were used to calculate the overall and sport-specific incidence, and chi-square analysis was performed to identify contingency data.
Results:
In a 3-year period, a total of 5319 musculoskeletal injuries occurred in 1072 athletes. There were 491 (9.2%) hip injuries that occurred in 288 athletes, of which 40 injuries were FAI. The overall incidence of symptomatic FAI was 3.0% of the total population, 3.7% of all injured athletes, and 13.9% of athletic hip injuries. There were no statistically significant differences in FAI rates among male and female athletes overall or among male and female athletes within similar sports. Of the 19 athletes who were treated nonoperatively, 2 failed to return to play: 1 secondary to multiple musculoskeletal injuries and 1 related to cardiac issues. There were 21 hips in 20 patients that were treated operatively, with 1 athlete failing to return to sport. Return to play occurred at a mean of 202 days (range, 81-360 days) after hip arthroscopic surgery.
Conclusion:
In this large, multisport NCAA Division I cohort, the overall incidence of symptomatic FAI was 3.0% and represented 13.9% of hip injuries. The successful management of FAI with return to play was achieved by both nonoperative and operative treatment methods. The relatively low incidence of symptomatic FAI, despite reports of a high prevalence of FAI morphology in athletes, serves to emphasize the importance of clinical evaluations in treating patients with FAI.
Hip and groin injuries account for 3% to 6% of injuries in young athletes. 9 Over the past decade, femoroacetabular impingement (FAI) has emerged as a well-recognized cause of nonarthritic young adult hip pain. 10,22 FAI results from dynamic bone and soft tissue impingement secondary to femoral head-neck junction abnormalities (cam type) and/or acetabular overcoverage (pincer type), which can lead to damage to hip articular cartilage and/or the acetabular labrum. 24 The management of these injuries continues to evolve, with the literature demonstrating a global increase in arthroscopic treatment. 1 Outcomes from arthroscopic treatment have been promising, with studies reporting high levels of patient satisfaction and return to sporting activities. 23,25
There has recently been an increase in published studies describing the epidemiology and, by proxy, the cause of FAI. 3,4,8,12,19,21,22 Early sport participation has been implicated as a risk factor for the development of cam FAI, as morphological changes may occur to the developing femoral head physis. 4 As such, there are an increasing number of studies that have investigated the radiographic prevalence of these bony abnormalities in athletes among a variety of sports. 6,8,14,16,20,27,30 Many of these studies, however, have focused on radiographic prevalence within asymptomatic patients. Similarly, there are general population studies that have described the overall prevalence of FAI morphology in the asymptomatic population. 11 Others have focused on the overall incidence of hip and groin injuries based on athletic exposures. 9,17,22 There is, however, a paucity of reports that have described the incidence of symptomatic FAI within the athletic population. Moreover, few reports have attempted to determine the rate of symptomatic FAI based on factors such as sport participation and sex.
Therefore, the purpose of this study was to report on both the overall and sport-specific incidence of symptomatic FAI in a large, multisport National Collegiate Athletic Association (NCAA) Division I institution. The ability to return to sport was recorded for all patients, and the time to return was recorded for patients treated operatively. Our hypothesis was that the return-to-sport rate would be high in both nonoperatively and operatively treated athletes with symptomatic FAI.
Methods
A retrospective review of electronic medical records over a 3-year period with athletes having a minimum 1-year follow-up was performed. The medical records of all athletes who sustained a musculoskeletal sport-related injury were reviewed. Patients were identified for further chart review if they sustained a hip injury during sport participation within the study period. Data were then obtained to include sex, sport played when injured, treatment performed, and outcome. The diagnosis of FAI was confirmed by history and physical examinations by an orthopaedic surgeon (M.S.), consistent bony morphology of FAI on plain radiography, and in most cases, magnetic resonance arthrography that included an intra-articular injection of anesthetic with more than 50% relief of pain.
Study Definitions
Hip Injury
For the purposes of this study, a hip injury was defined as one that (1) was located in the hip joint, pelvis, groin, thigh, and/or buttock; (2) occurred during an organized practice or competition throughout the academic year (traditional and nontraditional seasons); and (3) received medical attention from a certified athletic trainer or team physician.
Missed Time
For the purposes of this investigation, missed time was defined as the number of calendar days that an injured athlete was not allowed to participate in any organized practice or competition within his or her respective sport. Missed time included the number of calendar days between the incident date and the calendar day on which the athlete was medically cleared to return to play at a level that allowed practice participation in his or her sport. 5
Similar Sports
For the purposes of this investigation, similar sports implied intercollegiate sponsored sports that have both male and female teams and have similar demands. The following sports were considered similar sports during this study: basketball, diving, fencing, rowing, soccer, swimming, tennis, volleyball, and water polo. As the result of different events and demands, gymnastics and baseball/softball were not considered sex-similar sports.
Data Collection
Data were collected from March 2009 to August 2013. Data were gathered from the InjuryZone database (Presagia Sports) and electronic medical records. We queried all musculoskeletal injuries that occurred in athletes during the study period. We then identified all hip injuries, as outlined above, and stratified them into the following categories: FAI, general pain/dysfunction, musculotendinous, ligament, bursitis, bone stress, contusion, and other. Nonspecific dysfunction included the diagnoses of tightness, irritation, and spasm. Individual participation on a sports team was utilized, and one athlete could only participate on one team during the study.
Statistical Analysis
Excel 2010 (Microsoft) was used to analyze the raw data collected in this investigation. Variables included for analysis in this study were sex, sport, hip involved, date of presentation, date on which symptoms began, treatment, date of follow-up, days of sport missed, return-to-sport date, and diagnosis. For those who received cortisone injection(s), the number received, timing, and response were noted. For those undergoing surgical treatment, we analyzed the time from symptoms to surgery, surgical treatment performed, and need for microfracture. Descriptive statistics were used, with the incidence for each respective sport determined. Where applicable, the chi-square test was performed for contingency data.
Results
Among the 1332 student-athletes observed in this study, 1072 athletes (478 female and 594 male) sustained a total of 5319 musculoskeletal injuries (2121 female and 3198 male). Overall, 491 (9.2%) hip injuries occurred in 288 student-athletes (131 female and 157 male) (Figure 1). Among the 288 athletes who sustained a hip injury, 40 athletes were diagnosed with FAI, representing an incidence of symptomatic FAI in 3.0% of all athletes, 3.7% of injured athletes, and 13.9% of athletes who had hip injuries observed in the study period. FAI represented 8.1% of all hip diagnoses observed during the study period. FAI occurred in 21 female and 19 male patients. There was no statistically significant difference between the rates of FAI among male and female athletes by chi-square analysis. Moreover, no statistically significant differences were detected between male and female athletes participating in similar sports.
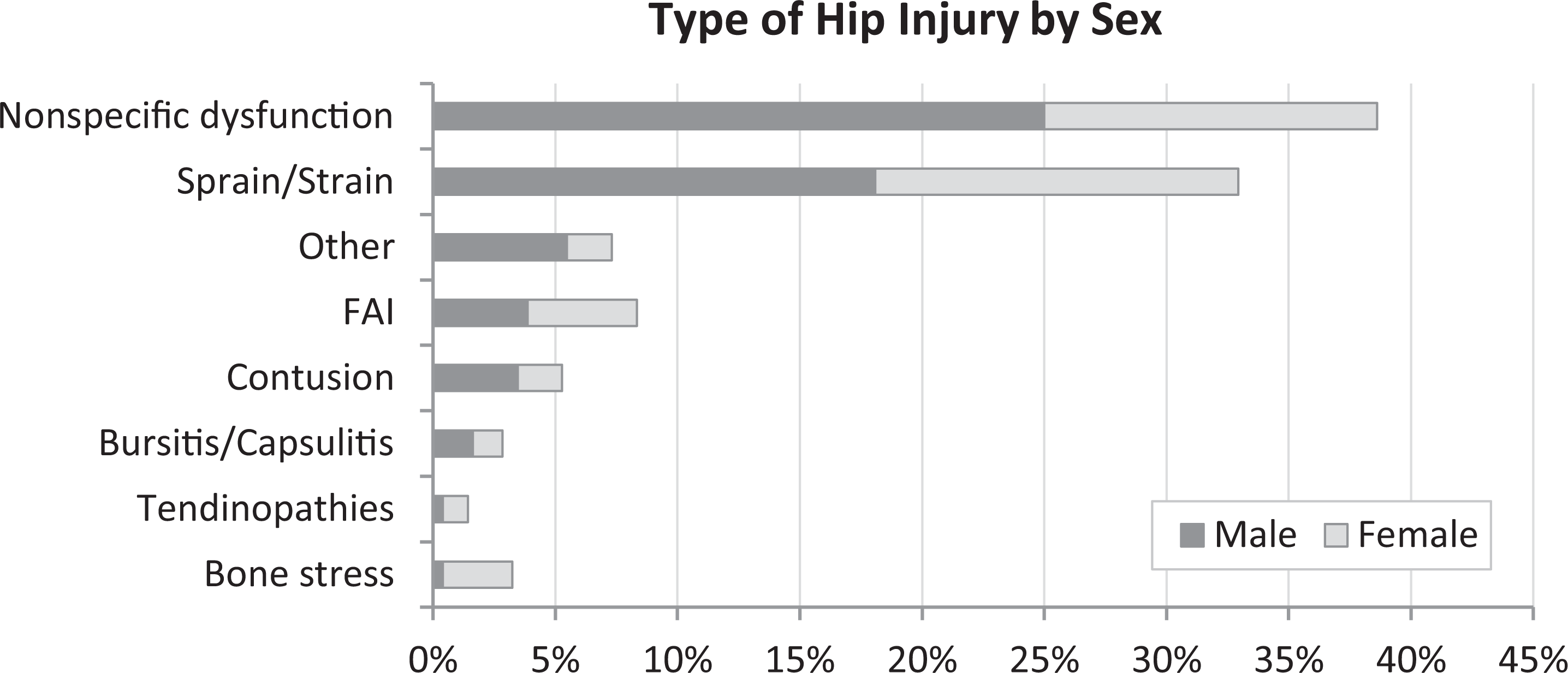
Proportion of male and female athletes by type of hip injury (n = 491). Nonspecific dysfunction included tightness, irritation, and spasm. “Other” included neuropathy, hernia, general inflammation, and pain.
FAI and Sport
Participation in each sport was evaluated to determine the percentage of each team’s athletes who were affected by FAI (Figure 2). For this calculation, each athlete was only counted one time during the study period. Among the 40 patients who were diagnosed with FAI, 24 injuries (15 male and 9 female) occurred in similar sports, but this difference failed to reach statistical significance. Symptomatic FAI was diagnosed among 21 sport teams, with men’s basketball representing the greatest number (n = 7) and percentage (33.3%). At least 5% of the team’s athletes in 8 sports were affected by FAI.
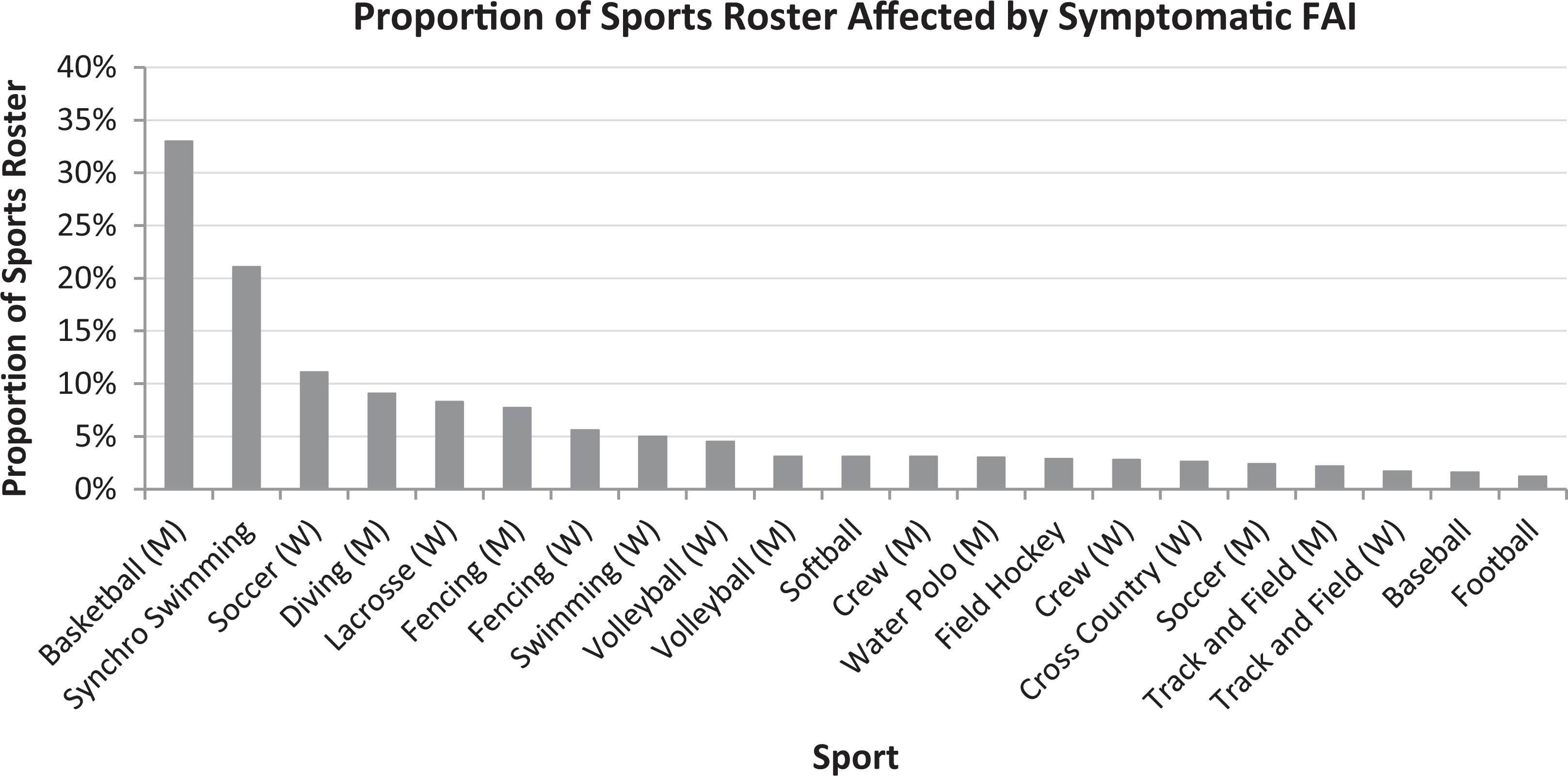
Proportion of athletes affected by femoroacetabular impingement by team sport. The sport roster includes the total number of athletes over the study period. M, men’s; W, women’s.
Nonoperative Management of FAI
All athletes were initially treated nonoperatively, and this was the only treatment method in 19 of 40 athletes after their diagnosis of FAI. Nonoperative management consisted of formal physical therapy for stability and therapeutic exercise interventions as well as transient activity modification during episodes of increased symptoms. In addition to formal physical therapy and activity modification, 27% of athletes treated nonoperatively received an image-guided corticosteroid injection. Injections were utilized if symptoms persisted for approximately 10 weeks after the diagnosis and patients failed physical therapy and activity modification. Those who did not receive injections played with discomfort, played with modification, and/or received nonsteroidal anti-inflammatory drugs. We cannot comment specifically on whether they were asymptomatic or able to play with their symptoms. All 19 athletes treated only nonoperatively underwent a physician follow-up within a mean of 13 months (range, 4-23 months) after their respective diagnosis date. There were no athletes observed who were treated nonoperatively for their hip pain (associated with FAI and/or labral abnormality) and missed any time away from their respective sport. At the time of final follow-up, none had undergone surgical treatment. There were 2 athletes who retired from sports: one related to cardiac issues and one related to multiple injuries, including his hip, shoulder, and ankle. The remaining 17 of the 19 patients (89.5%) treated nonoperatively were able to return to their previous level of sport. As such, nonoperative treatment only resulted in a successful return-to-sport rate of 42.5% (17/40) after a diagnosis of FAI.
Operative Management of FAI
A total of 21 hips in 20 patients (10 female and 10 male) failed nonoperative treatment and underwent a surgical intervention with hip arthroscopic surgery for persistent symptoms related to FAI. The mean time from symptoms to surgery was 255 days (range, 25-495 days). We found that 71% of those who underwent a surgical intervention waited longer than 6 months before proceeding with a surgical intervention. There were 7 (33.3%) hips that received at least one steroid injection before the surgical intervention. Surgery consisted of acetabuloplasty alone in 19% of hips, cam resection/femoral osteoplasty alone in 24% of hips, and combined femoral and acetabular osteoplasty in 57% of hips. Microfracture was performed in 5 cases (23.8%). The mean time from injury to surgery was 267 days (range, 85-463 days) for patients who required microfracture compared with 264 days (range, 25-495 days) for those who did not require microfracture. Of the cases that involved pincer-only management, 75% of those patients were female. They demonstrated a mean chondral defect distance from the rim of 2.8 mm (range, 2-4 mm), and none required microfracture. Mixed-type impingement occurred in 3 times as many male patients as female patients. A total of 4205 days of sports participation were lost after an arthroscopic intervention, averaging 202 days to recovery (range, 81-360 days). The overall return-to-sport rate was 95.2% (20/21). One athlete, a female synchronized swimmer, returned to running, swimming, hiking, and bouldering but did not return to synchronized swimming because of issues unrelated to her hip. A male athlete who underwent bilateral surgery did not return to his initial sport of crew but did return to playing rugby.
Discussion
In this large, multisport cohort of NCAA Division I athletes, the overall incidence of symptomatic FAI was 3.0% of all observed athletes and represented 13.9% of hip-injured athletes. This rate is higher than what has been presented in prior large epidemiology studies, which have reported 1.4% of hip injuries in collegiate athletes. 9 Moreover, another large NCAA database study did not specify FAI but identified 1 labral tear in an injury population of 1618 football players. 17 This large cohort study serves as one of the first studies to identify the true incidence of symptomatic FAI among a mixed elite-level athletic population.
Multiple studies have reported on the radiographic prevalence of FAI and have implicated sport participation in its development. ¶ Siebenrock et al 26 investigated 72 hips in basketball players with age-matched controls who did not participate in sports. They found that basketball players had a higher prevalence of cam deformity, with 89% of athletes having an alpha angle of >55° versus 9% of nonathlete controls. Larson and colleagues 14 identified radiographic evidence of FAI in 90% of collegiate football players undergoing an evaluation before the National Football League (NFL) Draft. Similarly, Nepple et al 20 identified radiographic evidence of FAI in 94.3% of hips evaluated in football players at the NFL Combine. Looking at aquatic athletes, Langner et al 13 utilized magnetic resonance imaging and identified cam morphology in 67.5%, pincer morphology in 22.5%, and labral tears in >50% of patients studied, despite only 15% of the patients seeking treatment for hip pain. Still, others have identified radiographic markers of FAI to be present in 9% to 50% of the asymptomatic population. 8,9,11,17,28 Many of these studies, however, report the prevalence of FAI radiographic markers but are unable to comment on the incidence of symptomatic FAI within the population.
In this study, we were able to identify the incidence of symptomatic FAI within our study population. A large, multisport NCAA Division I cohort is an ideal population to evaluate the incidence of FAI within the sport population. First, it represents a class of elite, young adult athletes with a high likelihood of early exposure to sports who are unlikely to have underlying arthritis. Second, nearly all sport injuries are initially treated and recorded within our health record system, functioning as a contained population. Finally, given the variety of sports, it allows the opportunity to risk-stratify across different sporting activities as well as allow for comparisons between male and female athletes participating within similar sports.
In the current study, the men’s basketball team, with 33.3%, was identified as having the largest percentage of symptomatic FAI for a team within our study cohort. In contrast, we only found 2 football players who developed symptomatic FAI during the study period. This finding could be caused by the relative rest afforded by once-a-week play in football or, similar to other injuries, failure to seek treatment because of the ability to compensate. It is also possible that the higher incidence in our Division I basketball players is related to accelerated adolescent growth, coupled with increased overloading from early athletic activities in these typically taller athletes. Another speculative possibility is that during this time period, the basketball coach placed a strong emphasis on defense, and players were frequently in a “defensive slide” position, placing the hip in flexion and external rotation with side-to-side movements. Additionally, the strength coaches could have put an emphasis on deep squats, deadlifts, and exercises with lunges. This may have produced symptoms that otherwise would have remained dormant, even in the setting of FAI morphology.
While we are unable to specifically account for the stark differences between the reported radiographic prevalence within the literature and the incidence in our study, it does demonstrate the importance of correlative physical examination results to imaging findings. Moreover, it supports the notion that this is a dynamic problem and that while sport participation may lead to radiographic markers consistent with FAI, it does not necessarily correlate with the presentation of symptoms. To that end, based on our data, we recommend an initial period of nonoperative treatment for the patient with hip pain and FAI features, even in the elite athlete. However, if symptoms persist, then surgery should be considered, as the duration of symptoms has been a negative prognostic factor for return to elite-level play. 25
Several studies have discussed the differences in FAI between male and female patients. Shibata and colleagues 25 reported that male athletes were more likely to have mixed-type impingement and that female athletes were more likely to have pincer-type impingement. Nawabi et al 19 found that male sex was a risk factor for undergoing surgery in elite athletes. In contrast, our study did not show any difference in the incidence of FAI between male and female athletes, nor was there a difference in those who went on to surgical management. We did note morphology differences similar to Shibata et al, 25 with female patients having more frequent isolated pincer morphology and male patients having more frequent mixed morphology. With that stated, when compared within similar sports, we were unable to identify differences in the incidence of symptomatic FAI between male and female athletes. As such, this prompts the need for further investigation as to the impact of sex on the development of FAI within the athletic population.
Finally, an increasing body of evidence has developed regarding the treatment of FAI in an athletic population. Both nonoperative and operative treatment modalities have emerged, with authors recommending an individualized approach to treatment. 10,15,18,25,29 Of our 40 patients diagnosed with FAI, 19 (47.5%) were treated nonoperatively during their time as collegiate athletes. They did not have any loss of time from sports documented, and only one athlete retired from sport secondary, in part, to their hip injury. Similarly, 21 hips in 20 patients failed nonoperative treatment and were treated successfully with arthroscopic management, with return to sport at a mean of 6.7 months after surgery. All but one patient managed surgically were able to return to the same level of sport or higher after surgical treatment. Therefore, with proper patient selection, both nonoperative and operative treatment modalities can achieve success in managing elite athletes. Further longitudinal studies are needed to determine the long-term effect of both nonoperative and operative management on the later development of hip osteoarthritis.
Limitations
Several limitations exist with regard to this study. First, it is retrospective and therefore limited in its design. To that end, we are unable to comment on the radiographic prevalence of FAI within this patient population and therefore unable to calculate the percentage of patients who remain asymptomatic or to identify potential at-risk athletes. Future prospective observational studies should be conducted to better delineate the rate of conversion from asymptomatic FAI to symptomatic FAI to help answer these questions. Second, this study utilized a short observational time period (3 years) at a single institution, with a relative short-term follow-up after treatment. A longer observational period would likely provide the most representative incidence data. However, our institution changed reporting software after this time period, so a longer study period was not available within this database. With that stated, we feel that our large number of individual athletes (n = 1332) and high number of musculoskeletal and hip injuries (n = 5319 and 491, respectively) likely mitigate this risk.
It is also possible that athletes developed symptomatic FAI that went unreported within our system and/or they received treatment at an outside facility. We think that this is unlikely, given the collegiate athlete health program and the fact that if an athlete underwent surgery elsewhere, they still would have had to be cleared by the lead author (M.S.) to return to sport and thus be identified. Nonetheless, this is still a small possibility and may lead to underreporting the incidence of FAI or conversion to surgical treatment. Finally, not all sports are represented at our institution, namely, the high FAI prevalence sports of ice hockey and lacrosse, and therefore, this may underrepresent the overall incidence of FAI within a collegiate athlete population.
Conclusion
In this large, multisport NCAA Division I cohort, the overall incidence of symptomatic FAI was 3.0% and represented 13.9% of hip injuries. This represents the true incidence of symptomatic FAI within a contained elite-level athlete population. Hip injuries represented 9.2% of all musculoskeletal injuries within this cohort. The successful management of FAI with return to play was achieved by both nonoperative and operative treatment methods. The relatively low incidence of symptomatic FAI, despite reports of a high prevalence of FAI morphology in athletes, serves to emphasize the importance of clinical evaluations in treating patients with FAI.
Footnotes
Final revision submitted December 1, 2021; accepted December 15, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.R.S. has received consulting fees from Anika Therapeutics, Medacta, and Smith & Nephew; nonconsulting fees and royalties from Smith & Nephew; and honoraria from Medacta. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Stanford University (No. 25191).