
Abstract
Background:
Operative treatment is suggested for unstable type 3 acromioclavicular (AC) joint injuries; however, there is no clear consensus regarding the definition of an unstable type 3 injury. We propose a new radiographic method, the “Chiang Mai lean forward” view, to verify horizontal displacement in an unstable AC joint injury.
Hypothesis:
A radiograph taken with the torso leaning forward would allow the detection of a higher proportion of AC joint injuries.
Study Design:
Descriptive laboratory study.
Methods:
A total of 20 shoulders from 10 fresh whole-body cadaveric specimens (mean age, 68.8 years) were tested at 3 different torso leaning angles (30°, 45°, and 60°) to determine the best position for projecting the x-ray beam. The shoulders were dissected sequentially starting with the AC ligament (stage 1), then additional sectioning of the partial coracoclavicular (CC) ligament with either the trapezoid ligament cut first (stage 2A) or the conoid ligament cut first (stage 2B), and finally complete sectioning of the CC ligament (stage 3). Radiography was performed after each stage to evaluate the degree of displacement of the anterior border of the acromion relative to the anterior border of the clavicle. Paired t tests were used to compare the degree of displacement at each stage to that of the shoulder before cutting.
Results:
Leaning at an angle of 30° provided better visualization of the AC joint in the “Chiang Mai lean forward” view. Compared with the intact condition, complete isolated cutting of the AC ligament produced 5.21 mm of horizontal displacement of the AC joint (P < .0001), complete tearing of the AC ligament and partial cutting of the CC ligament resulted in a displacement of <12 mm (7.91 mm at stage 2A [P = .0003] and 8.10 mm at stage 2B [P = .0013]), and complete tearing of both the AC and the CC ligaments resulted in a displacement of 26.37 mm (P < .0001).
Conclusion:
The “Chiang Mai lean forward” radiographic view is a potentially useful tool for determining the degree of the injury and the stability of the AC joint.
Keywords
An acromioclavicular (AC) joint dislocation is a common injury, accounting for up to 9% of all shoulder injuries 12 and 30% to 50% of athletic shoulder injuries. 18 The Rockwood classification system includes 6 types of acute, traumatic AC joint injuries based on the degree and direction of displacement in the anteroposterior (AP) radiographic view. 18 In our clinical practice, we have noticed that many Rockwood type 3 injuries (those having a coracoclavicular [CC] ligament displacement of 25%-100%) had not only vertical instability but also rotational deformity, 14 which was caused by a combination of both vertical and horizontal displacement. In some of the cases in which plain radiographs showed <100% vertical displacement, the patients were treated using nonoperative methods. However, a few months after the injury, some of the patients still had shoulder pain and instability due to scapular dyskinesia. We assumed that this resulted from inadequate healing of the AC and CC ligaments that had not been properly treated.
All of these patients had been evaluated only using radiographs in the AP and transcapular views. After further evaluation, we noted horizontal instability of the AC joint that had not been detected initially on routine plain radiographs. The axillary radiographic view is an option for determining horizontal displacement. 16 Following the standard procedure for performing radiography in this view, the patient should be either sitting or lying down with the shoulder abducted and the elbow resting on the table. However, this position may reduce the degree of deformity and, as a result, will not provide the actual displacement for a correct diagnosis. 16
Decision-making for the treatment of type 3 AC joint injuries is the most highly controversial. 11 The International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS) Upper Extremity Committee subdivides type 3 injuries into subtypes 3A (stable) and 3B (unstable). 6 Its recommendation is that 3 weeks after an injury, a patient with a type 3 injury should undergo radiography in a special view, that is, the Alexander view 1 or the Basamania view, 4 to identify an unstable condition. If the radiograph shows horizontal displacement, the injury should be classified as subtype 3B, for which surgical treatment is recommended. There are also some studies that have recommended measuring the degree of displacement of the distal clavicle and acromion in a modified Alexander view to obtain data on horizontal instability. 9,13
However, we have found that obtaining radiographs either in an Alexander or Basamania view can be difficult in patients with acute-stage AC joint injuries because of the pain and discomfort caused by the positioning of their bodies. Additionally, the rotational effect of the body sometimes obscures the deformity. For these reasons, we propose the “Chiang Mai lean forward” view as a new method for determining the degree of AC joint displacement and instability on radiographs. This position, which uses only gravity, should be more comfortable for patients with acute injuries and should provide a more accurate diagnosis to guide treatment.
To our knowledge, no studies have been published on the quantification of horizontal instability as determined from radiographs with the torso leaning forward. The first objective of this study was to determine the optimal leaning angle for radiographic visualization of the AC joint. The second objective was to determine the correlation between displacement of the AC joint in the “Chiang Mai lean forward” view and the severity of the ligament injury. We hypothesized that a radiograph taken with the body leaning forward could provide more information on horizontal translation for AC joint injuries.
Methods
Institutional review board approval was waived for this cadaveric study. We used fresh-frozen whole-body cadaveric specimens that had been donated to the university. The specimens were thawed in a temperature-controlled room at 4°C for 48 hours and then left at room temperature until they were soft and had regained full range of motion. A total of 20 shoulders from 10 fresh whole-body cadaveric specimens (mean age, 68.8 years [range, 41-88 years]; 3 women and 7 men) were used. The specimens were inspected and underwent standard radiography to exclude those with abnormalities, for example, a complete rotator cuff tear, osteoarthritis of the glenohumeral joint, and severe degenerative changes in the sternoclavicular and/or AC joints.
Experiment Protocol
The “Chiang Mai lean forward” view was obtained by leaning the torso forward and lowering the arm in front of the body, using only gravity to stress the AC joint. The cadaveric specimens were stabilized in a sitting position on a chair using restraining ropes (Figure 1). A block spacer (30°, 45°, or 60°) was placed between the back of the chair and the specimen to control the degree of leaning. The restraining ropes were tied around the costal margin, the iliac crest, the chest wall, the neck, and the eyes in a way that did not restrict scapular motion. Before the experiment, we manually elevated the arms of each specimen in the coronal and sagittal planes and adducted the arms in the horizontal plane. Each movement was repeated 5 times to confirm the mobility of the shoulders and to release any contracture of the shoulders. The shoulder to be investigated was then set in a position that allowed the arm to hang down freely under the force of gravity.

Positioning of a cadaveric specimen for the “Chiang Mai lean forward” view with a block spacer to control the degree of leaning.
The AC and CC ligaments were exposed by making limited 4-cm incisions in the skin and the deltoid attachment along the anterior border of the clavicle and the AC joint. The AC, trapezoid (Tr), and conoid (Co) ligaments were identified. Sequential sectioning of the AC ligament, partial CC ligament, and complete CC ligament was performed without further disrupting the fascia or muscles, starting with stage 0 (healthy, uncut condition). Stage 1 was sectioning of the AC ligament (AC ligament cut), and stage 2 was additional sectioning of the partial CC ligament. This stage was further divided into 2 groups: in stage 2A, the Tr ligament was cut first (AC + Tr ligament cut), and in stage 2B, the Co ligament was cut first (AC + Co ligament cut). Stage 3 consisted of complete sectioning of the CC ligament (AC + CC ligament cut) (Figure 2).

Diagram showing sequential sectioning of the acromioclavicular (AC) and coracoclavicular (CC) ligaments. Co, conoid; Tr, trapezoid.
Radiographic Evaluation
A radiographic examination under C-arm fluoroscopy was conducted at each of the 4 stages of the experiment. Radiographic imaging was performed using a BV Pulsera Mobile C-arm (Philips). The x-ray beam was set parallel to the floor and projected from anterior to posterior of the shoulder. The center of the x-ray beam was directed at the AC joint. A 20-mm metal bar was placed on the skin at the area of the head of the humerus as a reference for distance measurements.
Radiographic Measurements
First, we evaluated different degrees of leaning for the “Chiang Mai lean forward” view by inserting a block spacer of 30°, 45°, and 60° behind the back of the body. Then, at each of the 3 degrees of leaning, we measured translation of the anterior border of the acromion relative to the anterior border of the distal clavicle in millimeters. We drew a line (line AB in Figure 3A) along the AC joint. Then, line CD was drawn through the most anterior point of the distal clavicle and perpendicular to line AB, and line EF was drawn through the most anterior point of the acromion and perpendicular to line AB. The distance between lines CD and EF where they crossed line AB was the length of translation (Figure 3).

(A) Measuring translation of the distal clavicle relative to the acromion on a radiograph using the “Chiang Mai lean forward” view. The black lines represent the outlines of bones. AB is a line along the acromioclavicular joint. CD is a line perpendicular to AB, passing through the most anterior part of the distal clavicle. EF is a line perpendicular to AB, passing through the most anterior part of the acromion. Translation is the distance from CD to EF measured at the point where those lines cross AB. (B) View direction on 3-dimensional computed tomography scan.
All radiographic measurements were performed twice by each of 2 independent examiners who were blinded to the cadaveric data. Intraobserver and interobserver differences were evaluated using the intraclass correlation coefficient (ICC). 20 The ICC was calculated by comparing the results of the 2 examiners. An ICC from 0.00 to 0.40 was rated poor, 0.41 to 0.75 was fair or moderate, and >0.75 was excellent. The 2 examiners performed a second radiographic measurement 4 weeks later. During the second measurement, the examiners had no access to the first measurement or to the other examiner’s measurement during the measuring process.
To determine the feasibility of the study, we decided to conduct a pilot experiment in the first 5 shoulders. The radiographs were evaluated and measured by 2 examiners. We found large variations in the measurements at 45° and 60° of forward leaning. These variations in the radiographs and the resulting low quality made analysis difficult. The 30° forward leaning radiographs, however, allowed the clear identification of bony landmarks and had a low variation in measurements. It was decided to use the 30° forward leaning position for all 20 shoulders to determine the degree of translation of the anterior border of the acromion relative to the anterior border of the distal clavicle.
Statistical Analysis
Results are presented as the mean ± SD and range. Descriptive statistics (paired t tests) were used to analyze the data. A P value of <.05 was considered statistically significant. Statistical analysis was performed using SPSS Version 16.0 (IBM Corp).
Results
The “Chiang Mai lean forward” view at 30° of forward leaning was found to be the best angle because it allowed the clear identification of key bony landmarks, for example, the acromion process, the scapular spine, and the distal clavicle. This degree of leaning also allowed visualization of the AC joint almost as though it were viewed from a superior position, clearly showing the relationship between the acromion and the distal clavicle. With higher degrees of forward leaning (45° and 60°), the bony landmarks were obscured by the overlapping glenoid and scapular bones (Figure 4). The extent of the ligament injury with 30° of forward leaning was evaluated by measuring translation of the acromion process relative to the distal clavicle (Figure 5).
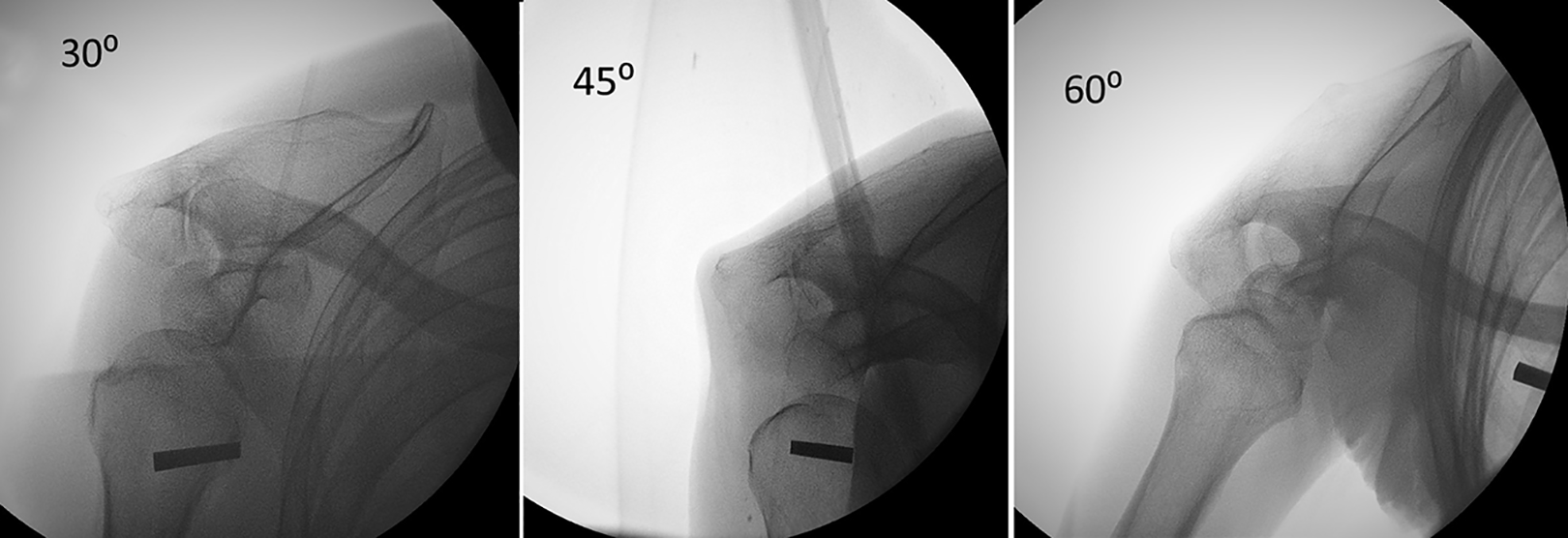
The “Chiang Mai lean forward” view at 30°, 45°, and 60° of forward leaning. The relationship between the distal clavicle and the acromion process was clearer at 30° compared with either 45° or 60°.
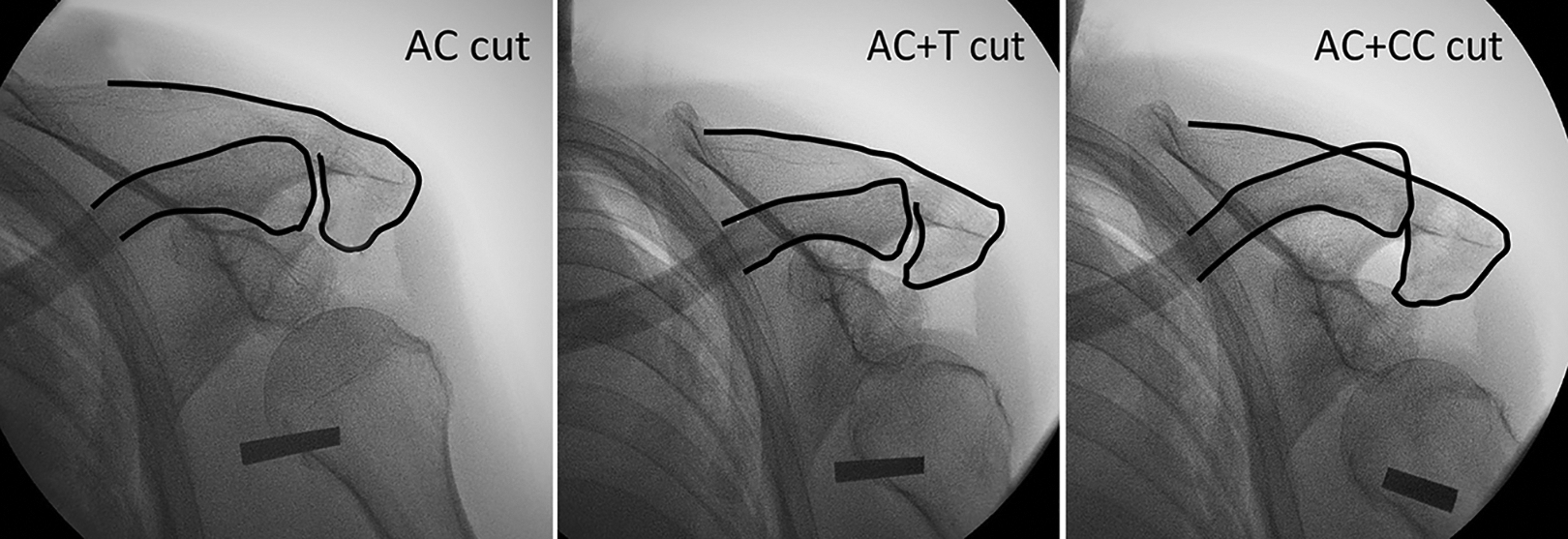
The “Chiang Mai lean forward” view at 30° of forward leaning showing progressive translation of the clavicle and rotation of the clavicle and scapula after sectioning of the acromioclavicular (AC) and coracoclavicular (CC) ligaments. The black lines represent the outlines of bones. T, trapezoid.
At experiment stage 0 (healthy condition), the mean anterior translation of the acromion process was 1.51 ± 1.92 mm. At stage 1, the distance was significantly increased to 5.21 ± 2.36 mm (P < .0001). After partial CC ligament sectioning, the distance was increased to 7.91 ± 2.88 mm at stage 2A (P = .0003) and to 8.10 ± 3.20 mm at stage 2B (P = .0013). There was no significant difference in anterior translation of the acromion whether the Tr or Co ligament was sectioned first (P = .891). At stage 3, there was a significant increase in anterior translation of the acromion: 26.37 ± 5.40 mm (P < .0001) (Table 1).
Displacement of the Anterior Border of the Acromion From the Distal Clavicle a

a Data are reported as mean ± SD (range). Bolded P values indicate a statistically significant difference compared with stage 0 (P < .05). AC, acromioclavicular; CC, coracoclavicular; Co, conoid; NA, not available; Tr, trapezoid.
From our experiment, we found that the anterior borders of the clavicle and the acromion were not always aligned in the intact AC joint. Only 60% of the specimens (n = 6/10) had the anterior border of the acromion and clavicle aligned (<1-mm posterior translation of the distal clavicle relative to the acromion). At stage 0, the difference in anterior translation of the acromion process between the right and left AC joints in the same cadaveric specimen was 0.91 ± 0.98 mm. When the other 4 conditions were compared with stage 0, the difference in anterior translation was statistically significant in all cases (3.69 ± 1.73 mm for stage 1 vs 0 [displacement 1], 6.66 ± 2.23 mm for stage 2A vs 0 [displacement 2A], 6.32 ± 3.11 mm for stage 2B vs 0 [displacement 2B], and 24.85 ± 4.51 mm for stage 3 vs 0 [displacement 3], respectively; P < .0001 for all) (Table 2).
Within these comparisons, there was no significant difference between displacements 2A and 2B (P = .78). However, there were significant differences between displacements 2A and 1 and displacements 2B and 1 (P < .0001 for both).
Comparison of Radiographic Measurements Between Experiment Stages a

a Data are reported as mean ± SD (range). Bolded P values indicate a statistically significant difference compared with stage 0 (P < .05). Stage 0 (healthy), stage 1 (AC ligament cut), stage 2A (AC + Tr ligament cut), stage 2B (AC + Co ligament cut), and stage 3 (AC + CC ligament cut). AC, acromioclavicular; CC, coracoclavicular; Co, conoid; NA, not available;Tr, trapezoid.
Interobserver and Intraobserver Reliability
The interobserver reliability of the 2 independent raters with respect to the radiographic measurements for the 30° leaning forward position was excellent, with an ICC of 0.92. The ICC for intraobserver reliability was also rated excellent, with ICC values for the 2 raters of 0.91 and 0.87.
Discussion
Our study demonstrates the significant difference in displacement of the anterior border of the acromion relative to the anterior border of the clavicle on radiographs taken in the 30° leaning forward position with the arm hanging free. The degree of displacement relates to damage of the structures. Currently, acute injuries of the AC joint are treated based on the degree of instability using the Rockwood classification system. There is, however, some controversy regarding the treatment of Rockwood type 3 injuries. The Rockwood classification system emphasizes the degree of vertical displacement in the AP radiographic view. We believe that displacement can occur in >1 plane. In fact, after an injury, it is the scapula that has been set free from the clavicle rather than the distal clavicle that moves up. The scapula drops down, so when the patient leans forward, the scapula becomes protracted. This rotational deformity results from both vertical and horizontal instability. For this reason, it is very important to detect both vertical and horizontal instability using precise, reliable, and reproducible methods. 7,10,22
Radiography is routinely used as an imaging tool in the assessment of AC joint injuries because the equipment is widely available and provides convincing results. 3,17,19 However, in the literature, there is no consensus regarding the standard view for the radiographic evaluation of acute horizontal instability of the AC joint. 2,15 Additionally, horizontal instability is often neglected or underdiagnosed, which can lead to poor patient outcomes. 2,8,13 In the past, the axillary radiographic view was the standard modality for diagnosing horizontal instability. Later, Rahm et al 16 showed in a cadaveric model that the standard axillary radiographic view of the shoulder can falsely demonstrate posterior translation of the lateral clavicle as a result of patient positioning and projection angles. Tauber et al 21 proposed using a supine, dynamic axillary view to detect horizontal translation in patients with an acute AC joint dislocation. With this method, a measurement of the glenoacromioclavicular angle is used to quantify horizontal instability of the clavicle in terms of angle differences. However, in clinical practice, the dynamic axillary view of Tauber et al is problematic because of its complexity, higher radiation exposure, and additional cost. The ISAKOS Upper Extremity Committee recently suggested using the cross-body adduction view (Basamania/Alexander) for the evaluation of Rockwood type 3 injuries, 6 but there is a lack of a standardized evaluation method and evidence of the advantages of that view over other views.
We propose the “Chiang Mai lean forward” view, which is a dynamic radiographic evaluation method. With this method, stress is created on the AC joint by leaning the torso 30° forward and letting the arm hang down freely under the force of gravity alone. The weight of the arm pulls the scapula forward and downward, creating stress across the AC joint. Fundamentally, 30° of lean is the most suitable for the “Chiang Mai lean forward” view, as it allows clear visualization of the bony landmarks of the anterior acromion and the anterior distal clavicle. A greater degree of leaning produces a less clear radiographic image because of overlapping bony structures. The “Chiang Mai lean forward” view shows the extent of anterior translation and rotation of the acromion relative to the distal clavicle after sectioning of the AC and CC ligaments.
With a Rockwood type 3 AC joint injury, small upward displacement of the clavicle is visible in the AP view on plain radiographs, but in fact, what has happened is that the scapula has dropped down and rotated around the distal clavicle. The Rockwood type 3 classification does not consider horizontal displacement of the AC joint. The “Chiang Mai lean forward” view, however, does consider horizontal displacement and thus can help determine the degree of instability of the AC joint, helping to select the treatment option.
The ISAKOS consensus group on AC joint injuries recommends dividing Rockwood type 3 into type 3A (stable) and type 3B (unstable) by taking a cross-body radiograph at 3 weeks after an injury. Then, if an unstable-type injury is seen on the cross-body adduction radiograph, surgical treatment is recommended. However, because an AC joint injury is a soft tissue injury, it is our opinion that early repair of the ligament can enhance healing. An ideal radiograph is accurate and reproducible, and the procedure can be tolerated by the patient. Even though this radiographic view has worked very well in our patients, it still needs to be scientifically proven that it provides an advantage over other methods and that it is appropriate for use in combination with other methods.
For clinical applications, we do not think that this new radiographic view is useful in cases of gross displacement of the AC joint, for example, Rockwood type 5, because it is clear that the injury has resulted in an unstable condition. In cases of a smaller degree of displacement of the AC joint in the AP view, such as Rockwood type 3, we recommend the “Chiang Mai lean forward” view, as the amount of displacement identifies the degree of the injury of the CC ligament. If displacement is >12 mm, that suggests a complete tear of the CC ligament and a potentially unstable condition. In cases in which the amount of displacement is in doubt, we recommend obtaining a radiograph of the other shoulder for comparison. Our data indicated that the difference in alignment of the distal clavicle and the anterior border of the acromion between the 2 shoulders averages <1 mm; thus, the increment of displacement can be measured as displacement of the injured side minus that of the healthy side. If the difference is >11 mm, it suggests a complete tear of both the AC and the CC ligaments. The next step before recommending the use of this new radiographic procedure will be to evaluate the association between the degree of instability detected on the images and clinical treatment outcomes.
Limitations
Our study had several limitations. First, most of the cadaveric specimens in our study were older, while most AC joint injuries occur in young athletes. We did not have information on the change in elasticity of ligaments in the age group used in the study: the amount of elasticity could potentially affect the degree of displacement. Second, the study was conducted using cadaveric specimens that did not have muscle tone or contraction, something that could make a difference in actual patients. Further prospective clinical studies are needed to evaluate the clinical relevance and therapeutic advantages of this new radiographic evaluation method. Third, in our study, only 60% of the specimens had the anterior border of the acromion and clavicle aligned (<1-mm posterior translation of the distal clavicle relative to the acromion) in the intact AC joint. This percentage is the same as that reported by Barth et al 5 ; that is, uninjured AC joints are aligned in only 60% of cases. Bilateral shoulder radiographs for comparison and interpretation are recommended. Further comparative studies of plain radiography, the lean forward view, and magnetic resonance imaging are needed to confirm the findings of this study.
Conclusion
The “Chiang Mai lean forward” view is a method for the dynamic radiographic evaluation of AC joint injuries, which is useful for detecting horizontal instability of the AC joint. This radiographic view is best performed with the patient leaning forward at 30° and the arm hanging down naturally without extra weight. This view provides a potentially useful description of the relationship between the degree of displacement and AC joint abnormalities.
Footnotes
Acknowledgment
The authors thank the Department of Orthopaedics, Faculty of Medicine, Chiang Mai University as well as Chiang Mai University Hospital for their kind support. They also thank Areerak Phanphaisarn for statistical analysis and Dr G. Lamar Robert for English language editing.
Final revision submitted October 11, 2021; accepted December 22, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the Faculty of Medicine, Chiang Mai University (No. ORT-2562-06324).