
Abstract
Background:
The intraoperative invisible middle glenohumeral ligament (MGHL) test has been shown to be associated with a subscapularis tendon retraction. However, the preoperative location of the MGHL and its association with subscapularis tear severity has not been evaluated.
Purpose:
To determine (1) the interrater reliability for identification and position of the MGHL, (2) any association between the MGHL position and subscapularis tears, and (3) the cutoff point at which MGHL position can predict subscapularis tear severity.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
The magnetic resonance imaging (MRI) scans and surgical records of 176 patients were retrospectively reviewed by 3 independent orthopaedists. MGHL's identification, level (its position on axial MRI), and medial retraction ratio (distance from the lesser tuberosity to the MGHL divided by the width of the glenoid) were documented, and the interobserver agreement of the 3 indices was assessed. We calculated the association between subscapularis tears and the MGHL level and medial retraction ratio. Receiver operating characteristic (ROC) curve analyses were conducted to establish the optimal threshold of the MGHL medial retraction ratio to predict subscapularis tear.
Results:
The MGHL was identified by at least 2 reviewers in 124 individuals (70.5%). The interobserver reliability was very good for MGHL identification (κ = 0.766), moderate for MGHL level (κ = 0.582), and excellent for MGHL medial retraction ratio (intraclass correlation coefficient = 0.848). A low, positive correlation between MGHL level and subscapularis tear severity was found (Somers d = 0.392, P < .001), as well as a significant association between the medial retraction ratio and Lafosse classification of subscapularis tear size (P < .001). A medial retraction ratio of ≥1.25 had a sensitivity of 0.70, a specificity of 0.83, and a positive likelihood ratio of 4.20, with excellent accuracy (area under the ROC curve = 0.820) to predict severe subscapularis tear.
Conclusion:
The MGHL was identified in 70.5% of shoulder MRIs. The location of the MGHL on preoperative MRI, as described by its level and the medial retraction ratio, was significantly associated with subscapularis tear severity, and a medial retraction ratio of ≥1.25 was predictive of a severe subscapularis tear.
Although subscapularis tendon lesions have been reported in up to 40% of shoulder arthroscopies, 1 this issue has received little attention and has been described as a “forgotten tendon” or a “hidden lesion.” 21,30 The most effective noninvasive tool for the diagnosis of subscapularis tears is magnetic resonance imaging (MRI). However, the diagnostic accuracy of MRI for subscapularis tears varies widely, with sensitivities ranging from 25% to 94% 17,31 and specificities ranging from 64% to 100%, 2,11,16 which is relatively lower than that of overall rotator cuff tears. 25 Therefore, some indirect findings have been used to predict subscapularis tendon tears, such as subluxation of the biceps long head, 19,22 acute inferior angulation of the corocoid, 32 a large degree of coracoid overlap, 7 morphologic abnormalities of the lesser tuberosity and intertubercular groove, 28 and fluid accumulation around the subscapularis. 22,29
The middle glenohumeral ligament (MGHL), one of the infoldings of the glenohumeral capsule, was recently suggested to be associated with subscapularis tendon injuries. 6 Collotte and Nove-Josserand 12 reported that the MGHL inserts distally onto the articular face of the subscapularis tendon rather than directly onto the lesser tuberosity of the humerus, which can explain why it moves medially with subscapularis tear. Lenart and Ticker 23 found that the MGHL is often located medial to the glenoid joint line intraoperatively and is reduced after the subscapularis tendon is repaired. Chauvet et al 10 further named this arthroscopic finding the “invisible MGHL sign.” A positive invisible MGHL sign is an alternative indication of a subscapularis tendon retraction, where relocation of the MGHL can also be found after a repair. However, the invisible MGHL sign is based on intraoperative arthroscopic findings, and the location of the MGHL in preoperative imaging and its association with subscapularis tears have not been discussed.
The purpose of the present study was to determine (1) the interrater reliability for identification and position of the MGHL, (2) any association between MGHL position and subscapularis tears, and (3) the cutoff point at which MGHL position can predict subscapularis tear severity. We hypothesized that a medialized MGHL on a preoperative MRI will be associated with a subscapularis tear and that we can find the cutoff point by which to predict a subscapularis tear.
Methods
Participants
This retrospective study was approved by our institution’s institutional review board. Patients who had undergone an arthroscopic rotator cuff repair surgery by a single surgeon (W.-R.S.) were retrospectively recruited from a medical center in southern Taiwan between January 2017 and December 2019. Patients who presented with shoulder pain or discomfort for more than 3 months that was diagnosed as rotator cuff tear using MRI and who underwent arthroscopic rotator cuff repair surgery, for which there were detailed surgical records at our institution, were included. The exclusion criteria were (1) patients with previous fractures, infections, or previous surgical procedures around the involved shoulder; (2) the period between the MRI and arthroscopic surgery was more than 3 months; and (3) an MRI examination performed on a low-resolution scanner (<1.5 T). 15
Intraoperative Evaluation
All arthroscopic shoulder procedures were performed in the lateral decubitus position. The integrity of the subscapularis tendon was evaluated and recorded by a single senior surgeon (W.-R.S.). The preliminary anatomic and lesion assessments were viewed using a 30° arthroscope in the intraarticular view. To facilitate systemic exploration of the entire attachment status of the subscapularis tendon on the lesser tuberosity, a 70° arthroscope was used, and the upper arm was internally rotated. 5,24 The classification system suggested by Lafosse et al 20 was used to describe subscapularis tear size (Table 1). In addition, to facilitate the classification according to the treatment algorithm, 21 the tear was further classified as (1) no tear; (2) minor tear, which included tears classified as Lafosse type I and type II 21,33 ; and (3) severe tear, which included tears classified as Lafosse types III to V.
Lafosse Classification of Subscapularis Tears

Image Evaluation
All MRIs of the participants were evaluated by 3 orthopaedic surgeons (K.-L.H., H.-M.C., and H.-C.C.) to identify the MGHL, the level of the MGHL on axial MRI, and the medial retraction ratio of the MGHL. Of the 3 orthopaedic surgeons, 1 was visiting staff in the field of sports medicine, 1 had a fellowship in sports medicine, and the other was a senior orthopaedic resident. One of the authors (K.-L.H.) provided the participating orthopaedists with a detailed description of how to identify the MGHL and determine its level and the medial retraction ratio on MRI. The MRIs of the patients and the answer sheets were then sent by email. Thereafter, the 3 participating orthopaedists performed the diagnostic evaluations without specific clinical information about the patients. The data were collected, and the interobserver agreements were analyzed. The MRIs of the included patients were displayed and measured using Digital Imaging and Communication in Medicine image viewing software (πView; INFINITT Co Ltd).
MGHL Identification
To identify the MGHL, some definitions were made according to previous literature. The MGHL has been described as attaching to the anterior-superior labrum of the glenoid proximally and to the anterior aspect of the proximal humerus distally. 3,4,8,18 However, the most visible and valuable aspect of a diagnosis of a subscapularis tear is the middle part, which crosses the superior horizontal border of the subscapularis tendon. 8,10,18 Thus, we defined the “visible MGHL” as follows: (1) a flat or a round structure just posterior to the subscapularis tendon in an axial image, 4 (2) the structure was visible in at least 2 cuts (3 mm) in an axial image, and (3) the structure was located in the middle half of the glenoid corresponding to a coronal image (Figure 1). Shoulder MRIs with a visible MGHL defined by at least 2 observers were then further evaluated for MGHL level and retraction ratio.

T2-weighted axial MRI (left) with the corresponding level on the T1-weighted coronal view (right) in the same patient. The visible MGHL was defined as a flat or round structure just posterior to the subscapularis tendon that was visible in at least 2 cuts in the axial image (arrow in A and B) and was located in the middle half of the glenoid when corresponding to the coronal image. The images also show that the MGHL was located at level 2 in (A) and at level 1 in (B). However, the medial retraction ratios of the MGHL were similar. MGHL, middle glenohumeral ligament; MRI, magnetic resonance imaging.
MGHL Level
The axial view closest to the equator of the glenoid and the midpoint of the MGHL were used to define the MGHL level (Figure 2A). An MGHL located lateral to the tip of the anterior labrum (Figure 2B) was defined as level 1; an MGHL located between the tip of the labrum and the base of the glenoid (Figure 2C) was defined as level 2; and an MGHL located medial to the base of the glenoid (Figure 2D) was defined as level 3. The final level for further analysis was decided by the level that most observers agreed.

T2-weighted axial MRI at the equator of the glenoid. (A) Schematic diagram of the MGHL level according to its position. (B) An MGHL (arrow) located lateral to the labrum was classified as level 1. (C) An MGHL (arrow) located between the tip of the labrum and the base of glenoid was classified as level 2. (D) An MGHL (arrow) located medial to the base of the glenoid was classified as level 3. MGHL, middle glenohumeral ligament; MRI, magnetic resonance imaging.
MGHL Medial Retraction Ratio
To determine the medial retraction ratio of the MGHL, the axial view closest to the equator of the glenoid was used again. The distance between the tip of the lesser tuberosity and the midpoint of MGHL (distance a in Figure 3A) divided by the width of the glenoid (distance b in Figure 3B) was defined as the medial retraction ratio. If the lesser tuberosity and MGHL were not at the same level as the equator of the glenoid, the observers were asked to measure the distance at the level at which the lesser tuberosity and MGHL were visible simultaneously and closest to the equator. However, the width of the glenoid was always defined as that in the equator. The final ratio used for further analysis was decided by the average of the 3 observers.

(A) T2-weighted axial MRI at the level at which the lesser tuberosity and the MGHL can be observed simultaneously, where the distance between the MGHL and the lesser tuberosity was measured as distance a. (B) T1-weighted axial view at the level of the equator of the glenoid, where the width of glenoid was measured as distance b. The medial retraction ratio of the MGHL was defined as a/b. MGHL, middle glenohumeral ligament; MRI, magnetic resonance imaging.
Statistical Analysis
The clinical and demographic characteristics were expressed as either means and standard deviations for continuous variables or numbers and frequencies for discrete variables. First, we evaluated the reliability of the proposed methods to identify the MGHL, to assess the level of the MGHL, and to calculate the ratio of medial retraction of MGHL. The Fleiss kappa statistic was used to assess the interobserver agreement for MGHL identification and MGHL level. 14 Agreement for the kappa statistics was interpreted as poor (<0.40), fair to good (0.40-0.75), and excellent (>0.75) in accordance with Fleiss. The intraclass correlation coefficient (ICC) was used to determine the interobserver agreement related to the MGHL medial retraction ratio.
Second, the characteristics of patients with a visible versus an invisible MGHL were compared. A chi-square test was conducted to evaluate the categorical variables, including sex, the affected side, and the severity of the subscapularis tear. Continuous variables, such as age, were evaluated using unpaired Student t tests.
Third, the utility of these proposed indices was tested. The association between the MGHL level and the severity of the subscapularis tear was examined using the Somers d. The association between the MGHL medial retraction ratio and the subscapularis tear was examined using a binary logistic regression. Receiver operating characteristic (ROC) curve analyses were used to establish the optimal threshold of the MGHL medial retraction ratio, which were aimed toward distinguishing between subjects with advanced subscapularis tears and those without. The independent variable in the analysis was the MGHL medial retraction ratio. The dependent variable was the dichotomous variable based on the Lafosse classification, comprising subjects with advanced tears and subjects with minor tears, as determined using the Youden index. 34 A P value of less than .05 was considered statistically significant. The analyses were performed using SPSS Version 17 (IBM Corp).
Results
Patient Characteristics
A total of 176 patients were enrolled, as shown in the flowchart presented in Figure 4. The average age was 58.7 years, and 96 of the patients were male (54.55%). There were statistically significant differences in age and sex among the different subscapularis tear severities (Table 2). Older male patients tended to have more severe subscapularis tears than younger female patients.
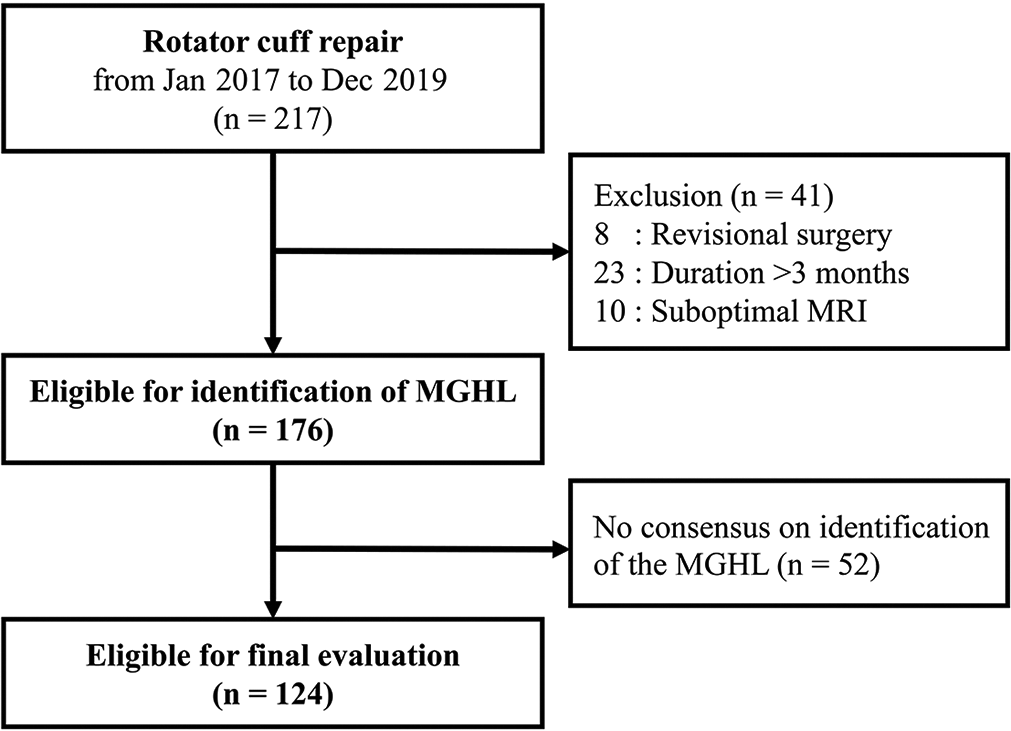
Flowchart of patient enrollment. MGHL, middle glenohumeral ligament; MRI, magnetic resonance imaging.
Patient Characteristics According to Lafosse Classification and Clinical Severity of the Subscapularis Tear a

a Bolded P values indicate statistically significant difference within classifications (P < .05).
Interobserver Agreement for MGHL-Related Assessments
Among the 176 shoulder MRIs, a visible MGHL was defined in 123 shoulders by observer 1, 129 shoulders by observer 2, and 106 shoulders by observer 3. The Fleiss κ coefficient for visible MGHL was 0.766, indicating excellent interobserver agreement. An MGHL was identified by at least 2 observers in 124 shoulder MRIs (70.5%), which made these subjects eligible for further analyses to find the level and the MGHL medial retraction ratio. In those 124 visible MGHLs, 103 (83.1%) were defined by all 3 observers and 21 (16.9%) were defined by only 2 observers. The Fleiss κ coefficient for the level of the MGHL was 0.582, indicating moderate interrater agreement. The ICC for the MGHL medial retraction ratio was 0.848, indicating excellent interobserver agreement.
Comparison of Patients with Visible Versus Invisible MGHL
The age, sex, and affected side were similar between the 2 groups. Regarding the severity of the subscapularis tear, there were no significant between-group differences by Lafosse classification (P = .658) and classification according to clinical severity (P = .880) (Table 3).
Comparison of Patients with Visible Versus Invisible MGHL a
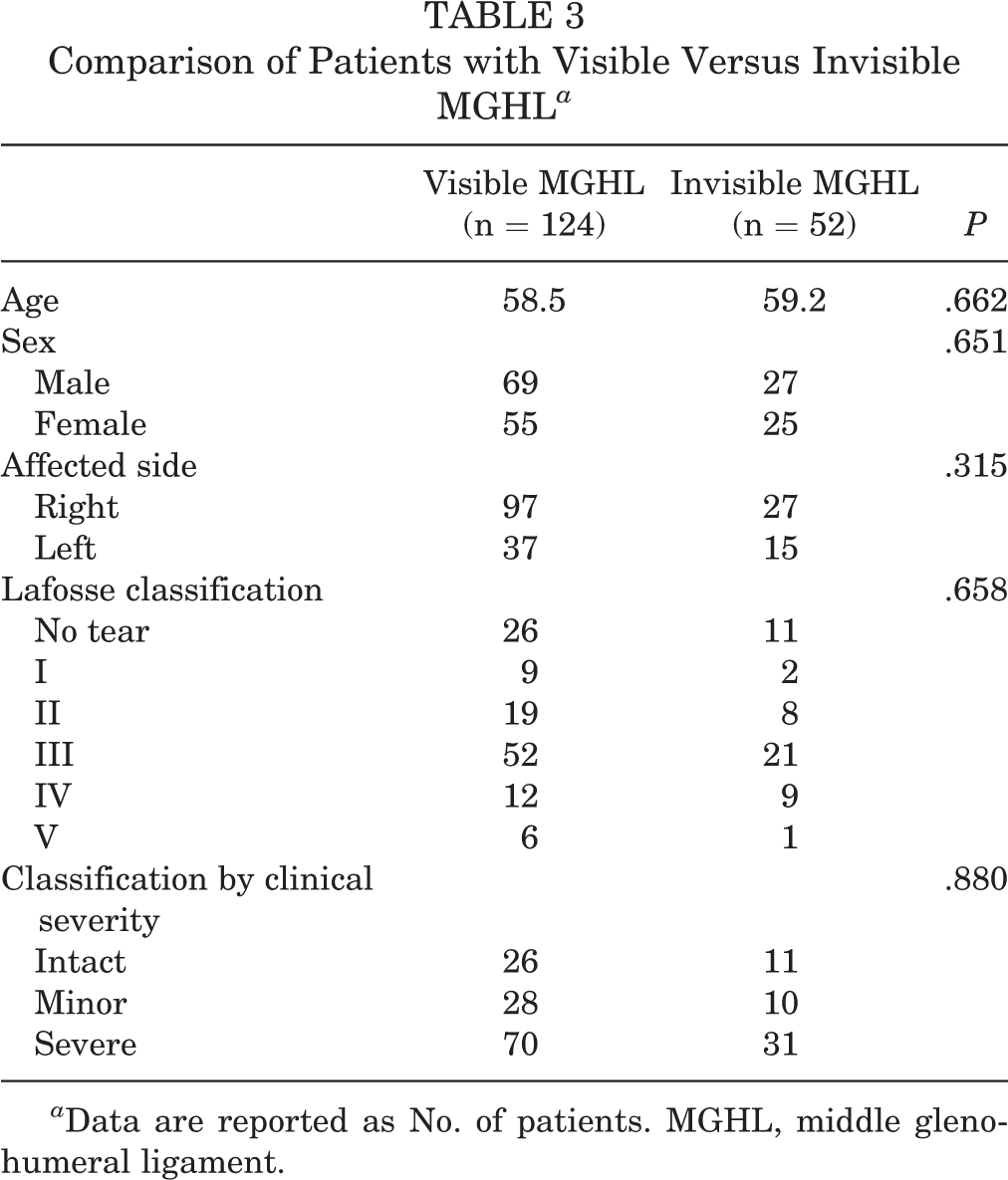
a Data are reported as No. of patients. MGHL, middle glenohumeral ligament.
Association Between MGHL Level and Subscapularis Tear Severity
Among the 124 MRIs eligible for evaluation of the level of the MGHL, the MGHL was defined as level 1 in 54 shoulders, level 2 in 39 shoulders, and level 3 in 31 shoulders, with the severity of the tear increasing at higher levels. The association between the level of MGHL and the severity of subscapularis tear is listed in Table 4. According to the chi-square analysis, a statistically significant association (P = .002) between the level of the MGHL and the severity of subscapularis tear was found. Results of the Somers d analysis indicated a low-to-moderate positive correlation between level of MGHL and Lafosse classification (d = 0.392, P < .001).
MGHL Medial Retraction Ratio
The MGHL medial retraction ratios of the 124 eligible subjects were divided into 6 groups according to the severity of subscapularis tear. A significant association was found between the MGHL medial retraction ratio and the Lafosse classification of a subscapularis tear (P < .001) (Figure 5, Table 4). However, when the subscapularis lesion was classified by the clinical severity (no, minor, or severe tear), there were no significant differences found between the no tear group and the minor tear group, but a significant increase in the MGHL medial retraction ratio in the advanced tear group compared with the no tear group and minor tear group. The ROC curve analysis showed that a medial retraction ratio of MGHL ≥1.25 could effectively discriminate subjects with advanced subscapularis tear from those without. The area under ROC curve was 0.820 (95% CI, 0.746-0.897) (Figure 6), indicating a very good accuracy of the test. The sensitivity and specificity for this threshold was 0.700 and 0.833, respectively, and the positive likelihood ratio was 4.20.

Graphical representation of the average medial retraction ratio of the MGHL for each group with different grade subscapularis tears based on Lafosse classification. The graph includes the different grades according to clinical severity. Green block: no tear or minor tear; pink-red block: advanced tear. MGHL, middle glenohumeral ligament.
Results of Measurements Classified Using the Lafosse Classification and Clinical Severity of the Subscapularis Tear a
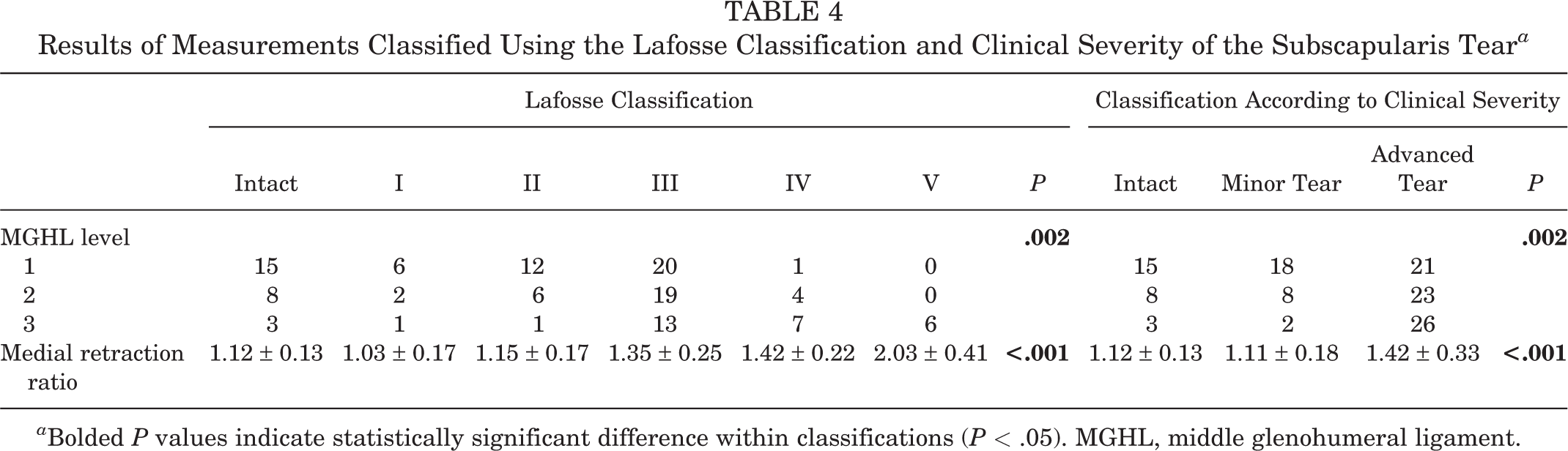
a Bolded P values indicate statistically significant difference within classifications (P < .05). MGHL, middle glenohumeral ligament.

Receiver operating characteristic curve for the medial retraction ratio of the middle glenohumeral ligament with respect to an advanced subscapularis tear.
Discussion
This study was an imaging counterpart of the invisible MGHL test conducted during arthroscopy. Our findings highlight the anatomic proximity between the MGHL and the subscapularis tendon, where a medial retraction ratio greater than the level of the MGHL offers a reliable, accurate measurement by which to distinguish major subscapularis tears from minor tears. In addition, we found that an invisible MGHL does not always signal a subscapularis tear.
The MGHL is known as an anatomic structure with a significant multiplicity of normal variants. 4 The MGHL has been reported to be absent in 15% to 30% of specimens and magnetic resonance arthrographies. 9,27 The proximal attachment of the MGHL is a frequent location of a normal variant, which includes attachment on the labrum at the origin of the superior glenohumeral ligament (SGHL), being separate from the origin of the SGHL, 18 and at the origin of the SGHL and long biceps tendon 4 where, simultaneously, there is also a variance in the distal attachment of the MGHL. However, these normal variances are mainly located around the proximal and distal attachment area but rarely in the middle part, which runs obliquely across the subscapularis. Therefore, we defined the visible MGHL as the presentation of the middle part of the MGHL to avoid the normal variances around the proximal and distal attachment site.
Using this definition, excellent interobserver reliability was found, and the MGHL was defined in 70.5% of the shoulder MRIs, which is similar to the findings in the previous literature on this topic. 9,27 In addition, there were no significant between-group differences in age, sex, and subscapularis tear severity between patients with a visible MGHL and an invisible MGHL. This suggests that the absence of an MGHL may be one of the normal variances in the shoulder rather than a pathological lesion.
According to the invisible MGHL test as described by Chauvet et al, 10 the initial nonvisible MGHL refers to when the MGHL is retracted medially to the glenoid surface and is associated with a subscapularis tear. Therefore, we evaluated the location of the MGHL on an axial view and classified it relative to the position of the labrum. Level 1 MGHL in a preoperative MRI implied that it was easily viewed through initial posterior lateral portal in arthroscopic surgery. In contrast, level 3 MGHL in an MRI implied that the MGHL could be viewed only after pulling the subscapularis laterally. Based on our hypothesis, we found that there was a statistically significant association (P = .002) between the MGHL level and the severity of a subscapularis tear, where a higher level indicated a more severe tear. However, there was only moderate interrater agreement and a low-to-moderate correlation according to Somers d analysis. The relative lower interrater agreement was attributed to the fact that the MGHL is “obliquely” across from the subscapularis rather than perpendicular to it. On an axial view, the MGHL may be located at different levels in different cuts of shoulder MRIs (Figure 1). Although we defined the MGHL level based on the cut closest to the equator of the glenoid, an observer could choose different cuts to evaluate the MGHL level and thus obtain a different result. A high-riding humerus, such as in massive rotator cuff tear, may affect the cut chosen for the level of MGHL. Furthermore, patient positioning may also result in changes in the location of MGHL. 13 The MGHL medially deviates along the articular surface of the subscapularis tendon during internal rotation of the shoulder 13 and is thus likely to blend with the anterior joint capsule in such a case. Based on this, predicting a subscapularis tear only based on the MGHL level may not be entirely reliable.
From observations of arthroscopic surgery, the distance between the MGHL and the lesser tuberosity on the upper margin of the subscapularis is a relatively static value even during rotation of the shoulder. Thus, we measured the distance between the MGHL and the lesser tuberosity in the axial view and divided it by the width of the glenoid for the purpose of standardization. We defined this value as the medial retraction ratio of the MGHL. The results showed an excellent interobserver agreement (ICC = 0.848) for the medial retraction ratio of the MGHL, and a significant association was found between the ratio and the severity of the subscapularis tear. This indicated that the medial retraction ratio of the MGHL is more reliable than the MGHL level in terms of predicting a subscapularis injury.
Although the medial retraction ratio of MGHL was found to be significantly associated with the severity of a subscapularis tear, we failed to find a significant difference between the no tear group and the minor tear group. This implied that the retraction of the subscapularis tendon is not obvious when there is only a minor tear (Lafosse grades I and II). This result was similar to observations described by Martetschläger et al, 26 which showed that a small tear size (<10 mm) in the coronal plane is associated with a shorter tear length (<10 mm) in the axial plane. In addition, in an arthroscopic finding discussed by Collotte and Nove-Josserand, 12 most MGHLs insert distally to the lateral or intermediate part of the subscapularis. Thus, a tear within the proximal third of the subscapularis tendon (Lafosse grades I and II) theoretically results in less tendon retraction.
In contrast, the medial retraction ratio of the MGHL showed excellent predictive power in advanced subscapularis tears. When the medial retraction ratio of the MGHL ≥1.25, the area under the ROC curve was 0.820. This is a useful value for preoperatively predicting the severity of a subscapularis tear, especially when the patient position is not appropriate. An externally rotated shoulder will pull the subscapularis and MGHL laterally, 13 in turn changing the position of the MGHL (Figure 7). In addition, it is difficult to describe the morphology of a tensioned subscapularis tendon. By using the MGHL medial retraction ratio, it is easy to predict a subscapularis tear even when the shoulder is put into an internal or external rotation position.

(A) T2-weighted axial view at the level of the equator of the glenoid. The MGHL (arrow) was classified as level 1 because it was located lateral to the anterior labrum. However, the medial retraction ratio of the MGHL was 36.58/25.77 = 1.42, indicating an advanced tear. (B) Intraoperative findings showed a subscapularis tear >50% and a positive invisible MGHL sign. MGHL, middle glenohumeral ligament.
Limitations
There are some limitations to this study. First, we found a relationship between the preoperative location of the MGHL and the severity of the subscapularis tendon tear, but we were unable to determine the relationship between the preoperative location and the intraoperative invisible MGHL test, because this was a retrospective study. Although both the preoperative location of the MGHL and the intraoperative invisible MGHL test can predict the severity of subscapularis tendon tears, there were still some differences between them. For example, the preoperative MGHL showed no obvious medial retraction in a Lafosse grade II tear but the invisible MGHL test was significantly noted a Lafosse grade II tear. 10 Further prospective studies are needed to determine the relationship between preoperative images and the intraoperative invisible MGHL test. Second, the true length of the subscapularis tendon between the MGHL and lesser tuberosity was not equal to the linear distance between the MGHL and lesser tuberosity because the subscapularis tendon may be curved and closely attached to the anterior surface of the humeral head, especially when the shoulder is put into an external rotation position (Figure 7A). Thus, measuring the linear distance may lead to an underestimation of the true length as well as the medial retraction ratio of the MGHL. Third, by our definition, the MGHL could only be described in 70.5% of the shoulder MRIs in the study. Thus, using the MGHL location could be considered a supplemental method to predict the severity of subscapularis tears, but it cannot be used exclusively.
Conclusion
The study findings indicated that the MGHL can be accurately defined in 70.5% of shoulder MRIs, with excellent interobserver reliability. The location of the MGHL on the preoperative MRIs, as described by its level and the medial retraction ratio, was significant associated with the severity of the subscapularis tear. A medial retraction ratio of the MGHL ≥1.25 was predictive of a severe subscapularis tear.
Footnotes
Acknowledgment
The authors thank Ms Shing-Yun Chang, BS, MSc (Department of Orthopedic Surgery, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan) as well as the Skeleton Materials and Bio-compatibility Core Lab, Research Center of Clinical Medicine, National Cheng Kung University Hospital(NCKUH-11002049) and Ministry of Science and Technology (MOST 110-2314-B-006-021) for their assistance with this project.
Final revision submitted December 9, 2021; accepted December 23, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the Ministry of Science and Technology, Taiwan, and National Cheng Kung University Hospital, Tainan, Taiwan (NCKUH-11002049). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from National Cheng Kung University Hospital (ref. No. A-ER-110-169).