
Abstract
Background:
Sleep disturbances are common following concussion and may affect symptom severity and recovery timing. Whether post-concussion sleep problems are associated with functional outcomes, such as postural stability, remains unexplored.
Hypothesis/Purpose:
We examined the association of self-reported sleep problems with clinical measures of postural stability, persistent post-concussion symptoms (PPCS), and symptom severity following pediatric concussion. We hypothesized that patients reporting post-concussion sleep problems would demonstrate worse postural stability, more severe symptoms at their initial clinical visit, and slower symptom recovery times than those without sleep problems.
Methods:
We retrospectively examined data from patients (6-18 years) evaluated by a sports medicine physician ≤21 days post-concussion. Patients performed the modified Balance Error Scoring System (mBESS) and single- and dual-task tandem gait (TG). They also reported initial concussion symptom severity they recalled within the first 24 hours post-injury and current symptoms at the first clinical visit using the Health and Behavior Inventory (HBI). Symptom duration was the number of days post-injury until the patient reported a return to baseline status. PPCS was defined as a symptom duration >28 days post-injury. We stratified patients based on those that self-reported sleep problems since injury (n=97, 14.32.9 years; 49% female; initial visit 10.25.8 days post-injury) compared to those who did not (n=110, 14.32.4 years; 46% female; initial visit 9.35.4 days post-injury) assessed with a yes/no question. Groups were compared using independent sample t-tests, Mann Whitney U tests, or Chi square analyses evaluated at a significance level of p=0.05. We examined PPCS development between groups using a logistic regression analysis adjusted for time of initial visit. Symptom severity was analyzed using a 2x2 repeated measures ANOVA with pairwise follow-up using an adjusted significance level of p=0.025.
Results:
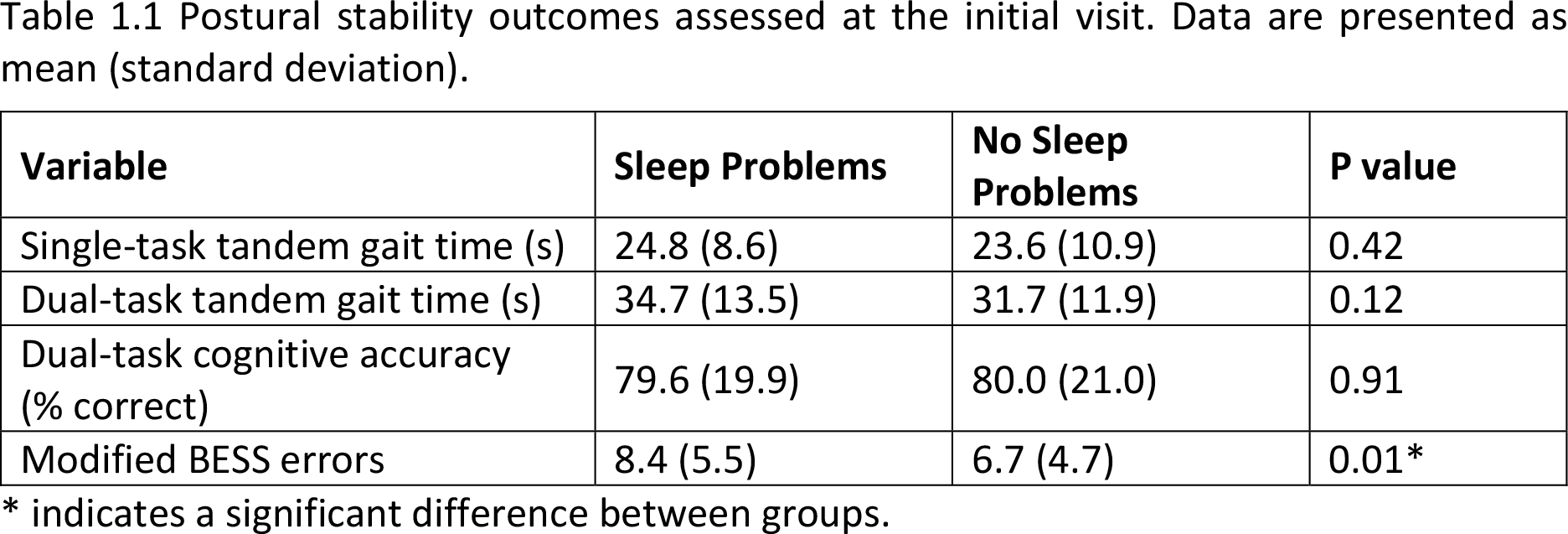
Patients reporting sleep problems post-concussion had significantly more mBESS errors than those without (Table 1). We observed no between-group differences for single- or dual-task TG time or dual-task cognitive performance. Sleep problems post-concussion were associated with more severe symptoms during the first clinical visit despite similar day-of-injury symptoms (Figure 1), and a 2x greater odds of developing PPCS (adjusted odds ratio=2.02, 95% confidence interval = 1.01, 4.06; p=0.049).
Conclusion:
Youth athletes who reported sleep problems post-concussion demonstrated worse balance on the mBESS, increased likelihood of developing PPCS, and more severe symptoms than those who did not. Identifying sleep problems early in concussion recovery may allow clinicians to implement targeted treatment recommendations to improve sleep, and potentially reduce incidence of PPCS.
Postural stability outcomes assessed at the initial visit. Data are presented as mean (standard deviation).

Symptom severity profiles for groups with and without sleep problems. Violin plots describe the probability density of measurements. Data are presented as the median (center dot, with corresponding number included) and interquartile range (box around the median). The retrospective rating of symptom severity at the time of concussion was not significantly different after making Bonferroni adjustment (p=0.03; where we defined statistical significance as p<0.025 due to multiple comparisons: the two time points where outcomes were compared). The sleep problem group, however, had significantly worse symptoms than the no sleep problem group at the time of initial clinical visit.