
Abstract
Objectives:
High tibial osteotomy (HTO) is a well-established procedure for addressing varus deformity of the knee or offloading the medial compartment in cases of medial compartment osteoarthritis. Altering the weightbearing axis of the tibia through HTO may result in unintended changes to the posterior tibial slope (PTS) and thus the sagittal stability of the knee. In 2003, Lobenhoffer described a biplanar “L” shaped HTO with an ascending cut in the coronal plane, leaving the tibial tubercle on the distal side of the osteotomy. Since then, multiple techniques have been described, including an “Inverse L”, leaving the tibial tubercle on the proximal end of the osteotomy. We present a modified “flex” version to the plate fixation used in the “L” and “Inverse L” technique with the goal of minimizing changes in the PTS during HTO. To quantify the effect of osteotomy technique on PTS, “L” (n=5), “Inverse L” (n=5), “L with flex” (n=6), and “Inverse L with flex” (n=6) techniques were performed on cadaveric specimens following medial opening wedge HTO (Figure1). Pre- and post-osteotomy fluoroscopic images were taken and PTS measured to determine whether one technique was more effective at minimizing PTS change after medial HTO.
Methods:
The tibia from 22 fresh frozen cadaveric male specimen (11 pairs, mean age 46
Results:
PTS as measured by reviewers before and after HTO using the “circle method” and the motion capture analysis of the change in orientation of the tibial plateau are reported in Table 1. For all specimens, the posterior tibial slope decreased by 1.77 degrees (+/- 3.2). There was no statistically significant difference in change of tibial slope amongst all techniques, measured by lateral radiographs or motion capture analysis.
Conclusions:
There was no statistical difference in the change in posterior tibial slope across treatment types. Reviewer calculations of tibial slope using the circle technique was not different from measures observed through high resolution motion capture. No difference in the change in PTS may allow surgeons to select the technique that they feel most comfortable using on their patient with less concern of causing changes in the PTS and sagittal instability during an HTO. Additionally, this may allow for versatility in the event that patient anatomical characteristics interfere or impede the use of a specific technique. Future studies incorporating pre- and post-CT data to quantify hinge fracture and further characterize slope are underway.

Techniques used for fixation after medial opening wedge HTO. A) "L" B) "Inverse L" C) "L with Flex" D) "Inverse L with Flex" The green line describes the direction of the coronal cut defining the regular L from Inverse L technique.
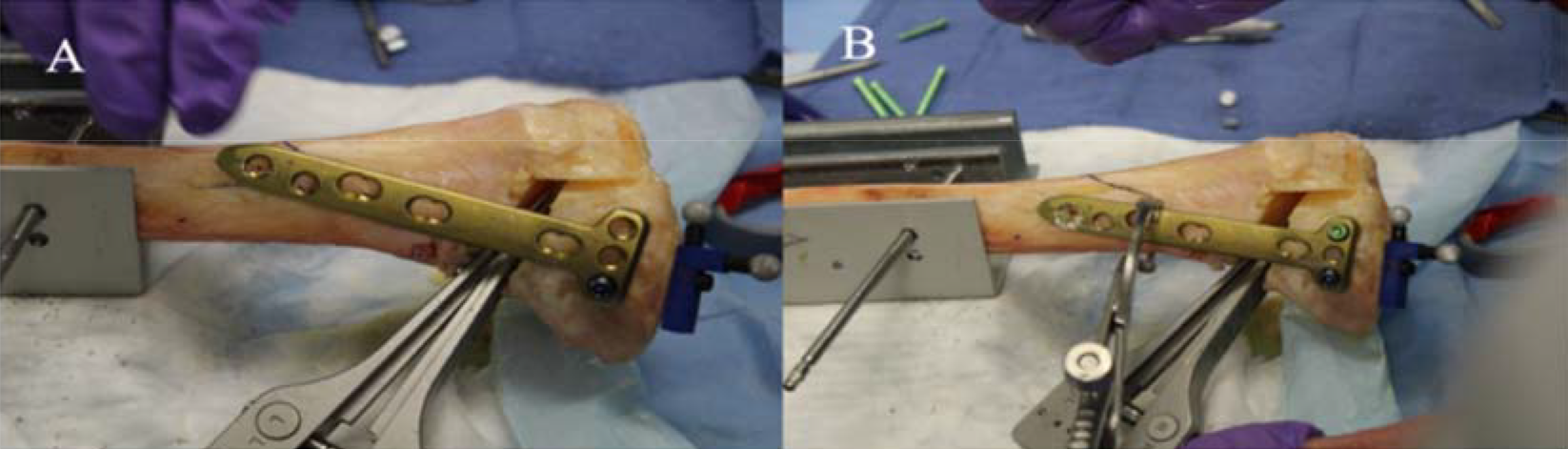
"Flex" technique for maintaining posterior tibial slope in medial opening wedge high tibial osteotomy. Following osteotomy, the plate is secured proximal with the distal end purposefully positioned anterior along the tibial cortex (A). The plate is then reduced to the tibial shaft and secured, with obligatory asymmetric posterior gap relative to the anterior gap (B).
PTS angles pre- and post-HTO as measured by three independent reviewers. The table includes the change in slope as calculated from reviewer measures and the OptiTrack motion capture system. All angles are in degrees.
