
Abstract
Background:
Patient satisfaction metrics are commonly used to assess the quality of health care and affect reimbursement. The Press Ganey Ambulatory Surgery (PGAS) is a satisfaction survey that has emerged as a prominent quality assessment tool; however, no data exist on whether PGAS scores correlate with early postsurgical satisfaction during the PGAS survey administration period in patients who underwent anterior cruciate ligament reconstruction (ACLR).
Purpose:
To determine if PGAS scores correlate with measures of satisfaction and patient-reported outcomes (PROs) at 2 weeks postoperatively in ACLR patients.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
A retrospective review of patients who underwent ACLR at a single institution was performed. Patients who completed the PGAS survey and PROs at 2 weeks postoperatively were included in the study. Surgical satisfaction was measured with the Surgical Satisfaction Questionnaire (SSQ-8), and PROs included 6 Patient-Reported Outcomes Measurement Information System domains. Bivariate analysis between PGAS and PRO scores was conducted using the Spearman rank correlation coefficient (r S).
Results:
Of the 716 patients who received the PGAS survey after ACLR, 81 patients completed the survey, and 39 patients also completed PROs and were included in the study. Total converted (mean scaled score) and “top box” (percentages of questions with highest rating selected) PGAS scores showed no significant correlations with the SSQ-8 (r S =–0.24; P = .14). There were no significant correlations between SSQ-8 and PGAS domain scores except for a negative correlation with Facility domain top box scores (r S =–0.33; P = .04), meaning that patients with higher surgical satisfaction had lower PGAS Facility scores. Total PGAS (converted and top box scores) and PGAS domain scores showed no significant correlation with any of the other PROs.
Conclusion:
PGAS scores showed no significant positive correlation with surgical satisfaction, function, pain, mental health, activity, or expectations of surgery in patients 2 weeks after ACLR. This suggests little to no relationship between PGAS score and surgical satisfaction in the early recovery period after ACLR.
As the Centers for Medicare and Medicaid Services (CMS) transitions to a patient experience-centered health care model, satisfaction surveys are increasingly being used to determine the quality of services provided. 21,22 Press Ganey Associates LLC has emerged as a highly regarded patient satisfaction survey vendor as more than 50% US health care institutions have adopted one of their surveys. 35 These surveys carry potential financial implications for both institutions and providers, as hospitals can be penalized up to 2% of base operating diagnosis-related group payments. Further, since the results are available to the public, they can potentially affect the reputation of the institution, leading to a lower patient volume. 22 Although hospital-based outpatient surgery departments and ambulatory surgery centers are not yet required by the CMS to report satisfaction metrics, many institutions have voluntarily begun using these standardized satisfaction metrics in anticipation of future mandated implementation from the CMS. 25
Prior studies have shown that Press Ganey (PG) surveys do not capture satisfaction data that correlate with legacy patient-reported outcomes (PROs) in patients undergoing surgery for degenerative conditions. 6 –8,19 Additionally, most of these studies capture PROs years after PG survey completion, which is administered within days of surgery. Previous studies evaluate correlations between short-term Press Ganey scores with long-term patient-reported outcomes. This study evaluates correlations between short-term PG scores with short-term PROs. 34 On the other hand, patients undergoing anterior cruciate ligament reconstruction (ACLR) are high-functioning individuals who may have different patient experience profiles than those of patients undergoing surgery for chronic conditions. Therefore, sports surgeons should understand the factors associated with PG survey scores in patients undergoing ACLR.
The objectives of this study were to determine if Press Ganey Ambulatory Surgery (PGAS) scores correlate with early surgical satisfaction or PROs in patients undergoing ACLR in the ambulatory surgery setting. By comparing PGAS scores with early surgical satisfaction and PROs, we aimed to elucidate whether patients’ state of health during the PGAS survey administration period is correlated with PGAS scores. We hypothesized that PGAS scores would not be significantly correlated with early surgical satisfaction or with other PROs that measure physical function, pain, mental health, activity level, and expectations.
Methods
After obtaining institutional review board approval, a PG database was retrospectively reviewed for Current Procedural Terminology code 29888 to identify patients undergoing primary or revision ACLR at a single academic ambulatory surgery center between June 2015 and August 2019. All adult patients (≥18 years of age) undergoing primary or revision ACLR were sent the PGAS survey according to our surgery center’s protocol. Exclusion criteria for receiving the PGAS survey were patients admitted to the hospital or incarcerated patients. All surgical procedures were conducted by 4 sports medicine fellowship–trained orthopaedic surgeons (including J.D.P. and R.F.H.) with 3 to 23 years of experience. PGAS surveys were initially sent to patients by mail within a week of surgery. Once the facility’s sampling number of 120 surveys were sent each month, the method of survey administration was switched to email for the remainder of the month for a 100% sampling rate. No patients received both mail and email surveys. For patients receiving the email survey, the emails were sent within a week of surgery and a second reminder email was sent 5 days later if there was no response. The email survey link closed after 30 days, but most responses were typically received within 2 days. The PGAS survey measures the “patient experience” through 35 questions divided into 6 domains: Registration, Facility, Nursing, Physician, Personal Issue, and Overall Assessment. Responses were assessed with a Likert scale of 1 to 5 (very poor to very good) and converted to a score from 0 (very poor) to 100 (very good). 3 Additionally, the percentage of questions with the highest possible rating selected was calculated to obtain the “top box” scores for each patient. 2,3,16 These converted and top box scores were averaged for the total and domain scores for the total cohort.
Patients who completed the PGAS survey were cross-referenced for enrollment in an institutional review board–approved, prospective, single-institution orthopaedic registry with completed 2-week postoperative PROs. 14,28 Patients were included in the orthopaedic registry if they were 18 years of age or older, were English speaking, were not incarcerated or a ward of the state, and were willing and able to participate in the study. Patients with multiligamentous knee injuries were not excluded from the study, but no patients had such injuries in the cohort. The registry questionnaires included 6 domains of the Patient-Reported Outcomes Measurement Information System (PROMIS) computer adaptive test: Physical Function, Pain Interference, Fatigue, Social Satisfaction, Anxiety, and Depression. 4,5,20,27 Knee pain and overall body pain were assessed using the Numeric Pain Scale. 10 Expectations of surgery were assessed with the Expectations domain of the Musculoskeletal Outcomes Data Evaluation and Management System. 15,29,36 Patient physical activity after surgery was measured using the Tegner activity scale. 30 Relevant surgical and patient factors were obtained from the electronic medical record. Questionnaires were administered using the Research Electronic Data Capture data collection system. 12,13
Surgical satisfaction was measured with the Surgical Satisfaction Questionnaire (SSQ-8), which broadly captures satisfaction with the recovery process for the present surgical condition. 11 The SSQ-8 is a validated tool to assess patient surgical satisfaction and includes 8 questions about pain control, performing daily activities, returning to work, exercising, surgical results, likelihood of making the same treatment decision again, and likelihood of recommending the surgery to someone else. Scores ranged from 0 to 100, where higher scores indicated more satisfaction with the surgery performed.
Continuous data were reported as means and standard deviations, while categorical data were reported as frequencies and percentages. The 39 patients who completed both the PGAS and the registry surveys (PGAS + registry cohort) were compared with the 42 patients who did not (PGAS-only cohort) to assess for possible selection bias. Relationships between categorical variables were assessed with chi-square tests. After assessing for normality, continuous variables were compared with independent-samples t tests or 1-way analysis of variance tests for parametric data, and Wilcoxon signed-rank or Kruskal-Wallis tests were used for nonparametric data. Bivariate analysis between continuous variables was conducted using the Spearman rank correlation coefficient (r S). All analyses were performed with JMP Pro Version 13 software (SAS Institute Inc), and P < .05 was used to determine statistical significance. All P values were 2-tailed.
Results
Of the 716 ACLRs performed during the study period, 81 patients (11.3%) completed the PGAS survey. Of the 81 ACLR patients who completed a PGAS survey, 39 patients were enrolled in the orthopaedic registry and completed 2-week postoperative PROs (PGAS + registry cohort). The mean age was 30.1 ± 12.8 years, 44% were male, 68% were White race, and 90% had commercial insurance. The majority (90%) of patients underwent a primary ACLR, 31% had concomitant meniscectomy, and 39% had concomitant meniscal repair. Only 8% had concomitant chondroplasty or microfracture procedures (Table 1).
Baseline Characteristics of Patients in the PGAS + Registry and PGAS-Only Cohorts a

a Values are presented as No. (%) or mean ± SD. ACLR, anterior cruciate ligament reconstruction; PGAS, Press Ganey Ambulatory Surgery survey.
b PGAS + registry patients completed both the PGAS and 2-week patient-reported outcome measures.
c PGAS-only patients completed the PGAS but did not complete 2-week postoperative patient-reported outcome measures.
To assess for selection bias, a comparison between the PGAS + registry cohort and PGAS-only cohort was performed, demonstrating no significant differences in sex, age, race, ethnicity, insurance, surgeon, or primary versus revision ACLR (Table 1). There was a significant difference, however, in the number of patients undergoing a concomitant meniscal repair. There were no significant differences in PGAS scores between groups (Table 2).
Distribution of PGAS Scores a

a Values are presented as mean ± SD. PGAS, Press Ganey Ambulatory Surgery survey.
The mean converted total PGAS score was 93.7 ± 6.8, and the mean top box total PGAS score was 77.8 ± 23.8 (Table 3). The lowest mean domain score was the Facility domain, which had a converted mean score of 87.3 ± 12.6 and mean top box score of 56.9 ± 40.1. The highest mean domain score was the Overall Assessment domain, which had a converted mean score of 98.1 ± 6.2 and a mean top box score of 93.2 ± 23.2. The mean SSQ-8 score was 72.7 ± 14.8. The total PGAS converted and top box scores were not significantly correlated with surgical satisfaction based on the SSQ-8 (Table 3). The only significant correlation between PGAS domain scores and the SSQ-8 scores was for the Facility top box score, which was a weak negative correlation (r S =–0.33; P = .04).
Correlations Between PGAS Scores and the SSQ a
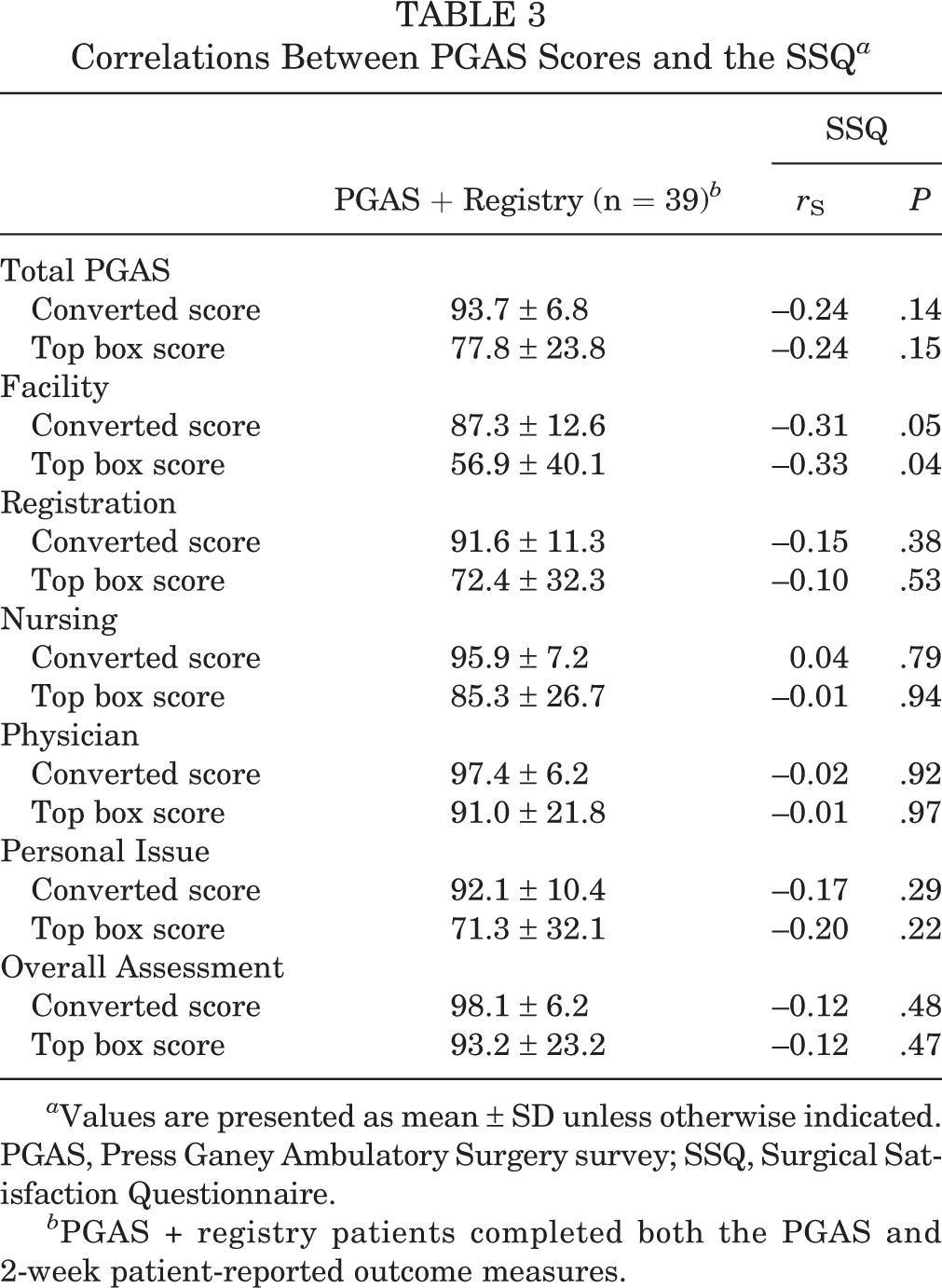
a Values are presented as mean ± SD unless otherwise indicated. PGAS, Press Ganey Ambulatory Surgery survey; SSQ, Surgical Satisfaction Questionnaire.
b PGAS + registry patients completed both the PGAS and 2-week patient-reported outcome measures.
The 2-week postoperative PROs are shown in Tables 4 and 5. There were no significant correlations between any of the PROs and the total PGAS converted or top box scores (Table 4). No significant correlations were observed between 2-week postoperative PROs and PGAS Domain scores (Table 5).
Correlations Between Total PGAS Scores and 2-Week PRO Scores a

a NPS, Numeric Pain Scale; Pain Int, Pain Interference; PF, Physical Function; PGAS, Press Ganey Ambulatory Surgery survey; PRO, patient-reported outcome; PROMIS, Patient-Reported Outcomes Measurement Information System; SS, Social Satisfaction; TAS, Tegner activity scale.
b Spearman correlation coefficient between PROs and total PGAS converted and top box scores.
c Expectations were assessed with the Musculoskeletal Outcomes Data Evaluation and Management System.
Correlations Between PGAS Domain Scores and 2-Week PRO Scores a
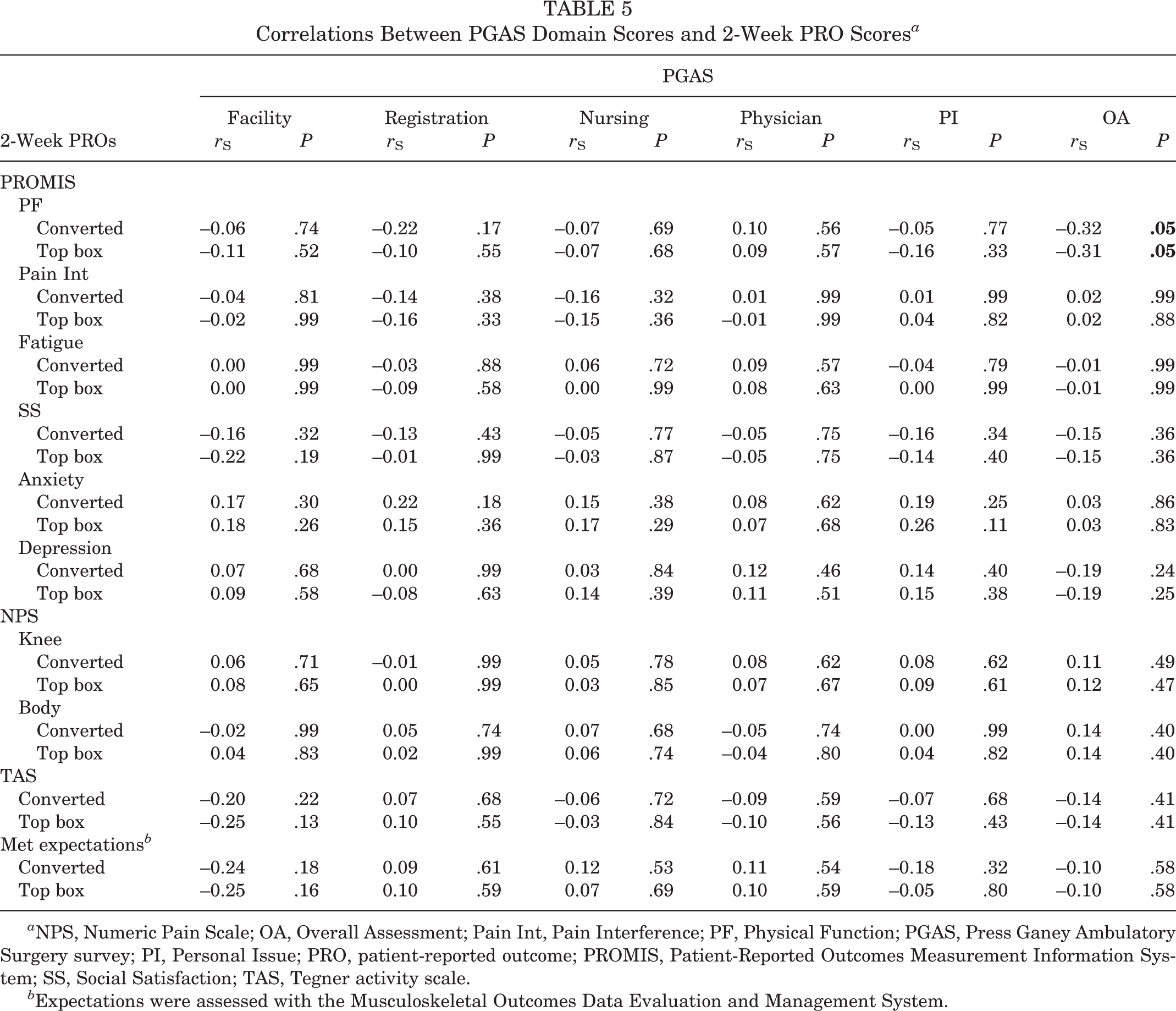
a NPS, Numeric Pain Scale; OA, Overall Assessment; Pain Int, Pain Interference; PF, Physical Function; PGAS, Press Ganey Ambulatory Surgery survey; PI, Personal Issue; PRO, patient-reported outcome; PROMIS, Patient-Reported Outcomes Measurement Information System; SS, Social Satisfaction; TAS, Tegner activity scale.
b Expectations were assessed with the Musculoskeletal Outcomes Data Evaluation and Management System.
Discussion
In patients undergoing ACLR, this study demonstrates that there was no statistically significant positive correlation between PGAS scores and a validated measure of surgical satisfaction, the SSQ-8. 11 In fact, the only statistically significant finding in this study was a negative correlation between SSQ-8 and PGAS Facility domain top box scores (r S =–0.33; P = .04). These findings further support the hypothesis that the PGAS survey evaluates patient satisfaction with a very specific focus on the patient experience at the surgery center, while the SSQ-8 emphasizes satisfaction with surgical results and recovery. Although the results of patient satisfaction metrics are increasingly being used to measure the quality of health care, there is limited research evaluating the correlation of PG scores with other validated postoperative outcome measures in patients undergoing ACLR. Prior studies have shown conflicting evidence that PG scores are correlated with validated PROs, especially in the total joint arthroplasty, spine surgery, and hand clinic populations. 1,6 –8,19,23,24,26,33 This study is important for surgeons and administrators, as improving surgical satisfaction and early recovery do not appear to influence PGAS scores, and more specific efforts are warranted to improve the patient experience.
The lack of correlation between surgical satisfaction, PROs, and PGAS scores contributes to concerns that PG surveys may not accurately capture valid patient satisfaction metrics. Torok et al 31 developed a validated measure of patient satisfaction for hospitalists based on quality of care metrics endorsed by the Society of Hospital Medicine and found no correlation with the PG survey. In the adult orthopaedic population, Joseph et al 18 showed that patient satisfaction measured by the PG survey weeks after discharge was discordant with patient satisfaction reported as an inpatient. Taken together, the lack of concordance between the PGAS survey and SSQ-8 may be explained by the different focuses of each survey, as well as the methods of PG survey administration.
This study contributes to the growing body of literature that shows little to no correlation between PG surveys and PROs. While no studies have evaluated associations between PG scores and PROs in patients undergoing ACLR before the current study, the total joint arthroplasty literature has explored the topic. Chughtai et al 7,8 found no correlations between the PG survey “overall hospital rating” score and various validated outcome assessment tools measuring quality of life, physical function, and activity level years after total knee or hip arthroplasty. Kohring et al 19 similarly found little to no correlation between PG scores and PROMIS Physical Function scores at both 90 days and 1 year after total joint replacement. The lack of correlation with validated PROs extends to other orthopaedic populations, including lumbar spine surgery, where there was noted to be a strong negative correlation between PG score and quality of care as measured by the National Neurosurgery Quality and Outcomes Database 1 year after surgery. 24
Perhaps the lack of correlation may be explained by the time point at which the PROs are measured. Mohamed et al 23 found that multiple PGAS domains were associated with pain intensity within the first 48 hours after total knee arthroplasty during an inpatient stay. Similarly, Tyser et al 33 found positive associations between PG scores and PROMIS (Physical Function, Anxiety, and Pain Interference) scores taken in the waiting room before an appointment in an outpatient hand clinic. Given these previous findings, one would expect surgical satisfaction and PROs to correlate more with PGAS scores if they were obtained during the same time frame. Despite assessing 2-week outcomes in the present study, however, we showed little to no correlation between PGAS scores, surgical satisfaction, and PROs. PG surveys appear to capture data limited to the patient experience during the clinical encounter and do not appear to be correlated with short- or long-term surgical outcomes. Efforts to improve PG scores likely extend beyond striving for excellent surgical outcomes and likely require directed action to improve the patient experience. Furthermore, surgeons should be cautioned to avoid interpreting PGAS scores as assessments of patient satisfaction with surgical outcomes, as the PGAS survey is more accurately reflective of a patient’s overall experience with an ambulatory surgery center.
Limitations
There were several limitations to this study. The small sample size may indicate that this study was underpowered to detect small differences. A total 39 patients provides 80% power to detect a Spearman correlation coefficient of 0.42 with an alpha level of .05. Therefore, the study was appropriately powered to show fair or better correlations between the PGAS score and SSQ-8 or PROs. Furthermore, this study includes all the PGAS responses after ACLR from a single institution over 4 years and accurately represents all the available PGAS satisfaction scores that could be used to determine rankings and reimbursement among participating institutions; however, this may limit study generalizability. PG has stated that only 30 responses are needed to draw meaningful conclusions of a practice. 35
Additionally, the study had a low response rate of 11.3% (81 of 716 ACLRs), which is consistent with response rates in orthopaedic clinic patients of between 8.9% and 16.5%. 9,26,32 Prior studies have shown evidence of nonresponse bias using the same PGAS survey administration methodology used in this study, where the survey administration mode changes from mail to email once 120 surveys are sent out per month. 34 This survey methodology is based on PG’s protocol at our institution, but future studies should assess how such methodology affects response rates and PGAS scores compared with other methods.
Prior studies assessing PG surveys in orthopaedic patients have largely included only the more abundant clinic encounters in heterogeneous populations. Therefore, the smaller sample size in the current study can be explained by including only surgical encounters in a homogeneous group of ACLR patients with a low response rate. Analyzing only patients who underwent ACLR helps control for treatment-specific confounders across different diagnosis-related groups at the expense of sample size. The sample size was further reduced by only including patients who completed 2-week PROs. To assess for possible selection bias, the patients who completed the PGAS survey and PROs (PGAS + registry cohort) were compared with those who did not complete PROs (PGAS-only cohort). The only difference between groups was the rate of concomitant meniscal repair, limiting potential biases.
Another limitation was the potential for recall bias because of the timing of PGAS survey completion, as patients could complete the survey from 48 hours to 6 weeks postoperatively. Such differences in timing could also affect correlations with 2-week PROs, as the orthopaedic registry required patients to complete their surveys between 10 and 21 days postoperatively. Ideally, patients would concurrently complete PGAS surveys and 2-week PROs to make more appropriate comparisons, but this was limited by the retrospective study design. While the SSQ-8 has yet to be validated specifically at the 2-week time point, Howard et al 17 showed that 2-week SSQ-8 scores captured meaningful surgical satisfaction that was correlated with PROs measuring function, pain, and activity level in the general orthopaedic population. In addition, we included patients who underwent revision ACLR, which may bias PGAS responses in those who have failed a prior ACLR by another surgeon. The influence of primary versus revision ACLR should be explored in future studies. Finally, many of the PGAS scores were over 90, which suggests that there may be ceiling effects for these scores.
Conclusion
This is the first study to assess the correlation between the patient experience and surgical satisfaction in the early postoperative phase in patients undergoing ACLR. Postoperative patient experience measures, such as PG surveys, are intended to improve health care quality by linking reimbursement with patient satisfaction. However, patient satisfaction is a complex concept that may reflect different aspects of health care depending on survey design. Our study demonstrated that PGAS scores do not correlate with a validated surgical satisfaction measure at 2 weeks postoperatively. Additionally, PGAS scores were not reflective of other 2-week PROs measuring function, pain, mental health, activity level, and expectations of surgery. This study serves as further evidence that PGAS surveys capture distinct data that appear to be unrelated to early surgical satisfaction and PROs during the PGAS survey administration period. Therefore, PGAS survey satisfaction should not be extrapolated to serve as an indicator of early surgical satisfaction or the current health state of patients undergoing ACLR.
Footnotes
Acknowledgment
The authors acknowledge J. Kathleen Tracy, PhD; Andrew G. Dubina, MD; Julio J. Jauregui, MD; Vidushan Nadarajah, MD; Patrick M.J. Sajak; Joshua M. Abzug, MD; Farshad Adib, MD; Craig H. Bennett, MD; S. Ashfaq Hasan, MD; Vincent Ng, MD; Cameran I. Burt, BS; Shaun H. Medina, MD; Keyan Shasti, BS; Dominic J. Ventimiglia, BS; Alexander J. Wahl, BS; and Michael P. Smuda, MSAT, ATC, for their assistance with data collection.
Final revision submitted November 8, 2021; accepted December 31, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by a grant from James Lawrence Kernan Endowment Fund Inc and a Career Development Award (No. IK2 BX004879) from the US Department of Veterans Affairs Biomedical Laboratory R&D Service. N.L.L. has received grant support from Arthrex and Zimmer Biomet, education payments from Arthrex and Smith & Nephew, and hospitality payments from Wright Medical Technology. J.D.P. has received education payments from Supreme Orthopedics Systems. S.J.M. has received education payments from Arthrex and Smith & Nephew. R.F.H. has received education payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of Maryland, Baltimore (reference No. HCR-HP-00062261-6).