
Abstract
Background:
Emergency department (ED) visits after orthopaedic surgery such as anterior cruciate ligament reconstruction (ACLR) affect patients and health care systems and should be better understood.
Purpose:
To determine the incidence, predictors, and reasons for ED visits within 90 days after ACLR.
Study Design:
Descriptive epidemiologic study.
Methods:
Patients who had undergone ACLR between 2010 and 2020 were identified in a national database, and 90-day ED visits, readmissions, risk factors, and primary diagnoses for visits were determined. One-year postoperative data were used to establish baseline weekly ED visits for the cohort. Patient age, sex, Elixhauser comorbidity index, region of the country (Northeast, Midwest, West, South), and insurance coverage (Medicare, Medicaid, and commercial) were extracted, and these variables were compared using univariate analysis and multivariate logistic regression.
Results:
Out of 81,179 patients, ED visits were identified for 6764 (8.3%), and readmissions were identified for 592 (0.7%). Overall, 5300 patients had 1 ED visit, 1020 patients had 2 visits, 275 patients had 3 visits, and 169 patients had ≥4 or more visits; visits occurred within 2 weeks of surgery 38% of the time. Notably, weekly visits returned to baseline at week 3. Independent predictors of ED utilization from multivariate analysis were insurance type (relative to commercial insurance: Medicaid [odds ratio [OR], 2.41; 95% CI, 2.23-2.60] and Medicare [OR, 1.38; 95% CI, 1.19-1.60]), higher Elixhauser comorbidity index (per 2-point increase: OR, 2.24; 95% CI, 2.18-2.29), younger age (per 10-year decrease: OR, 1.23; 95% CI, 1.21-1.24), female sex (OR, 1.05; 95% CI, 1.02-1.08), and region of the country (relative to the West: Midwest [OR, 1.33; 95% CI, 1.26-1.39], Northeast [OR, 1.24; 95% CI, 1.18-1.30], and South [OR, 1.17; 95% CI, 1.12-1.23]). In the first 2 weeks, 67.5% of ED visits were for issues involving the surgical site, most commonly surgical-site pain (29% of all visits). In the total 90-day period, 39.4% of visits involved the surgical site.
Conclusion:
Within 90 days of ACLR, >8% of patients visited the ED, while 0.7% were readmitted. ED visits increased in the first 2 postoperative weeks and returned to baseline rates around week 3. Within the first 2 weeks, two-thirds of visits involved the surgical site. Younger patients, patients with greater comorbidity burden, those in certain regions of the country, and those with Medicaid had greater odds of ED utilization.
Anterior cruciate ligament (ACL) reconstruction (ACLR) is a common orthopaedic procedure, with >100,000 ACL injuries occurring annually in the United States. 8,12,13,23,29 Most ACLRs are performed for active adolescent and young adult patients, increasingly in the outpatient setting, and postoperative care and rehabilitation have long been considered essential to achieving desirable outcomes. 1,5,11,19
Throughout orthopaedics, postoperative readmissions are a commonly used quality metric, and readmissions rates after ACLR have historically been low, at around 1% to 2%. 3,10,27 However, emergency department (ED) visits have received less attention, although they have been associated with lower patient satisfaction after other procedures and despite the fact that they present a substantial cost to the health care system, representing >$75 billion in aggregate costs in 2017. 9,15,17,22,30,31
The present study made use of PearlDiver, a large national administrative database, to analyze ED utilization within 90 days of ACLR. Specifically, the study aimed to determine the incidence, predictive factors, and reasons for ED visits after ACLR.
Methods
Database and Cohort
The current retrospective cohort study used M53Ortho data set within PearlDiver for the period between 2010 and the second quarter of 2020. This data set contains deidentified information in compliance with the Health Insurance Portability and Accountability Act on nearly 53 million orthopaedic patients in the United States. Our institutional review board granted exemption from review based on the PearlDiver data being aggregated and deidentified.
Patients who had undergone ACLR were identified using the Current Procedural Terminology code 29888 (arthroscopically aided ACL repair/augmentation or reconstruction). Patients were excluded from the study if they did not have minimum 90-day follow-up information in the database. Patients with concomitant knee surgeries were not excluded.
The following patient characteristics were extracted and tabulated: age, sex, Elixhauser comorbidity index (ECI), region of the country based on US Census Bureau definitions (West, South, Midwest, Northeast), and insurance plan (commercial, Medicaid, Medicare).
ED Visits/Readmissions
ED visits were identified based on the occurrence of any of the following Current Procedural Terminology codes that correspond to ED visits consisting of specific aspects of care (99281, 99282, 99283, 99284, and 99285). These codes were used to determine the total number of ED visits within 90 days of ACLR, as well as the weekly incidence of ED visits. For comparison, the cohort’s weekly incidence of ED visits 1 year after surgery was determined by averaging incidences from weeks 52 to 56. For these calculations, patients were excluded if they were not followed in the database for at least 56 weeks after ACLR.
Reasons for ED visits were determined based on International Classification of Diseases (ICD) codes listed as the primary diagnosis for visits. From PearlDiver, a list of ICD diagnosis codes and the number of patients with each code listed as primary diagnosis for an ED visit was extracted. The codes were categorized manually as pain, swelling/effusion, infection, wound dehiscence/bleeding, other surgical-site care/issues, central nervous system (CNS)/psychiatric, gastrointestinal, infection outside the surgical site, cardiovascular, other musculoskeletal, respiratory, and genitourinary. These categories were further dichotomized as involving the surgical site directly (pain, swelling/effusion, infection, wound dehiscence/bleeding, other surgical-site care/issues) or involving other body systems (CNS/psychiatric, gastrointestinal, infection outside the surgical site, cardiovascular, other musculoskeletal, respiratory, genitourinary). While some events in other categories, such as gastrointestinal (constipation), infection outside the surgical site (pneumonia, urinary tract infection), and cardiovascular (pulmonary embolism, deep vein thrombosis), may have been related to surgery, we dichotomized based on surgical-site involvement to illustrate ED visits that had the greatest probability of being associated with surgery. Because observation-level information is not available in PearlDiver, many visits coded as potentially related concerns (eg, constipation, pneumonia) may or may not have been related.
Readmissions for any reason were identified by searching for occurrence of inpatient codes. Patients were categorized as readmitted if they had any inpatient Current Procedural Terminology code or inpatient ICD code within 90 days of ACLR. Those who were readmitted were assessed for readmission from the ED compared with other pathways.
Data Analysis
Characteristics of patients with and without ED visits after ACLR were compared using univariate analysis. Mean age and ECI were compared using the Welch t test. Sex, region, and insurance plan were compared using Pearson chi-square test. A multivariate logistic regression model was built to determine the relative effects of independent patient characteristics.
All statistical tests were performed using PearlDiver. For all analyses, significance was defined as P < .05. Figures were constructed using Microsoft Excel (Microsoft Corporation) and Prism 9 (GraphPad Software).
Results
Study Cohort and Incidence of ED Visits and Readmissions
A total of 84,138 patients undergoing ACLR were identified, of which 2959 (3.5%) were excluded because they were not followed in the database for the entire 90-day postoperative period. The final study cohort was 81,179 patients, with 5.5% visiting the ED within 30 days of ACLR and 8.3% visiting the ED within 90 days of ACLR (Figure 1). Of these 81,179 patients, 15,593 had concomitant knee surgeries, with 1216 (7.8%) of this subgroup visiting the ED within 90 days of ACLR. All 81,179 patients were analyzed together for the remainder of the study.
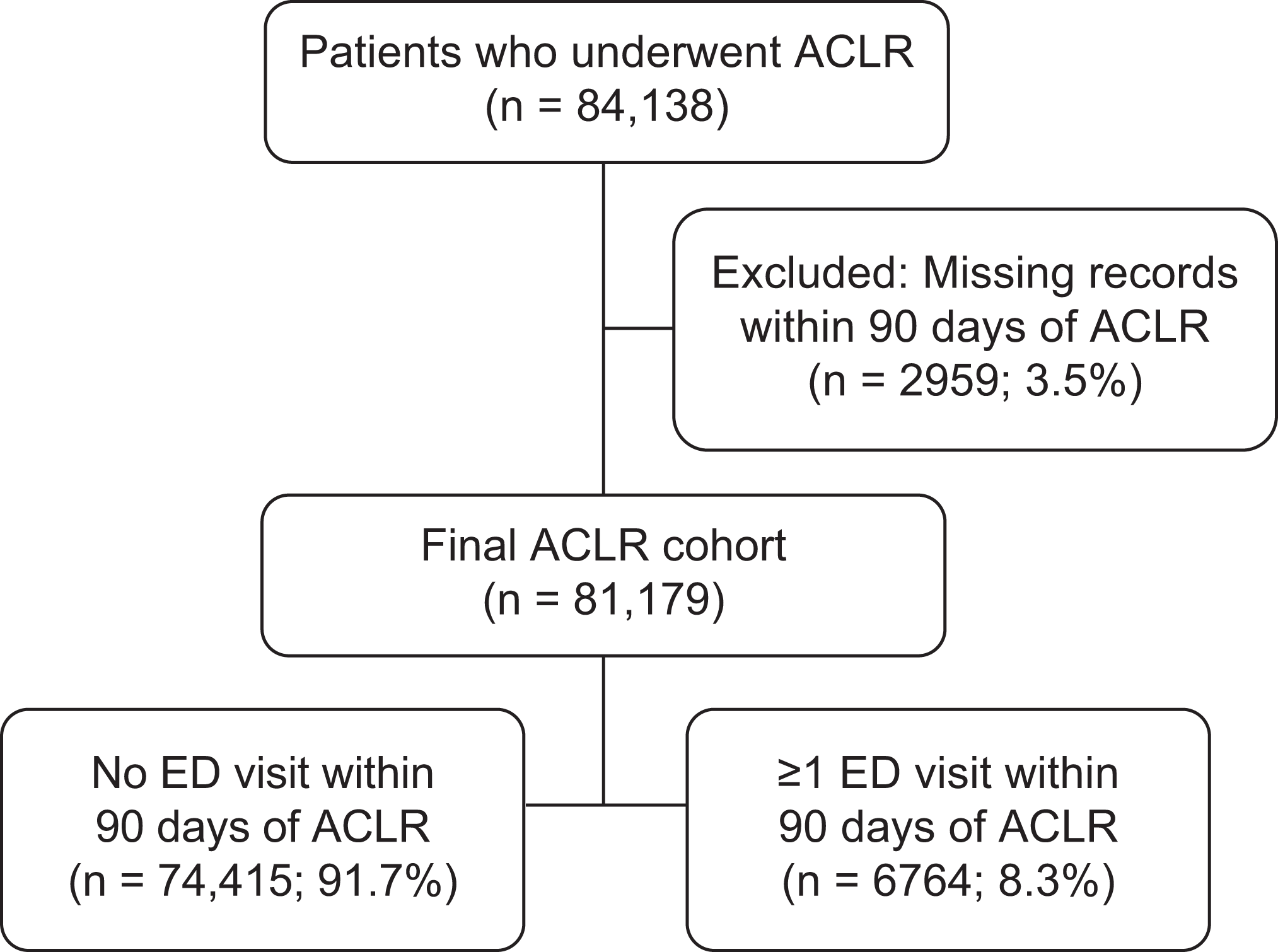
Flow diagram showing designation of study cohorts. ACLR, anterior cruciate ligament reconstruction; ED, emergency department.
The distribution of ED visits by week is shown in Figure 2. For those who returned to the ED within 90 days of ACLR, 1 ED visit was noted for 5300 patients; 2 ED visits, for 1020; 3 ED visits, for 275; and ≥4 ED visits, for 169. Notably, 38% of ED visits occurred within 2 weeks of surgery. The incidence of visits in the first week after surgery was 3% (n = 2406) of the entire study population, and the incidence in week 2 was 1.3% (n = 1031) of the entire study population. Because the weekly incidence of ED visits appeared to plateau after week 2, the rate of ED visits at 1 year after ACLR was assessed. From weeks 52 to 56, the average (±SD) proportion of the study population visiting the ED was found to be 0.67% (±0.04%), ranging from 0.63% to 0.73%The incidence of ED visits at week 3 (0.68%) was within 1 SD of the baseline value.

Pie chart showing the overall incidence of ED visits after ACLR. The graph shows the incidence of ED visits by weeks after ACLR; multiple ED visits by the same patient are represented individually. The 1-year baseline rate of weekly ED visits was determined by averaging the weekly visits for 5 weeks at the 1-year mark after ACLR; the error bar indicates SD, showing that visits in week 3 were within 1 SD of baseline. ACLR, anterior cruciate ligament reconstruction; ED, emergency department.
For comparison with the 8.3% of patients with postoperative ED visits, 90-day readmissions for the study population were assessed and found in 592 patients (0.7% of the study population and 8.8% of those returning to the ED). Out of the 592 readmissions, 564 occurred from the ED.
Factors Associated With Postoperative ED Utilization
Patient characteristics of the identified study cohort are shown in Table 1. Overall, the study population of 81,179 had an average age of 31.7 ± 13.6 years with slight female predominance (50.7%); the patients had relatively few comorbidities as measured via their ECI---an index of patient comorbidities defined by ICD diagnosis codes---(average ECI, 1.3 ± 1.8), they were distributed evenly throughout the country, and most had commercial insurance (88.4%). On univariate analysis, each of these variables besides age (P = .12) was found to be correlated with whether patients returned to the ED in the 90-day postoperative period (P < .001).
Univariate Analysis of Characteristics of Patients With ACLR a

a Data are reported as mean ± SD or n (%). Bold values indicate statistically significant difference between groups (P < .05). ACLR, anterior cruciate ligament reconstruction; ECI, Elixhauser comorbidity index; ED, emergency department.
Multivariate logistic regression was performed, and results are presented in Table 2. Postoperative ED visits after ACLR were independently associated with younger age (for each 10-year decrease: odds ratio [OR], 1.23; 95% CI, 1.21-1.24), female sex (OR, 1.05; 95% CI, 1.02-1.08), higher ECI (for each 2-point increase: OR, 2.24; 95% CI, 2.18-2.29), certain regions of the country (OR range, 1.17-1.33), and insurance type (relative to commercial insurance: Medicare [OR, 1.38; 95% CI, 1.19-1.60] and Medicaid [OR, 2.41; 95% CI, 2.23-2.60]).
Multivariate Analysis of Predictive Factors for ED Utilization a

a Bold values indicate statistical significance (P < .05). ECI, Elixhauser comorbidity index; ED emergency department; OR, odds ratio. Dashes indicate not applicable.
Reasons for Postoperative ED Visits
The reasons for postoperative ED visits after ACLR are shown in Figure 3. In the total 90-day postoperative period, 39.4% of primary diagnoses were found to be related directly to the surgical site, while 60.6% were not related directly to the surgical site. In the first 2 weeks after surgery, 67.5% were related to the surgical site, and 32.5% were not.

Most common primary diagnoses for emergency department (ED) visits within 90 days of anterior cruciate ligament reconstruction (ACLR), categorized by relation to surgical site. CNS, central nervous system.
Of the diagnoses involving the surgical site, pain accounted for 66% (29% of all primary diagnoses for returning to the ED, related to surgical site or not); swelling/effusion, for 9% (4%); infection, for 9% (4%); and wound dehiscence/bleeding, for 6% (3%).
Of the diagnoses that did not involve the surgical site, CNS/psychiatric accounted for 22% (13% of all primary diagnoses for returning to the ED, related to surgical site or not); cardiovascular, for 20% (11%); gastrointestinal, for 20% (11%); infection outside the surgical site, for 18% (10%); other musculoskeletal, for 8% (4%); respiratory, for 6% (3%); and genitourinary, for 5% (3%).
Discussion
ACLR is a common orthopaedic procedure; thus, improvement in perioperative care should enhance the patient experience, improve outcomes, and lower costs. 8,12,23 Despite the prevalence of ACLR, postoperative ED visits remain relatively understudied. The current investigation addresses this by shedding light on postoperative ED utilization, predictors, and reasons.
Of all patients with ACLR, 8.3% visited the ED at least once in the 90 days after their surgery. A study from 2018 found that 3.5% of patients visited the ED within 30 days of ACLR, which is slightly lower than our 30-day finding of about 5.5%. 18 In addition, in our study, only 0.7% of patients were readmitted within 90 days of surgery, which is similar to the finding of 1.2% in another study of ACLR. 2 This gap between ED visits and readmissions highlights the need to consider ED utilization in addition to readmissions.
The greatest incidence of post-ACLR ED visits occurred in postoperative weeks 1 and 2, with 3.0% and 1.3% of all studied patients visiting the ED, respectively. After the second week, the number of weekly visits plateaued. Between weeks 3 and 13, 0.56% to 0.72% of patients visited the ED in each week. To gain insight into this plateaued incidence of ED visits, postoperative weeks 52 to 56 were assessed and noted to have weekly postoperative ED visits for 0.63% to 0.73% of patients. Because these ranges are similar, this indicates that patients returned to a near-baseline rate of visiting the ED by week 3, suggesting that preventive measures should focus on the first 2 weeks after surgery.
To further guide preventive measures for post-ACLR ED visits, we assessed predictors of such visits. Patients with more comorbidities (measured via the ECI) were more likely to visit the ED (for each 2-point increase in ECI score: OR, 2.24). This finding intuitively makes sense and is in line with a previous study that found medical comorbidities to be associated with higher odds of ED utilization after total joint arthroplasties. 7 Similar results have also been reported after outpatient hand surgery. 28
The current study also found insurance coverage to correlate with return to the ED after ACLR. Relative to those with commercial insurance, those with Medicare (OR, 1.38) and those with Medicaid (OR, 2.41) were more likely to visit the ED. Again, these findings are consistent with the literature. A previous overview study found that patients with Medicaid coverage are 4 times more likely to visit the ED than are those with commercial insurance. 14,20,26 This association is probably multifactorial but has previously been suggested to be correlated with other socioeconomic factors. 32,33 One possible explanation is that patients with Medicaid use the ED due to difficulty accessing other medical providers such as primary care physicians and physical therapists. 20,26 The increased odds of ED use with Medicare coverage are probably multifactorial as well. A plausible explanation may involve the finding that less healthy patients were more likely to visit the ED. Most patients with Medicare are older, which tends to increase comorbidity burden. Our ACLR cohort was relatively young, so some patients with Medicare may have access to it due to disabilities rather than age, which could also be associated with greater comorbidity. Generally worse health could partially explain the greater odds of ED utilization for patients with Medicare.
Age and regional differences in post-ACLR ED utilization were noted. In our cohort, younger patients were more likely to visit the ED, which was also found in a previous study of general ED utilization. 14 Perhaps younger patients have a lower threshold for seeking treatment for issues such as surgical-site pain because they are less accustomed to living with pain and other comorbidities. Another study showed that postoperative ED visits for pain were more common among younger patients. 24 Parents may also play an important role in bringing younger patients to the ED for postoperative issues more frequently. Although regional differences cannot be fully explained, geographic variation in barriers to care, such as distance from hospitals and access to primary care providers, and attitudes regarding ED utilization or pain management may contribute.
Finally, the reasons for ED visits after ACLR were assessed. Interestingly, over half (60.6%) of the 90-day ED visits were not related directly to the surgical site. To further investigate this finding, we assessed the reasons for ED visits in the first 2 weeks (during the greatest spike in visits). In the first 2 postoperative weeks, 67.5% of ED visits were related to the surgical site, indicating that surgical-site issues are most prominent in the first weeks. In subsequent weeks, however, other body systems may require additional attention, and medical follow-up may be helpful when indicated.
For the ED visits related to the surgical site, pain was the clear predominant factor, accounting for 66% of diagnoses related to the surgical site and 29% of all ED primary diagnoses. Menendez and Ring 21 similarly found pain to be the most common reason for ED visits after hand surgery. In the era of attempting to limit narcotics, finding the balance of limiting postoperative medications while achieving adequate pain control is clearly a priority. Alternative methods of pain control such as nerve blocks, which have been shown to reduce opioid usage after surgery, could play an important role in reducing postoperative ED visits. 6
The defined reasons and predictive factors for visiting the ED in the 90 days after ACLR should help guide quality improvement programs and optimize patient care. Strong predictive factors, such as Medicaid insurance coverage, large comorbidity burden, and younger age, could be used to quantify patient-level risk of ED use, as previously described for readmission prediction after joint replacement by Boraiah et al. 4 Patients at high risk of ED utilization could be preemptively directed into integrated care pathways designed to address concerns in an outpatient, non-ED setting to avoid high costs associated with ED visits. 16,25 Ideally, patients would present to providers they know, such as the operating surgeon or their primary care provider. Finally, in our cohort, nearly one-third of ED visits were related to pain at the surgical site. Additional counseling regarding expected pain and options for pain management could reduce postoperative ED utilization. Taken together, the present findings highlight risk factors for ED utilization after ACLR and suggest avenues to mitigate the burden associated with this care.
Limitations
There were limitations to this study. As a retrospective database study, the results depended on the accuracy of documentation with diagnostic and procedural coding, presenting a possible source of error. ED visits themselves are relatively dichotomous (happened or not) and should be reflected well in an administrative data set such as PearlDiver. However, the database’s research interface limits observation-level data exportation, which precludes the investigation of specific information about causes and presentations of complications. We therefore designed our statistical analyses to be run directly using the PearlDiver platform, which limited our specification of regression models. We extracted information about individual ED encounters based on primary diagnosis codes ascribed to the claim. While this approach limited the degree to which we could analyze each encounter, it allowed us to examine trends in national utilization that would otherwise not be possible. The current study also did not include cost analysis, analysis of reasons for readmission compared with ED use, or information about the effects of ACLR with concomitant procedures (eg, meniscal repair, posterior cruciate ligament reconstruction, lateral collateral ligament reconstruction). Regarding concomitant procedures, ad hoc analysis showed that patients with and without concomitant procedures had similar rates of ED utilization after ACLR.
Conclusion
Overall, the current study found that after ACLR, >8% of patients visited the ED at least once and 0.7% were readmitted. The greatest incidence of ED visits was in the first 2 postoperative weeks, with a rapid return to baseline afterward. During the first 2 weeks, two-thirds of visits were related to the surgical site. Patient characteristics associated with greater odds of ED utilization were younger age, female sex, greater ECI, certain geographic regions, and Medicaid or Medicare insurance. Because the study cohort was large and consisted of patients of both sexes, from different regions of the country, and with a reasonable distribution of insurance types, we believe the results of this study to be generalizable.
Footnotes
Final revision submitted December 7, 2021; accepted December 15, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.J.M. has received speaking fees and consulting fees from Smith & Nephew. J.N.G. has received consulting fees from Bioventus, Convatec, and Stryker and is the editor-in-chief for the North American Spine Society Journal. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the Yale Human Research Protection Program.