
Abstract
Background:
Preoperative coracoid dimensions may affect the size of the bone graft transferred to the glenoid rim and thus the postoperative outcomes of Latarjet coracoid transfer.
Purpose:
To determine the effect of coracoid length and width as measured on preoperative magnetic resonance imaging (MRI) on outcomes after Latarjet treatment of anterior shoulder instability.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were patients who underwent primary Latarjet surgery between 2009 and 2019 and had preoperative MRI scans and minimum 2-year postoperative outcomes. Longitudinal coracoid length was measured on axial MRI sequences as the distance from the coracoclavicular ligament insertion to the distal tip. Comparisons were made between shorter and longer coracoids and between narrower and wider coracoids. The outcomes of interest were recurrent instability, reoperation, complications, return to sport (RTS), and American Shoulder and Elbow Surgeons (ASES) score. Independent-samples t test, Mann-Whitney test, chi-square test, and Fisher exact test were used to compare outcomes between groups, and univariate correlation coefficients were calculated to evaluate the relationships between demographics and coracoid dimensions.
Results:
Overall, 56 patients were included (mean age, 28.4 years). The mean ± SD coracoid length was 21.6 ± 2.4 mm and width 10.0 ± 1.0 mm. Relative to patients with a longer coracoid (≥22 mm; n = 26), patients with a shorter coracoid (<22 mm; n = 30) had similar rates of recurrent instability (shorter vs longer; 6.7% vs 3.8%), complications (10.0% vs 15.4%), reoperation (3.3% vs 7.7%), and RTS (76.5% vs 58.8%) and similar postoperative ASES scores (85.0 vs 81.6) (P ≥ .05 for all). Likewise, relative to patients with a wider coracoid (≥10 mm; n = 27), patients with a narrower coracoid (<10 mm; n = 29) had similar prevalences of recurrent instability (narrower vs wider; 6.9% vs 3.7%), complications (17.2% vs 7.4%), reoperation (3.5% vs 7.4%), and RTS (66.7% vs 68.4%) and similar postoperative ASES scores (87.1 vs 80.0) (P ≥ .05 for all).
Conclusion:
Patients undergoing Latarjet coracoid transfer had similar postoperative outcomes regardless of preoperative coracoid dimensions. These findings should be confirmed in a larger cohort before further clinical recommendations are made.
The shoulder is the most inherently unstable joint in the human body, with primary shoulder dislocation rates ranging from 23 to 24 per 100,000 person-years in the general population and 98 per 100,000 person-years for young men. 18,20,29 Once a patient experiences a primary anterior shoulder dislocation, 39% will develop recurrent instability. 24 Surgical intervention is often recommended after primary anterior shoulder dislocation, especially in young active patients, to minimize the chances of recurrent instability. 3,17,22
Several surgical interventions are available for patients with shoulder instability, such as Bankart repair, capsulorrhaphy, and bone graft fixations into a glenoid defect (usually a Latarjet procedure). Notably, Burkhart and De Beer 7 found that 67% of patients with glenoid deformity (inverted glenoid pear appearance) develop recurrent instability, while only 6.5% without bony deformity experienced recurrent instability after arthroscopic stabilization. Recognition of the need to address bone defects of the glenoid has been well studied, and one such procedure is the Latarjet coracoid transfer. The Latarjet procedure utilizes a coracoid bone block for restoration of the glenoid surface but also provides stability through additional mechanisms. The procedure has been proposed to work by 3 stabilizing mechanisms: (1) the buttress effect of the coracoid bone, (2) the sling effect of the conjoint tendon and subscapularis, and (3) reinforcement by capsular duplication with the released coracoacromial ligament. 5,8
Preoperative coracoid dimensions—namely, the length and width of the coracoid—may affect the size of bone graft transferred to the glenoid rim and postoperative outcomes of Latarjet coracoid transfer. Young et al 28 advised the use of a coracoid bone graft length >25 mm for the Latarjet procedure to enable safe insertion of two 4.5-mm screws. However, a study examining the morphometric analysis of the coracoid process utilizing computed tomography (CT) demonstrated significant differences in dimensions based on age, sex, and ethnicity. 14 Thus, it cannot be assumed that all patients have coracoid dimensions adequate for the Latarjet procedure, and the identification of preoperative coracoid dimensions may help clinicians identify strong candidates for surgery. If coracoid dimensions are insufficient, an alternative bone-grafting procedure may be considered, such as distal tibial allograft or iliac crest grafting. 6,15,23
While preoperative coracoid dimensions have been evaluated utilizing CT, the authors could not identify any studies measuring coracoid dimensions with magnetic resonance imaging (MRI) before Latarjet surgery. Also, no studies have evaluated postoperative outcomes based on preoperative coracoid dimensions in Latarjet cases. Finally, utilizing MRI instead of CT to evaluate preoperative coracoid dimensions may improve the safety and cost-effectiveness of surgical planning before Latarjet surgery. Therefore, the purpose of this study is to determine the effect of coracoid length and width, as measured on preoperative MRI, on outcomes after Latarjet treatment of anterior shoulder instability. We hypothesized that patients with longer and wider coracoid dimensions would have improved postoperative outcomes after Latarjet treatment for anterior shoulder instability.
Methods
Inclusion/Exclusion Criteria
This retrospective cohort study was determined to be exempt from institutional review board approval due to the minimal risk involved with retrospective survey completion and chart review. Patients who had undergone a primary Latarjet procedure as treatment for anterior glenohumeral joint instability from 2010 to 2019 were identified with Current Procedural Terminology code 23462. Common indications for a primary Latarjet procedure included significant glenoid bone loss, recurrent instability after Bankart repair, and participation in high-risk sport. All Latarjet procedures were performed according to the standard technique, with the coracoid osteotomy performed anterior to the coracoclavicular (CC) ligaments and fixation of the coracoid graft to the anteroinferior glenoid with 2 screws. Graft orientation and any concomitant procedures, such as capsular shift or labral repair, were decided by the operating surgeon. Latarjet surgery cases with minimum 2-year follow-up and preoperative MRI of the affected shoulder were included. Patients were excluded if they had a history of ipsilateral shoulder infection, a lack of preoperative MRI, or a history of connective tissue disorder.
Data Collection
Physician chart notes and operative reports were reviewed to collect the following preoperative data: age, sex, hand dominance, surgery laterality, level of sport participation (none, recreational, competitive), contact sport participation, surgical history, and prevalence of chronic recurrent instability (history of ≥5 shoulder dislocations). Intraoperative data were also collected, including the number of screws used for fixation of the coracoid graft, concomitant surgery, and complications. Postoperative complications, recurrent instability, and reoperation were collected from postoperative physician and operative notes. Patients were contacted via RedCap (Vanderbilt University) to complete American Shoulder and Elbow Surgeons (ASES) scores and return to sport (RTS) outcomes at a minimum 2 years postoperatively. Patients who were participating in sport before surgery were included in RTS analysis.
Preoperative 2-dimensional MRI scans were analyzed for coracoid length and width by 3 independent reviewers: 2 research assistants and an orthopaedic surgery resident (R.W.P., D.A.D., D.H.) trained in coracoid dimension measurements by a musculoskeletal radiologist. Instead of measuring longitudinal coracoid length according to previously published CT techniques, 14,19 coracoid length was measured on axial MRI sequences as the distance from the CC ligament insertion to the distal tip to maximize clinical applicability (Figure 1). Because the CC ligament insertion and the distal tip of the coracoid were often on different MRI slices, a specific measurement protocol was utilized by all 3 reviewers (Figure 2). Once the insertion of the CC ligament was identified, the cursor was placed on this insertion. The reviewer scrolled inferiorly until the tip of the coracoid was in view and then found the linear distance from the cursor’s current location (insertion of CC ligament) to the coracoid tip. Width measurements were obtained perpendicular to this coracoid length at 3 locations—5 mm anteriorly from the coracoid base, midpoint, and 5 mm posteriorly from the coracoid tip—to most closely approximate width across the whole transferable coracoid.
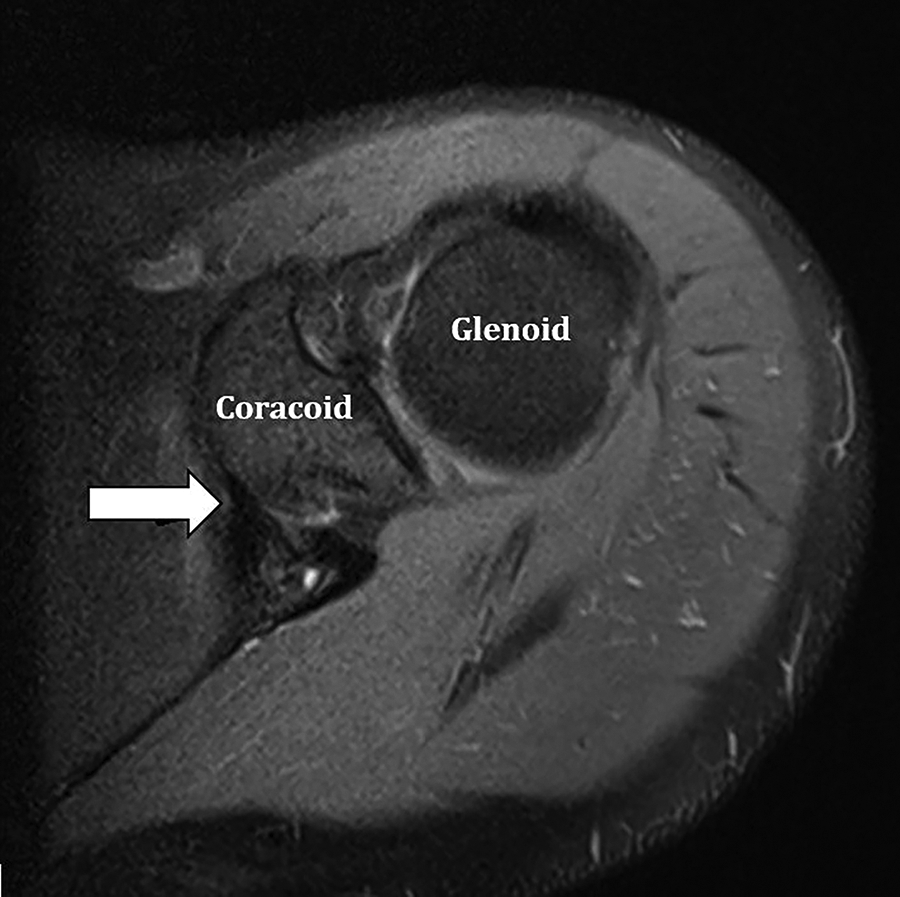
Identification of the coracoclavicular ligament on an axial T2 fat-saturated magnetic resonance imaging slice. The coracoclavicular ligament is the T2 hypointense structure (arrow) seen inserting on the medial margin of the coracoid base.

Demonstration of coracoid width measurements. (A) First, on the coronal oblique T1-weighted sequence, the coracoclavicular ligaments were identified (between the red arrows), outlined by fat, including the more lateral trapezoid ligament and medial conoid ligament. (B) Using scout localizers, the insertion of the coracoclavicular ligaments on the fluid-sensitive axial sequence was identified (red arrow). A line was drawn from this point to the anterior margin of the glenoid (yellow dotted line) denoting the width of the coracoid base. Coracoid width measurements were then collected at 3 locations: 5 mm anteriorly from the coracoid base, midpoint, and 5 mm posteriorly from the coracoid tip (white dotted lines). A straight line from the midpoint of the base to the tip (yellow solid line) was drawn to approximate coracoid length.
Glenoid bone loss was measured by 1 investigator (D.A.D.) utilizing sagittal oblique MRI sequences using the PICO method. 27 A circle of best fit was drawn over the intact margins of the glenoid rim to approximate the normal surface area. The area of the actual glenoid rim (glenoid defect not included) was divided by the area of the expected glenoid rim (a full circle with the glenoid defect) to find the percentage of remaining glenoid bone. Glenoid bone loss was then calculated by subtracting the percentage of remaining glenoid bone by 100%.
Statistical Analysis
Cases were split into short versus long coracoid (<22 vs ≥22 mm) and narrower vs wider coracoid (<10 vs ≥10 mm). These cutoffs were selected as the whole numbers nearest the means of coracoid length and width in this patient cohort, with several CT studies finding a mean coracoid length between 21 and 24 mm. 14,16,19 Demographic and postoperative outcomes were compared between shorter and longer coracoids, narrower and wider coracoids, and male and female coracoid dimensions. Independent-samples t tests were utilized to calculate P values for parametric data, and Mann-Whitney tests were used to calculate P values for nonparametric data. Chi-square and Fisher exact tests were used to calculate P values for categorical data. Univariate correlations were performed to evaluate the relationships between demographics and coracoid dimensions. Relationships with correlation coefficients from 0.0 to 0.19 were considered nonexistent, 0.20 to 0.39 weak, 0.40 to 0.59 moderate, and >0.59 strong. P < .05 was deemed significant. SPSS Version 27.0 (IBM Corporation) was utilized for ICC calculations, and all other statistical analyses were done using R Studio (Version 3.6.3).
Single-measures intraclass correlation coefficient (ICC) was determined to quantify interrater reliability among the 3 raters, using a 2-way mixed effects model and absolute agreement definition. We referenced scales introduced in previously published radiology literature for the interpretation of ICC values, in which <0.50 was considered weak reliability, 0.50 to 0.69 moderate, 0.70 to 0.89 good, and >0.90 excellent. 19
Results
A total of 56 patients who underwent a primary Latarjet procedure with available preoperative shoulder MRI were included in this study. Patients were 28.4 ± 10.1 years of age (mean ± SD), with 9 women and 47 men. There were 34 (60.7%) patients who underwent a Bankart repair before their Latarjet surgery (Table 1).
Reasons Why Included Patients Underwent Latarjet Surgery a

a Only reasons that were similar among ≥3 patients are reported. Bone loss ≥15° was considered significant.
Interrater reliability was good for measuring coracoid length (ICC, 0.79; 95% CI, 0.69-0.87) and coracoid width (ICC, 0.76; 95% CI, 0.46-0.88). Also, no coracoid abnormalities were observed within this patient cohort.
There were no statistically significant demographic differences between groups for coracoid length (<22 vs ≥22 mm) and coracoid width (<10 vs ≥10 mm) (Table 2). Coracoid length averaged 21.6 ± 2.4 mm (range, 16.7-26.9 mm), coracoid width 10.0 ± 1.0 mm (range, 8.3-13.2 mm), and glenoid bone loss 13.7% ± 8.2% (range, 0.0%-32.4%). There was no relationship between coracoid length and coracoid width (R = 0.16) (Figure 3). Coracoid length was weakly correlated with height (R = 0.32) and not correlated with weight (R = 0.11) or age (R =–0.06). Coracoid width was moderately correlated with height (R = 0.42), weakly correlated with weight (R = 0.29), and not correlated with age (R =–0.01).
Differences in Demographics and Intraoperative Variables by Coracoid Length and Width a

a Categorical data are presented as No. (%) and continuous data as mean ± SD.

Scatterplot showing the coracoid dimensions of the 56 patients who underwent a Latarjet procedure. No relationship was observed between coracoid length and width (R = 0.16). Green line, coracoid width group cutoff (10 mm); blue line, coracoid length group cutoff (22 mm); black dotted line, trendline.
All patients who underwent a Latarjet procedure with minimal glenoid bone loss had a preoperative history of chronic shoulder instability, and all these patients either failed an initial Bankart repair or were currently participating in a high-risk sport. There were 41 patients (73.2%) with harvestable coracoid length ≥20 mm. An overall 55 patients received 2 coracoid screws for fixation, and just 1 patient was limited to 1 screw. This patient had a coracoid length of 22.3 mm and a coracoid width of 11.7 mm.
Postoperative complications arose in 7 (12.5%) patients, with no statistically significant difference in complication rate based on coracoid length or width (all P > .05) (Table 3). Three patients required reoperation: (1) an 18-year-old nonathlete man (coracoid length, 20.1 mm; coracoid width, 10.7 mm) had an anterior humeral head subluxation that required Latarjet revision with iliac crest bone grafting and capsulorrhaphy 2.5 years after the primary Latarjet procedure; (2) a 24-year-old man (coracoid length, 23.5 mm; coracoid width, 9.6 mm) developed recurrent instability requiring hardware removal and open capsulorrhaphy 0.6 years postoperatively; and (3) a 21-year-old man (coracoid length, 24.8 mm; coracoid width, 13.2 mm) crashed into a wall while skateboarding and experienced a graft fracture requiring hardware removal with irrigation and debridement 1.6 years postoperatively. This was the only patient to experience a graft fracture. Last, 4 complications that did not require a reoperation involved persistent pain and shoulder locking, temporary nerve injury, surgical site infection, and persistent moderate to severe pain with numbness and tingling.
Postoperative Complications, Recurrent Instability, and Reoperation by Coracoid Length and Width a

a Data are presented as No. (%).
Long-term ASES and RTS outcomes were obtained for 36 (64.3%) patients at a mean follow-up of 4.8 years (range, 2.2-8.1 years). There were no differences in ASES score, RTS rate, or RTS time between groups by coracoid length and width (all P > .05) (Table 4).
Postoperative ASES scores, RTS Rates, and RTS Time by Coracoid Length and Width a

a Categorical data are presented as No. (%) and continuous data as mean ± SD. ASES, American Shoulder and Elbow Surgeons; RTS, return to sport.
Men and women did not differ in regard to mean coracoid length (21.8 ± 2.4 mm vs 20.8 ± 2.5 mm; P = .288) or glenoid bone loss (13.6% ± 7.5% vs 14.5% ± 11.9%; P = .822). However, men did have a wider coracoid than women (10.1 ± 1.0 mm vs 9.3 ± 0.5 mm; P = .001) (Figure 4). Despite this, women had similar postoperative outcomes to men (Table 5).

Difference between female and male patients in mean preoperative coracoid length and width as measured on magnetic resonance imaging. ×, mean; line, median; box, interquartile range; error bars, 95% CI; circle, outlier.
Postoperative Variables Between Female and Male Patients a

a Categorical data are presented as No. (%) and continuous data as mean ± SD. ASES, American Shoulder and Elbow Surgeons; RTS, return to sport.
Discussion
The study findings indicated that there were no significant differences in recurrent instability and reoperation rates, postoperative ASES scores, complications, or RTS between patients with smaller and larger coracoid length or width. Also, no strong relationships were observed between patient demographics (age, height, weight) and coracoid dimensions. Men and women had similar mean coracoid lengths and glenoid bone loss, but men had a wider mean coracoid width. Despite differing mean coracoid widths, men and women had statistically similar postoperative outcomes, but a small cohort of female patients (n = 9) limited the power of this analysis.
Two studies recently described reliable methods of evaluating preoperative coracoid dimensions, although these techniques utilized CT instead of MRI. 14,19 Jia et al 14 performed 3-dimensional reconstruction of 84 shoulder CT scans, but these coracoid length measurements did not account for the clinically relevant anatomy of the coracoclavicular (CC) ligament. Lamplot et al 19 also evaluated multiplanar reconstructed CT scans to evaluate preoperative coracoid dimensions and devised a protocol more specific to the typical osteotomy utilized during the Latarjet procedure. 21 Specifically, the axial view was utilized to identify the anterior aspect of the coracoid base (located at the junction of the vertical inferior pillar and the horizontal superior pillar) and measure its distance from the tip of the coracoid. While this method more closely accounts for the specific landmarks utilized during the Latarjet osteotomy, it still does not represent the intraoperative identification of the CC ligament insertion.
Clinicians frequently use MRI while treating shoulder instability owing to its easy visualization and diagnosis of labral tears. 25,26 Meanwhile, the radiation exposure from a shoulder CT scan has a lifetime attributable risk of cancer around 0.7 per 1000 patients. 13 Thus, the MRI protocol utilized in this study can improve patient safety and decrease health care costs by limiting the necessity of additional CT imaging. 2,13 Surgeons who wish to evaluate coracoid dimensions preoperatively can use this MRI protocol with good interrater reliability to evaluate coracoid length and width during standard-of-care MRI evaluation.
It has been suggested that a coracoid bone graft length of 25 mm or more best enables the safe insertion of two 4.5-mm screws. 28 However, with this MRI protocol, the current study found that all but 1 patient received 2 screws despite most having a coracoid length <25 mm, with none experiencing an acute graft fracture and just 2 receiving a hardware removal procedure. This suggests that the 25-mm cutoff may not be as important as previously noted for a successful Latarjet procedure. 4 For example, Boutsiadis et al 4 found that 96% of patients with 25% glenoid bone loss had adequate coracoid dimensions to restore glenoid anatomy, while 76% with 30% glenoid bone loss had adequate coracoid dimensions. Yet, the Latarjet procedure provides stabilization through other mechanisms as well, such as the sling effect of the conjoint tendon and subscapularis and reinforcement by capsular duplication with the released coracoacromial ligament. 5,8 Thus, measuring coracoid dimensions alone does not evaluate all the relevant stabilization mechanisms, and these other mechanisms may become more important in the setting of significant bone loss. Additionally, the Bristow procedure of coracoid fixation uses a smaller bone block than the Latarjet procedure and a single screw for fixation. While the Bristow procedure has been a successful shoulder stabilization procedure for patients without significant glenoid bone loss, a cadaveric study found that the Bristow procedure may lead to inferior stabilization in patients with significant glenoid bone loss, relative to the Latarjet procedure. 10 Though further research is needed to clarify the bone graft dimensions needed to treat various amounts of glenoid bone loss, surgeons who are treating patients with significant glenoid bone loss may utilize this MRI protocol if they are concerned about the anatomy of the coracoid preoperatively.
Several meta-analyses have evaluated postoperative outcomes for Latarjet surgery. 1,9,11,12 Recurrent dislocations were observed in 1.6% to 5.1% of patients across 4 meta-analyses. 1,9,11,12 Meanwhile, recurrent instability (including dislocations and subluxations) occurs in 2.0% to 12.1% of patients and revision in 2.4% to 5.4%. 1,11 The postoperative complication rate was 5% for complications that required reoperation 1 and 4% for all complications that were not instability related. 9 Finally, 73% (258 of 353) of patients were able to return to sport (RTS) at a mean 5.3 months. 12 Most of these data are in line with the findings of the current study, with the main difference being a lower RTS rate of 63.9%. This may be due to several factors. First, the current study included patients into the RTS analysis who were participating in sport before surgery and responded to long-term RedCap follow-up. Also, a meta-analysis revealed a minimum 15% (575 of 3917) of patients have a previous stabilization procedure, 9 but the majority of patients in this study had a prior shoulder stabilization procedure, which may have contributed to lower RTS rates.
Limitations
This study has several limitations. First, the sample size of this retrospective cohort study was small and may lower the strength of the conclusions drawn. There were just 3 patients with recurrent instability in our cohort, which may have lessened the ability to detect any effect of coracoid size on outcome. The lack of patients with recurrent instability limits the validity of post hoc power analysis findings; thus, a post hoc power analysis was not performed. Also, only 9 female patients were included, restricting the statistical power of the male versus female analysis. For example, previous research with a larger sample size of female patients (n = 29) found that women have shorter coracoid lengths than men 14 ; as such, larger studies comparing male versus female patients are necessary before clinical recommendations can be made. Plus, while the standard Latarjet procedure was utilized for all patients, details regarding graft orientation and indications for concomitant Bankart repair could not be standardized owing to the retrospective design of this study and the various surgeons who performed Latarjet surgery throughout our institution. Finally, intraoperative bone grafts were not measured, so their exact sizes were not determined. However, the general recommendation is to take a sufficient-length bone block that does not disrupt the integrity of the CC ligaments, which we adhered to in our measurement protocol.
Conclusion
Patients undergoing Latarjet coracoid transfer had similar postoperative outcomes regardless of preoperative coracoid dimensions. This MRI protocol for measuring coracoid dimensions has good interrater reliability and closely accounts for the specific landmarks utilized during the Latarjet osteotomy by focusing on identification of the CC ligament insertion. These findings should be confirmed in a larger cohort before further clinical recommendations are made.
Footnotes
Final revision submitted December 5, 2021; accepted December 15, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.B.F. has received education payments from Liberty Surgical, consulting fees from DePuy/Medical Device Business Services, and speaking fees and honoraria from Vericel. M.E.B. has received grant funding from Arthrex, education payments from Arthrex and Smith & Nephew, and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was waived for this study from Thomas Jefferson University (No. 20E.1089).