
Abstract
Background:
Surgical site infections (SSIs) significantly influence outcomes and health care costs after orthopaedic surgery, but they have not been well characterized for osteochondral allograft (OCA) transplantation with or without meniscal allograft transplantation (MAT).
Purpose:
To characterize the incidence, cost, and risk factors associated with potential or confirmed SSIs after large single-surface, multisurface, or bipolar allograft transplantation in the knee.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Prospectively collected registry data were analyzed for patients who underwent primary or revision OCA transplantation with or without MAT in the knee. The Centers for Disease Control and Prevention (CDC) guidelines were used to define SSIs and calculate the SSI incidence. Both potential and confirmed SSIs were analyzed to determine related treatment methods, calculate associated health care costs, and characterize risk factors based on the OCA surgery type (single-surface, multisurface, bipolar, ±MAT), American Society of Anesthesiologists physical status classification system, surgery duration, length of stay, age, sex, body mass index (BMI), and current tobacco use.
Results:
A total of 224 patients were included in the analysis. There were 2 SSIs in 1 patient that met CDC criteria, such that the incidence for this patient population was 0.9%. An additional 7 patients (3.1%) were examined for potential infections not classified as SSIs. Patients with potential or confirmed SSIs had a significantly higher mean BMI compared to patients with no evidence of an SSI (P <.001). BMI >35 (odds ratio, 9.1) and tobacco use (odds ratio, 6.6) were associated with greater odds for a potential or confirmed SSI. The mean health care costs were $6101 for patients who required additional emergency room visits and/or irrigation and debridement within 90 days postoperatively for potential or confirmed SSIs, $19 for patients with potential superficial incisional SSIs, and $12,100 for patients who experienced a potential or confirmed deep incisional or organ/space SSI >90 days from surgery.
Conclusion:
Large OCA transplantation with and without MAT were associated with a low incidence of confirmed SSIs (0.9%), and patients with BMI >35 and current tobacco use had greater odds of an SSI. Potential and confirmed SSIs were associated with unscheduled appointments, additional surgical procedures, and higher costs.
Surgical site infections (SSIs) are well-documented complex complications that can occur after knee surgery and adversely affect clinical outcomes. Patients who have an SSI after arthroscopic or open knee surgery are at an increased risk for readmission, reoperation, treatment failure, and higher health care costs. 5,16,19,31 The Centers for Disease Control and Prevention (CDC) categorizes joint infections into 3 groups based on severity and timing relative to surgery: superficial incisional, deep incisional, and organ/space SSI. A superficial incisional SSI occurs in the skin or subcutaneous tissue within 30 days after surgery, while a deep incisional SSI occurs within 90 days after surgery and involves the fascia and muscle. Organ/space SSIs occur within 90 days after surgery and are typically defined as deep joint infections. 23 These definitions are used by the Centers for Medicare & Medicaid Services to define an SSI in patients undergoing total knee arthroplasty (TKA) and are closely monitored for determining reimbursement penalties because of their effect on morbidity, mortality, and medical expenditures. 14,15,34 Superficial incisional infections can typically be resolved with the timely use of targeted antibiotics and effective wound management. However, deep incisional and organ/space joint infections are not as easily resolved and may result in longer hospital stays, additional surgical procedures, treatment failure, and diminished quality of life, all of which contribute to the economic burden associated with SSIs. 3,4,6,12,20,33 As such, the rates for SSIs routinely reported are only for deep incisional and organ/space infections, possibly underestimating total SSI rates and associated costs.
The reported incidence of SSIs after knee surgery varies based on a number of patient- and surgery-related factors, ranging from 0.1% for diagnostic arthroscopic surgery to 0.5% for arthroscopic anterior cruciate ligament (ACL) reconstruction, to 2% for TKA, and up to 6.5% for multiligament knee reconstruction. 12,17,18,25,31 In orthopaedic surgery, SSIs have been comprehensively studied in the TKA population, with a reported incidence of deep joint SSIs between 1.6% and 2.1% for primary TKA and increasing to 15.6% for revision TKA. 18 Identified risk factors for an infection after primary and revision TKA include comorbidities, male sex, longer surgery duration, elevated Charlson Comorbidity Index (CCI) score, history of infections, and public health insurance (eg, Medicare or Medicaid). 18,22,26 Patients with SSIs after primary TKA experience longer postoperative hospitalization and longer total inpatient times in the year after surgery compared with patients without SSIs. 16 Further, confirmed infections are associated with drastic increases in overall costs for care in the 90-day postoperative period, such that average total costs range from $12,000 to $60,000 to treat SSIs after primary TKA in the US health care system. 1,2,9,16 These data regarding the incidence, risk factors, complications, morbidity, and costs associated with SSIs after TKA have changed preoperative patient education and preparation, informed cost-effectiveness and value metrics, and improved clinical and patient-reported outcomes, such that they can serve as a model for application to other types of orthopaedic procedures.
Osteochondral allograft (OCA) transplantation in the knee is a standard-of-care surgical procedure that has been performed for >4 decades and has been characterized as an effective surgical treatment option for young, active patients with debilitating knee issues. 8,13,21,24,27,28,30,32 OCA transplantation in the knee continues to grow in clinical use in the United States, and patient outcomes have been well described. 12,30 However, to our knowledge, a comprehensive assessment of SSIs after OCA transplantation in the knee has not been reported. Therefore, the objective of the present study was to characterize the incidence, cost, and risk factors associated with potential and confirmed SSIs after OCA transplantation with or without meniscal allograft transplantation (MAT) in the knee. The study was designed to test the hypothesis that the incidence of confirmed SSIs and associated costs after large single-surface, multisurface, or bipolar allograft transplantation in the knee would align with that reported for arthroscopic ACL reconstruction or primary TKA. 12,18,25,31
Methods
Patient Cohort
Institutional review board approval was received for this study, and all participants provided documented informed consent. Patients at a single institution were prospectively enrolled into a dedicated registry that follows the outcomes of patients undergoing standard-of-care OCA transplantation. All OCAs and meniscal allografts were obtained from tissue banks accredited by the American Association of Tissue Banks and used according to the US Food and Drug Administration classification of a human cell and tissue product under section 361 of the Public Health Service Act.
Included for analysis in this study were registry patients with at least 1 year of follow-up after large single-surface, multisurface, or bipolar OCA transplantation with or without concurrent MAT (between February 2015 and September 2019). Patients enrolled in the registry were excluded from analysis when required data were not available from the electronic medical record (EMR) or registry database. For patients undergoing bilateral OCA transplantation (n = 3), each knee was analyzed individually. OCA surgery type (single-surface, multisurface, bipolar), American Society of Anesthesiologists (ASA) physical status classification system, surgery duration, length of stay, and descriptive information (age, sex, body mass index [BMI], current tobacco use) were collected at the time of surgery for analysis. Patient-reported outcome measures, in conjunction with EMR data regarding subsequent treatment methods and surgical procedures, were used to determine functional OCA survival as previously defined. 27,30
OCA Transplantation Protocol
The standard SSI prevention protocol for our institution was prescribed to each patient. After screening for relevant allergies, patients were instructed to use 2% chlorhexidine gluconate cloths to comprehensively cleanse their entire body the evening before and immediately before being premedicated for surgery. Prophylactic antibiotics (cefazolin, 1-g dose per 70 kg, with a maximum of 2 g) were given intravenously within 30 minutes of the incision and readministered intraoperatively every 3 hours during surgery.
Included patients underwent OCA transplantation for the treatment of ≥1 large (>2 cm2) grade 3 or 4 focal articular cartilage defects in the knee. Patients chose this treatment option over other (nonsurgical or surgical) alternatives after thorough preoperative assessments and counseling as well as approval for coverage by their insurance provider. For all patients, the decision-making and consent process included preoperative counseling with the attending surgeon and joint restoration health care team to discuss the risks and benefits associated with OCA transplantation; set expectations for adherence to postoperative restrictions, rehabilitation, and follow-up appointments; and communicate details of aftercare with the patient and his or her caregivers.
All surgical procedures were performed as previously described. 8,27,30 Single-surface OCA transplantation included unipolar cylindrical or shell grafts for the treatment of a single focal defect on the patella, trochlea, femoral condyle, or tibial plateau. Multisurface OCA transplantation included unipolar cylindrical or shell grafts for the treatment of at least 2 focal defects on the patella, trochlea, femoral condyle, and/or tibial plateau. Bipolar OCA transplantation included cylindrical or shell grafts for the treatment of apposing focal defects on the patella and trochlea or femoral condyle and tibial plateau with or without the associated meniscus. Surgery duration was defined as the time in minutes from the initial incision to wound closure.
Postoperatively, surgical wounds were covered with occlusive petroleum gauze dressing, sterile abdominal pads, cast padding, and elastic bandage material until the patient was discharged from the hospital. Dressing changes using impermeable island dressing and elastic bandage material were performed as needed while the patient was in inpatient care, on the day of discharge, and 5 to 7 days after surgery by the attending physician, resident physician, or nursing staff. Health care team members provided education on wound management, including written instructions regarding bandage and wound care, showering/bathing before suture removal, and a comprehensive postoperative rehabilitation protocol. 10 Patients were instructed to immediately communicate any wound concerns to the health care team and to return 2 weeks after surgery for a wound check and suture removal by the attending physician, resident physician, or nursing staff.
Each patient received procedure-specific postoperative rehabilitation instructions orally and as a written prescription. 10,27 These instructions were also communicated to outpatient physical therapists who were involved in the patient’s postoperative rehabilitation. Physical therapists at our institution were present at preoperative and postoperative clinic visits, provided inpatient therapy, and coordinated outpatient therapy. Patient adherence to the postoperative rehabilitation protocol was monitored and documented based on patient communication and outpatient physical therapy oral and written reports.
Standard-of-care follow-up visits were scheduled for 6 weeks, 3 months (90 days), 6 months, and 1 year after OCA transplantation. These and any other nonscheduled visits or health-related communications were recorded in the EMR.
SSI Definitions
EMRs were reviewed to identify all potential and confirmed SSIs from the time of surgery to the last recorded follow-up encounter. In addition to encounters associated with planned postoperative management for OCA transplantation, other encounters and treatment methods performed were reviewed and recorded. These included emergency department and office visits, irrigation and debridement, antibiotic bead placement, revision surgery, and medications related to potential and confirmed infections including the type and dose. CDC criteria 23 were used to categorize SSIs as follows:
Superficial incisional: An SSI that occurs within 30 days of the procedure; involves the skin or subcutaneous tissue; has purulent drainage, has been confirmed by cultures, or was deliberately opened by the physician (although not tested); and has pain, tenderness, swelling, erythema, or heat.
Deep incisional: An SSI that occurs within 90 days of the procedure; involves deep soft tissue of the incision site; and has purulent drainage, has spontaneous dehiscence along with confirmed cultures or symptoms of an infection such as fever, or was deliberately opened by the physician with confirmed cultures or symptoms of an infection, an abscess, or other evidence detected on a gross or histopathological assessment.
Organ/Space: A deep incisional SSI that occurs within a 90-day period after the procedure; involves any tissue deeper than the fascia or muscle that had been opened or manipulated during the procedure; and has purulent drainage, organisms identified in cultures, an abscess, or other evidence of an infection involving the tissue, joint, or implants detected on a gross or histopathological assessment.
Cost Calculation
Treatment methods for potential or confirmed SSIs were extracted from the EMR, and the costs for these treatment options were converted to Medicare reimbursement rates for a standardized comparison. 7 For medication costs not routinely covered by Medicare Parts A & B, self-pay chargemaster rates from the treating facility were used in analysis. Costs are reported as 2021 US dollars.
Statistical Analysis
All patients in the described cohort were included for analysis. Descriptive statistics including means, standard deviations, ranges, counts, and percentages were calculated. To determine mean differences by OCA surgery type, we used 1-way analysis of variance or the Kruskal-Wallis test. Data were determined to follow a normal distribution using the Shapiro-Wilk test or by visual assessment. The homogeneity of variance was determined using Levene's test. The 2-sample independent t test or Wilcoxon rank sum test was used to identify differences between potential or confirmed infections for continuous variables. For categorical variables, the Fisher exact test for proportions or the chi-square test of association was utilized to identify differences among the risk factors, clinical outcomes, OCA surgery types, or potential or confirmed infections. Odds ratios were calculated when significant differences were noted between those who had potential or confirmed infections and those who did not. Logistic regression models of potential or confirmed infections were used to assess associations, adjusting for surgery duration. Additionally, 2-sided significance was set a priori at P < .05, and R Version 4.0.3 (R Core Team) was used for all analyses.
Results
A total of 224 OCA transplantation with or without MAT procedures occurred during the study period; all 224 of these patients (100.0%) met the study criteria and were included in analysis. All patients had sufficient data documented to determine the 90-day SSI status.
The mean patient age was 37.6 ± 12.3 years, the mean BMI was 28.9 ± 5.2, 120 patients (53.6%) were male, and 20 patients (8.9%) reported that they used tobacco products daily during the 12-month postoperative period. Single-surface OCA transplantation was performed in 55 knees (24.6%), multisurface OCA transplantation was performed in 21 knees (9.4%), and bipolar OCA transplantation was performed in 148 knees (66.1%). The mean BMI was significantly different across OCA surgery types (P = .039), with the lowest BMI in patients undergoing single-surface OCA transplantation and the highest BMI in patients undergoing bipolar OCA transplantation. Patients undergoing single-surface OCA transplantation had a significantly shorter mean surgery duration (P < .001) and length of hospital stay (P < .001). No differences in the rates of concurrent osteotomy or other patient or operative characteristics were observed among OCA surgery types (Table 1).
Patient Characteristics and Surgical Outcomes by OCA Surgery Type a

a Data are reported as mean ± SD (range) or n (%). Bold values indicate a statistically significant difference (P < .05). ASA, American Society of Anesthesiologists; BMI, body mass index; OCA, osteochondral allograft.
Overall, 2 SSIs met CDC criteria for inclusion, such that the incidence of confirmed infections for OCA transplantation in this patient population was 0.9% (2/224 knees) (Table 2). The 2 confirmed SSIs occurred in each knee of the same patient and were associated with separate OCA transplantation procedures performed 2 years apart. In the right knee, a deep incisional infection was documented at the osteotomy site of single-surface OCA transplantation in a patient who underwent concurrent high tibial osteotomy (HTO) to correct a varus malalignment comorbidity. The patient had spontaneous wound dehiscence at the HTO incision site at 15 days postoperatively that was initially treated by the attending physician with wet-to-dry dressing. The patient subsequently presented to the emergency department at 18 days postoperatively when dehiscence worsened and was documented to have an elevated serum C-reactive protein level and erythrocyte sedimentation rate. After an evaluation by the attending surgeon the following day, the wound was irrigated and closed using sutures, and oral antibiotics (500 mg of cephalexin every 12 hours for 14 days) were prescribed. The SSI clinically resolved with this management, and the OCA transplantation incision site and joint were not adversely affected. Functional survival of the OCA for this patient’s right knee was documented in the registry as being >6 years after surgery.
Confirmed CDC-Defined SSIs a
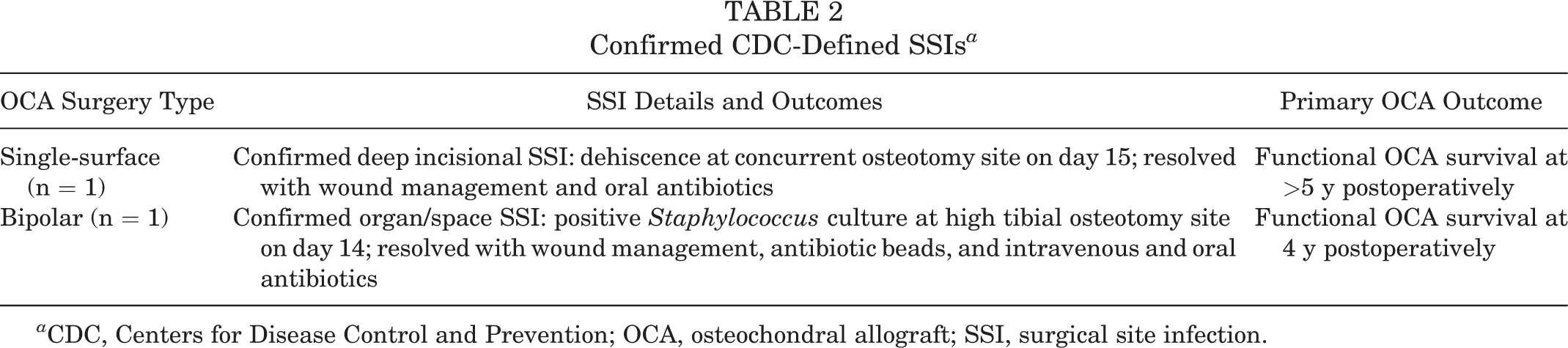
a CDC, Centers for Disease Control and Prevention; OCA, osteochondral allograft; SSI, surgical site infection.
At 14 months after primary OCA transplantation in the right knee, this same patient underwent HTO for realignment of the contralateral (left) lower extremity in preparation for OCA transplantation in the left knee. At 12 months after HTO, primary bipolar OCA transplantation was performed with concurrent revision osteotomy for radiographic nonunion. An organ/space SSI was documented in this patient at the HTO incision site at 14 days after surgery based on cultures from the osteotomy site obtained during irrigation and debridement for wound healing issues noted at the time of suture removal. Microbial cultures showed a growth of Staphylococcus aureus. This SSI was clinically resolved after the placement of 30 antibiotic-impregnated beads (gentamicin, tobramycin, vancomycin) at the osteotomy site for 4 days as well as intravenous antibiotics (2 g of cefazolin every 8 hours for 8 weeks), followed by oral antibiotics (500 mg of cephalexin every 12 hours for 42 days). Consequently, the OCA transplantation incision site and joint were not adversely affected. This patient remained asymptomatic from this SSI with functional survival of the OCA through 4 years after surgery.
An additional 7 patients (3.1%) presented for concerns of potential knee infections after undergoing OCA transplantation that did not meet CDC criteria for classification as an SSI. Of these 7 patients, 3 presented for superficial wound concerns (eg, minor drainage, prolonged redness, focal or diffuse swelling) after bipolar OCA transplantation but had no other evidence of an infection. Further, 2 of the 7 patients (1 with multisurface, 1 with bipolar OCA transplantation) underwent irrigation and debridement because of concerns of joint (organ/space) SSIs based on persistent redness, swelling, and/or effusion; samples collected for comprehensive microbial culture testing produced no growth through 6 weeks of culture. Another 1 of the 7 patients was evaluated at 2 years after primary bipolar OCA transplantation and HTO for radiographic concerns related to osteomyelitis at the HTO site. The HTO plate was removed, and swabs from it showed a growth of methicillin-resistant Staphylococcus sp. The last 1 of the 7 patients had a positive culture of Staphylococcus sp from 1 of 6 routine joint swabs obtained during staged conversion to TKA at 7 months after failed primary bipolar OCA transplantation. In each of these 7 patients, the OCA transplantation incision sites and joints were not adversely affected. Each of these 7 patients with potential infections were managed with oral antibiotic treatment and wound care and remained asymptomatic for an SSI through at least 1 year after resolution.
BMI and surgery duration were significantly greater for all patients with potential or confirmed SSIs compared to patients with no evidence of an SSI. Patients with a BMI >35 had 9.1 times greater odds for a potential or confirmed SSI compared to patients with a BMI ≤35. Patients who reported the daily use of tobacco after surgery had 6.6 times greater odds for a potential or confirmed SSI compared with patients who were not daily tobacco users (Table 3). Because of potential confounding between surgery duration and OCA surgery type, significant relationships were reassessed, accounting for surgery duration. However, all significant relationships remained. No statistically significant associations were noted for potential or confirmed infections with respect to the need for revision OCA transplantation (P = .12) or conversion to TKA (P = .10).
Associations of Risk Factors of SSIs After Allograft Transplantation a

a Data are reported as mean ± SD (range) or n (%) unless otherwise indicated. Bold values indicate a statistically significant difference (P < .05). ASA, American Society of Anesthesiologists; BMI, body mass index; OR, odds ratio; SSI, surgical site infection. Dashes indicate not applicable.
Costs related to potential and confirmed SSIs varied based on severity. For potential infections treated with oral antibiotics (3 patients), the 4-week oral cefalexin prescription cost was $19.14 per patient. Further, 4 patients (2 with potential SSIs, 2 with confirmed SSIs) required additional emergency room visits and/or irrigation and debridement within 90 days of surgery such that the mean cost rose to $6100.71 (range, $1237.18-$9931.42). For the 2 patients with SSIs who presented >90 days from surgery, the mean cost for treatment was $12,100.00 (range, $3556.73-$20,643.52).
In terms of outcomes, the SSIs occurring in the CDC-defined postoperative time period were associated with the need for wound management, irrigation and debridement, antibiotic bead placement, oral and intravenous antibiotics, and/or revision HTO. The SSIs clinically resolved, and the patient has remained asymptomatic with functional survival of the OCAs through 4 years after surgery.
Discussion
Based on the results of the present study, the incidence of confirmed SSIs and associated costs after large single-surface, multisurface, or bipolar OCA transplantation with or without MAT in the knee were within the ranges reported for TKA or arthroscopic ACL reconstruction. 1,2,9,16 The CDC-defined SSI incidence after OCA transplantation of 0.9% compares favorably with those reported for arthroscopic ACL reconstruction (0.5%) and primary TKA (1.6%-2.1%). 18,25,31 Importantly, no arthrotomy incisions, joints, or transplanted tissue were documented to be infected. The US health care–related cost associated with the management of CDC-defined SSIs after OCA transplantation totaled $11,169, which is lower than the range reported for TKA ($12,000-$60,000). 11 A high BMI and tobacco use, which are considered possible risk factors for an SSI after primary TKA, 18,26 were significantly associated with potential or confirmed SSIs after OCA transplantation, even after accounting for surgery duration.
CCI scores were not calculated for patients in the present study based on related contraindications for OCA transplantation, including diabetes mellitus, cardiovascular disease, pulmonary disease, and cancer. As such, CCI scores cannot be compared with those reported for patients undergoing TKA. 29,32 While surgery duration was not found to be a significant risk factor for SSIs after OCA transplantation, as has been reported for primary TKA, the difference in the mean surgery duration is striking. For primary TKA, a surgery duration of >100 minutes was significantly associated with a higher incidence of SSIs. 26 In contrast, the present study recorded <5% of surgical procedures as having a surgery duration of <100 minutes, with the mean surgery duration being 226.8 minutes. Despite these significantly longer surgery durations, the overall incidence of confirmed SSIs was lower than the range reported for primary TKA. These data suggest that surgery duration may not be a large risk factor for SSIs after OCA transplantation in the knee. Similarly, age, sex, American Society of Anesthesiologists (ASA) class, OCA surgery type (single-surface, multisurface, or bipolar), and length of stay were not significantly associated with a higher likelihood for potential or suspected SSIs in this patient cohort, in contrast to that reported for the TKA population.
The present study utilized CDC criteria to define SSIs to conduct fair comparisons with other types of knee surgical procedures and be compliant with the Centers for Medicare & Medicaid Services. Using these criteria, the incidence of SSIs was 0.9% for this OCA transplantation cohort. In addition, 7 patients (3.1%) were evaluated for potential infections that did not meet CDC criteria for classification as an SSI. Symptoms for these patients resolved with treatment, and they remained asymptomatic through at least 1 year after resolution. All potential and confirmed SSIs, from the time of surgery to the last recorded follow-up encounter, were used for risk factor analyses and cost calculations because of the clinical implications for patients and providers. Potential and confirmed SSIs occurring at any point during the postoperative period must be addressed for comprehensive health care. Therefore, while the incidence can be determined based on confirmed infections using the strict CDC criteria, reported risks, treatment methods, and costs should account for all potential and confirmed infections to accurately provide preoperative patient education regarding risks and benefits, insurance coverage, cost-effectiveness, and outcomes.
Limitations
There are several limitations to the present study that should be considered when interpreting and applying the data. This study included a limited population undergoing OCA transplantation with or without MAT at 1 institution using the same infection prevention protocol, transplantation techniques, and postoperative management protocol for all patients. In addition, the utilization of CDC criteria and their constraints regarding the timing of SSIs, as well as the possibility for misdiagnosed or missed SSIs based on interpretations of the criteria, should be considered. Similarly, costs associated with potential or confirmed SSIs may have been underreported based on a lack of standardization among insurance companies with respect to contracted reimbursement payments, which are not made publicly available. Additionally, all costs are based on the US health care system, such that they may not be applicable to other parts of the world. However, the cohort studied is the largest reported to date and was composed of a broad spectrum of patient characteristics and OCA surgery types with comprehensive outcome monitoring in a dedicated registry. Still, it is possible that potential and/or confirmed SSIs were underreported based on data collection methodology, diagnostics performed, and/or incomplete follow-up. Yet, based on the inclusion of all potential and confirmed SSIs for these analyses, the results are accurate with respect to the stated experimental design and provide a fair comparison with other types of knee surgical procedures performed in the United States and reported in the peer-reviewed literature.
Conclusion
The results of the present study suggest that large single-surface and bipolar OCA transplantation with or without MAT in the knee were associated with a low incidence of SSIs (0.9%), which aligns with the SSI incidence for other types of knee surgical procedures. The results suggest that patients undergoing OCA transplantation were most at risk for SSIs when they had a higher BMI (>35) and used tobacco after surgery. All potential and confirmed SSIs in the present study were effectively resolved, and no transplanted tissue or joints were documented to be infected. However, potential and confirmed SSIs were associated with unscheduled appointments, additional surgical procedures, and higher health care costs, highlighting the importance of effective preoperative patient education and engagement in a comprehensive infection prevention protocol that includes attentive postoperative wound management and strict adherence to postoperative restrictions, rehabilitation, and follow-up for centers performing large OCA transplantation with or without MAT in the knee.
Footnotes
Final revision submitted November 16, 2021; accepted December 22, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.P.S. has received research support from Arthrex; consulting fees from Arthrex, DePuy, Orthopedic Designs North America, and Smith & Nephew; and royalties from Thieme. J.L.C. has received research support from Arthrex, DePuy, GE Healthcare, Merial, and Purina; education payments from Sequoia Surgical; consulting fees from Arthrex, Bioventus, and Trupanion; speaking fees from Arthrex; and royalties from Arthrex, Merial, and Thieme. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Missouri (No. 320572).