
Abstract
Background:
At 1 year after anterior cruciate ligament reconstruction (ACLR), two-thirds of patients manage to return to sports (copers), whereas one-third of patients do not return to sports (noncopers). Copers and noncopers have different muscle activation patterns, and noncopers may not be able to control dynamic anterior tibial translation (ATTd) as well as copers.
Purpose/Hypothesis:
To investigate whether (1) there is a positive correlation between passive ATT (ATTp; ie, general joint laxity) and ATTd during jump landing, (2) whether ATTd is moderated by muscle activating patterns, and (3) whether there is a difference in moderating ATTd between copers and noncopers. We hypothesized that patients who have undergone ACLR compensate for ATTd by developing muscle strategies that are more effective in copers compared with noncopers.
Study Design:
Controlled laboratory study.
Methods:
A total of 40 patients who underwent unilateral ACLR performed 10 single-leg hops for distance with both legs. Lower body kinematic and kinetic data were measured using a motion-capture system, and ATTd was determined with an embedded method. Muscle activity was measured using electromyographic signals. Bilateral ATTp was measured using a KT-1000 arthrometer. In addition, the Beighton score was obtained.
Results:
There was no significant correlation between ATTp and ATTd in copers; however, there was a positive correlation between ATTp and ATTd in the operated knee of noncopers. There was a positive correlation between the Beighton score and ATTp as well as between the Beighton score and ATTd in both copers and noncopers in the operated knee. Copers showed a negative correlation between ATTd and gastrocnemius activity in their operated leg during landing. Noncopers showed a positive correlation between ATTd and knee flexion moment in their operated knee during landing.
Conclusion:
Copers used increased gastrocnemius activity to reduce ATTd, whereas noncopers moderated ATTd by generating a smaller knee flexion moment.
Clinical Relevance:
This study showed that copers used different landing techniques than noncopers. Patients who returned to sports after ACLR had sufficient plantar flexor activation to limit ATTd.
An anterior cruciate ligament (ACL) injury leads to greater knee laxity and alterations of muscle activation patterns. 1,4,20 ACL reconstruction (ACLR) reduces knee laxity. 24 At 1 year after ACLR, however, 82% of patients return to any sports, while only 62% are able to return to their preinjury level of sports, and only 44% manage to return to competitive sports. 6 The discrepancy between returning to any type of sports and returning to preinjury levels of sports may be caused by learned muscle control or adjustments of kinematics. Some patients are not able to control dynamic knee laxity (that is, anterior tibial translation [ATT]) during landing after ACLR, whereas others are.
There is no association between passive ATT (ATTp; such as during a Lachman test or KT-1000 arthrometer assessment) and dynamic ATT (ATTd; such as during normal gait, active extension, heel raises, cycling, single-leg squats, and chair squats) for ACL-deficient, ACL-reconstructed, or healthy knees. 27,41 One previous study even found that healthy participants with a large ATTp showed a small ATTd. 23 These findings suggest that next to the passive resisting force of the ACL and knee ligament properties, other factors, including dynamic muscle activation patterns or landing kinematics and kinetics, are involved for controlling ATTd. 23 One possibility is that patients undergoing ACLR who manage to return to their preinjury sports type and level (copers) are able to use muscle activation patterns that limit the strain of the ACL, whereas patients undergoing ACLR who do not manage to return to their preinjury sports (noncopers) rely more on the resisting force from the ACL. Studies have found that noncopers have different dynamic muscle activation patterns than copers during a single-leg stance on a stabilization platform 13 and a hop test. 18
In line with the suggestion that knee laxity can be mitigated by muscle-activation patterns in a dynamic situation, it has been reported that ACL-injured patients with low muscle strength of the quadriceps or large interleg hamstring muscle strength asymmetry show greater movement asymmetry in the sagittal plane. 1,31 This may be caused by an imbalance of the quadriceps-to-hamstring ratio, which may result in modified kinematics, kinetics, and ATTd. 2,39 It has also been found that residual muscle activity of the medial gastrocnemius and hamstring modulates ATTp. 8,26 Fleming et al 19 found that medial gastrocnemius activity increases ATTp, and computer models have shown that hamstring activity reduces ATTd during gait. 37
As far as we know, no research has been conducted to study in vivo the relationship between ATTd and muscle-activation patterns. This may be of interest for patients after ACLR, as copers may have a solution to limit knee ATTd that noncopers do not have but may be able to learn. The aims of this study were therefore to investigate whether (1) there is a relationship between ATTp (ie, general joint laxity [Beighton score]) and ATTd during jump landing, (2) whether ATTd can be moderated by muscle-activation patterns during a single-leg hop for distance (SLHD), and (3) whether there is a difference in ATTd between copers and noncopers. We hypothesized that copers compensate for knee laxity in dynamic situations by developing effective muscle-activation strategies, whereas noncopers are not able to actively moderate knee laxity.
Methods
The study was a collaboration between the Martini Hospital’s Department of Orthopedic Surgery and the University Medical Center Groningen’s Department of Rehabilitation Medicine and was conducted between April 2018 and November 2019. The study design, procedure, and protocol were approved by a medical ethics committee, and all participants provided informed consent.
Participants
The correlation between ATTd and ATTp was used for an a priori power analysis 14 (R 2 = 0.47). Based on an effect size of 0.69, alpha of ≤.05, and power of 80% to detect statistically significant differences, 12 participants were needed. We included 40 patients (15 women and 25 men; age range, 18-42 years). Inclusion criteria were patients who were followed up 12 to 24 months after ACLR and had undergone ACLR using hamstring tendon autografts. Exclusion criteria were patients with cartilage abnormalities that needed concomitant surgical treatment, those who underwent revision ACLR, those who underwent osteotomy, or those with contralateral ACL injuries.
ACLR for all patients was performed with an ipsilateral gracilis and semitendinosus tendon autograft, which was fixed using an endobutton (Endobutton CL Ultra; Smith & Nephew) in the femoral socket. For graft fixation in the tibial tunnel, a screw and sheath of polyether ether ketone (PEEK) material were used. This sheath has 4 wings that separate and compress graft strands against the bone tunnel as the PEEK screw is fixed into the sheath.
Study Parameters
The primary outcome measures were ATTd during an SLHD, 45 ATTp measured using a KT-1000 arthrometer (MEDmetric), and muscle-activation patterns during both ATTd and ATTp measurements for both the operated and contralateral legs. The coefficient of variation for this procedure for determining ATTd across 16 healthy knees was 5.2% ± 1.2%, and excellent reproducibility was observed (intraclass correlation coefficient [ICC] (3,1) = 0.92). 14 Moreover, Keizer and Otten 25 showed that ATTd >2.32 mm is reliable in terms of wobbling masses and the Vicon position error. Previous studies have found a smaller variability with the KT-1000 arthrometer compared with other devices to measure ATTp. 38 The mean variability of the KT-1000 arthrometer has been reported as 1.8 mm (interrater ICC = 0.79). 13
The secondary study parameters during the SLHD were the knee flexion angle, external knee flexion moment, and vertical ground-reaction force in both the operated and the contralateral legs. The Beighton score (range, 0-9 points), 11 a scoring system for joint laxity and hypermobility, was also used as a secondary study parameter.
Procedure
Each participant was measured in a single session. Participants completed a questionnaire about sports participation and anxiety (see Appendix), and the Beighton score was calculated. The questionnaire was then used to categorize patients as copers (those who are returned to their preinjury type of sports) or noncopers (those who did not return to their preinjury type of sports) for the subsequent data analysis. After this, ATTp (KT-1000 arthrometer; condition 1) and ATTd (SLHD test; condition 2) were calculated. The order of the conditions was randomized to reduce the effect of fatigue on knee laxity. 9
Surface electromyographic (EMG) electrodes (Wave Plus wireless EMG system; Cometa Systems) were attached according to SENIAM (surface EMG for noninvasive assessment of muscles) guidelines. 32 For condition 2, we recorded the EMG signals for the medial hamstring, lateral hamstring, rectus femoris, vastus medialis, vastus lateralis, gastrocnemius medialis, and gastrocnemius lateralis. For condition 1, the EMG signals were recorded for the medial hamstring, lateral hamstring, rectus femoris, vastus medialis, and vastus lateralis. Gastrocnemius activity was not measured in condition 1 because the location of the EMG electrodes interfered with the attachment of the KT-1000 arthrometer. The same researcher (M.N.J.K.) placed all the electrodes.
During condition 1 (passive test), ATTp was measured using a KT-1000 arthrometer with the knee at 30° of flexion under a force of 67, 89, and 133 N. 33 The participants lay supine and were instructed to relax their leg, which was verified by observing the surface EMG recordings. This test was repeated 3 times for both legs.
During condition 2 (dynamic test), 10 SLHDs were performed on both the operated and contralateral legs, and ATTd, muscle activation patterns, knee flexion angle, and external knee flexion moment were determined. Using a 10-camera, 3-dimensional (3D) motion capture system (Vero; Vicon), 3D marker positions were measured at a frequency of 200 Hz. Markers were attached as adapted from Boeth et al 14 (Figure 1). Markers were placed by the same researcher (M.N.J.K.) for each participant. After attaching the markers, calibration frames of a flexion-extension movement and a star-arc movement, as prescribed by the manufacturer’s instructions, were taken to be able to identify the hip and knee joint centers and axis of rotation of the knees. 16,17 See Keizer and Otten 25 for details on the entire procedure.

Marker placement. Markers were attached on the right and left anterior and posterior superior iliac spines, the right and left iliac crests, the greater trochanter, the medial and lateral epicondyles of the femur, the medial and lateral malleoli of the ankle, the heel, anterior of the talus bone, and the first and fifth metatarsophalangeal joints. Also, 2 additional markers were attached to the pelvis and 2 to the thigh, and 6 additional markers were attached to the shank. 14
The participants subsequently performed 3 practice SLHDs with both legs, starting with the uninjured leg. The participants started by standing still on their tested leg and hopped forward as far as possible. Participants were instructed to stand still for at least 3 seconds after landing to ensure a controlled landing. For each leg, the median of the distance of the 3 practice jumps was used for the starting distance from the middle of a 40 × 60–cm force platform (AMTI). Overall, 10 successful jumps were recorded with both legs. The starting leg was randomized.
Data Analysis
Data were processed and analyzed using the Statistics Toolbox in MATLAB (Version 9.7; MathWorks). All kinematic and kinetic data and muscle activity during each jump were determined between 1 second before and 1.5 seconds after initial contact (IC), defined as the moment at which the vertical ground-reaction force was >5% of the body weight. The zero point of ATTd was calibrated using the frames captured during a flexion-extension task. Raw 3D marker position data were filtered using a low-pass frequency convolution filter of 10 Hz with zero lag. Gaps smaller than 20 frames were filled using quadratic spline interpolation with zero lag. Trials with larger gaps were excluded.
The knee flexion moment was calculated from the ground-reaction force vector and its lever arm to the center of the knee of the stance leg. For the quantification of ATTd and knee angles, 2 coordinate systems were reconstructed in the tested knee using a customized MATLAB script based on the method of Boeth et al. 14 One system was reconstructed in the femoral segment (parent system) and 1 in the tibial segment (child system). See Keizer and Otten 25 for the details of this procedure. The motion of each coordinate system was consistent with the movement of the respective segment. ATTd was quantified in millimeters using the relative movement of the origin of the coordinate system of the tibia relative to that of the femoral coordinate system. The knee flexion angles and rotations between both coordinate systems (tibial and femoral) were calculated. Rotations were obtained using scalar products as in the equations by Robertson et al. 35
The surface EMG signals were recorded at a sampling frequency of 1000 Hz. Muscle activity around the point of first ground contact, taking into account an electromechanical delay of 49.7 milliseconds, 10 was rectified and filtered using a fourth-order, low-pass frequency Butterworth filter at 6 Hz with zero lag. To minimize the influence of body fat and skin conductivity, we scaled the EMG signals to the mean muscle activity from 1 second before IC to 1.5 seconds after IC of the SLHD for each participant. Because of large variations in peak activation between and within participants, especially of the semitendinosus muscle, during a maximal isometric contraction task, we did not scale to this muscle activity. Maximal isometric contraction tasks are notorious for these kinds of large variations. The mean of the kinematic data, kinetic data, and muscle activation patterns of the 10 trials represented the movement pattern of the participants.
Statistical Analysis
The subsequent statistical analyses were performed on the means of the 10 trials of each participant. The Pearson correlation was calculated between ATTp of the operated leg and the Beighton score, and a statistical parametric mapping (SPM) regression analysis was performed to analyze the relation between ATTd of the operated leg over time and the Beighton score. Pearson correlations were calculated between maximal ATTd and ATTp for the operated and contralateral legs in copers and noncopers separately.
To analyze the EMG signals over time, we used an SPM canonical correlation analysis (CCA) to find the significance between muscle activity and ATTd and between muscle activity and kinetics. SPM{χ2} analyses were performed using the open-source spm1d code (V.M.0.1; www.spm1d.org) in MATLAB (Version 9.7). For this, data from IC to 0.5 seconds after IC were used. The dependent variable was ATTd, and the independent variables were the activity of the independent muscles, knee flexion angle, and external knee flexion moment over time. When the original SPM{χ2} analysis exceeded the calculated critical chi-square value (threshold) based on an alpha of ≤.05, the null hypothesis was rejected, implying a correlation. When significant values were reached, a post hoc regression analysis was performed for each independent muscle activity and kinetic variables as independent variables. This procedure was performed for the whole cohort, for only the copers, and for only the noncopers.
P values were considered to be significant with an alpha of ≤.05. If a correlation was significant, a correlation coefficient of 0.20-0.49, 0.50-0.79, and 0.80-1.00 were considered to represent a weak, moderate, and strong association, respectively. 15
Results
The baseline characteristics of the study participants are displayed in Table 1. Figure 2 shows the results between copers and noncopers of the kinetic and kinematic data over the 10 trials in the operated leg, and Figure 3 shows similar data for the contralateral leg.
Baseline Characteristics a
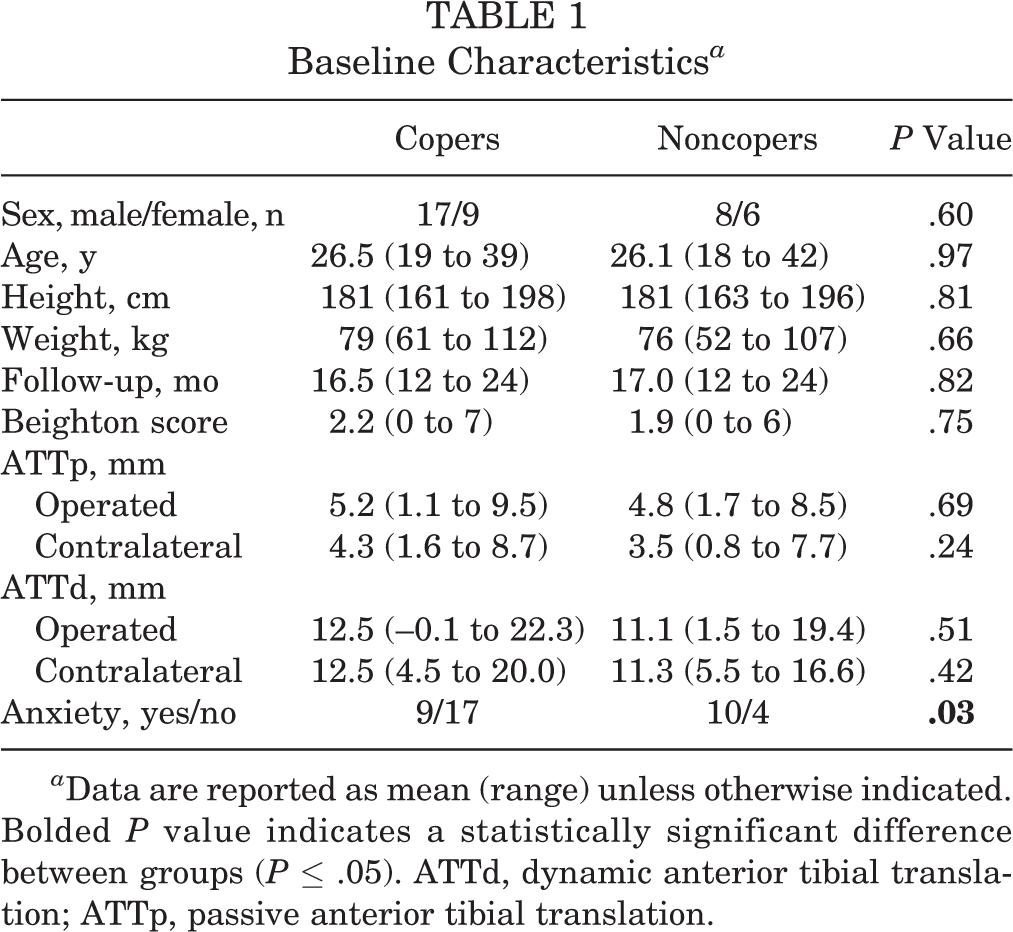
a Data are reported as mean (range) unless otherwise indicated. Bolded P value indicates a statistically significant difference between groups (P ≤ .05). ATTd, dynamic anterior tibial translation; ATTp, passive anterior tibial translation.
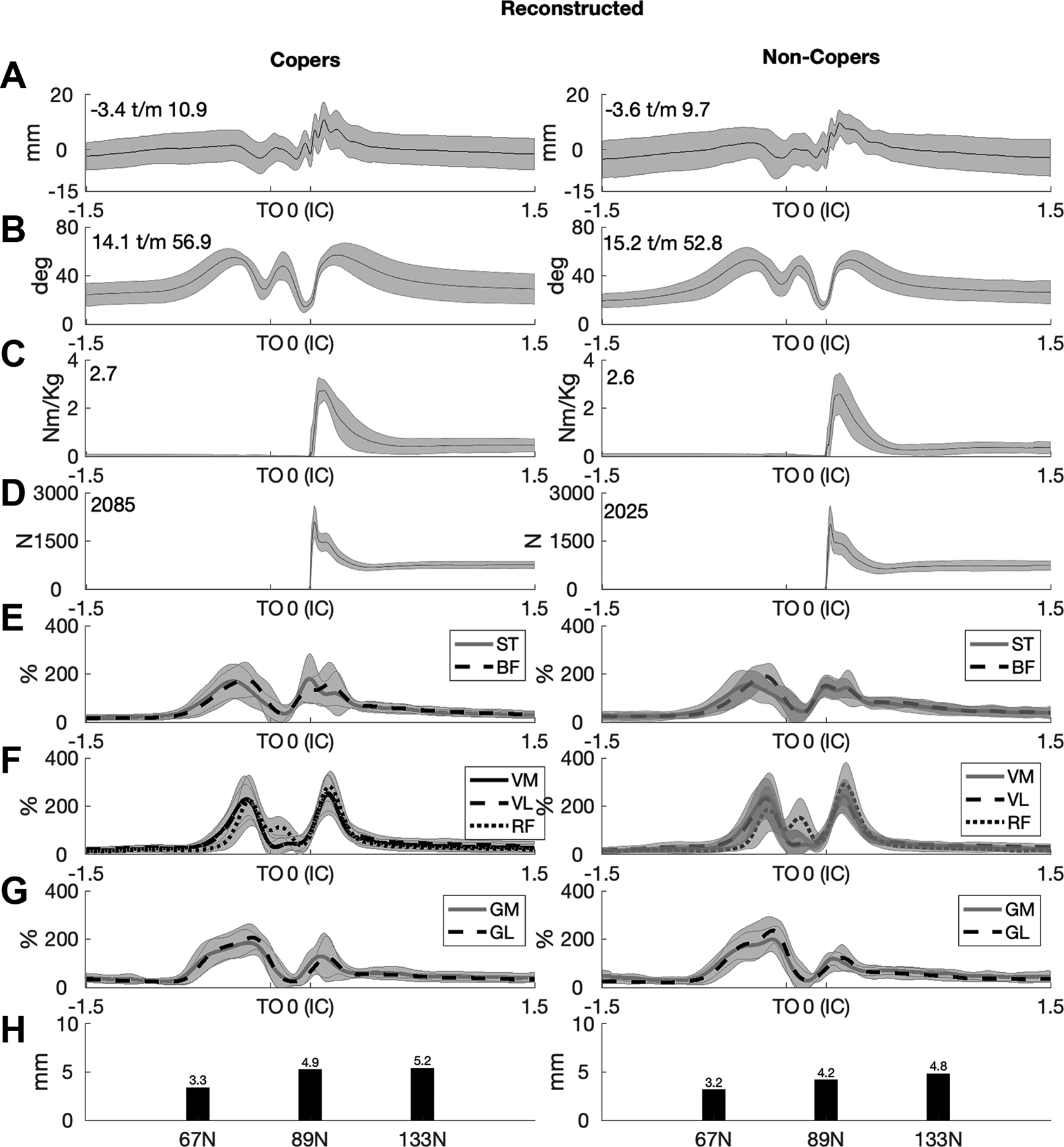
Mean results for the operated leg of copers and noncopers for (A) dynamic anterior tibial translation (ATT), (B) knee flexion angle, (C) external knee flexion moment, and (D) vertical ground-reaction force. Muscle activity expressed as a percentage of mean electromyographic signals for (E) medial (ST) and lateral (BF) hamstrings; (F) vastus medialis (VM), vastus lateralis (VL), and rectus femoris (RF); (G) gastrocnemius medialis (GM) and gastrocnemius lateralis (GL); and (H) passive ATT. Gray areas indicate SDs. IC, initial contact.

Mean results for the contralateral leg of copers and noncopers for (A) dynamic anterior tibial translation (ATT), (B) knee flexion angle, (C) external knee flexion moment, and (D) vertical ground-reaction force. Muscle activity expressed as a percentage of mean electromyographic signals for (E) medial (ST) and lateral (BF) hamstrings; (F) vastus medialis (VM), vastus lateralis (VL), and rectus femoris (RF); (G) gastrocnemius medialis (GM) and gastrocnemius lateralis (GL); and (H) passive ATT. Gray areas indicate SDs. IC, initial contact.
General Joint Laxity and ATT
There was a weak but significant positive correlation between the Beighton score and ATTp of the operated leg (r = 0.42; P = .007). The SPM{t} regression analysis (Figure 4) showed a significant positive correlation between the Beighton score and ATTd of the operated leg between 0.08 and 0.19 seconds before IC (P = .003).
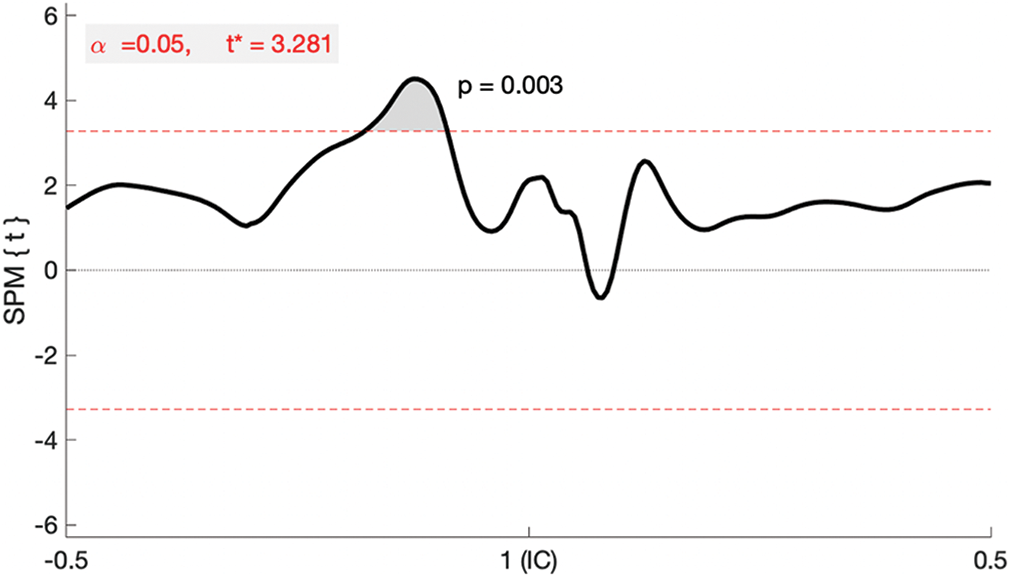
SPM{t} regression analysis between the Beighton score and dynamic anterior tibial translation (ATTd). IC, initial contact; SPM, statistical parametric mapping.
ATT of Copers Versus Noncopers
There was no significant correlation between ATTp and maximal ATTd of the operated leg for copers (r = 0.05; P = .82), and there was a moderate significant positive correlation for noncopers (r = 0.55; P = .04). There was no statistically significant difference between ATTp and maximal ATTd for copers or noncopers in the contralateral knee (r = 0.05, P = .82; and r = 0.38, P = .18, respectively).
The correlation of ATTp between the operated and contralateral legs was moderately significant for both the copers and noncopers (copers: r = 0.56; P = .003) (noncopers: r = 0.68; P = .008) (Figure 5A). The correlation of ATTd between the operated and contralateral legs was significant but weak for copers (r = 0.39; P = .047) and moderately significant for noncopers (r = 0.76; P = .002) (Figure 5B).

Correlation between the operated and contralateral legs in copers and noncopers for (A) passive anterior tibial translation (ATTp) and (B) maximal dynamic anterior tibial translation (ATTd).
Control of ATTd
Table 2 shows the results of the SPM{χ2} CCA in the operated and contralateral legs for the whole cohort, copers, and noncopers. Also shown are the variables with a significant correlation of ATTd according to the post hoc SPM{t} analysis.
SPM{χ2} CCA and Post Hoc SPM{t} Regression Analysis on Significant Muscle Activity and Knee Joint Kinetics a

a CCA, canonical correlation analysis; IC, initial contact; NS, not significant; SPM, statistical parametric mapping.
b Time frame after IC in which the variable was significant.
c –, negative correlation; +, positive correlation.
d Only the significant variables are shown.
For the whole cohort, the SPM{χ2} CCA of the operated leg showed a significance between 2 and 3 milliseconds after IC (P = .049) and between 11 and 17 milliseconds after IC (P = .028). The post hoc SPM{t} regression analysis showed significant correlations of vastus lateralis, gastrocnemius medialis, and gastrocnemius lateralis muscle activity and knee flexion angle with ATTd over some time points (Table 2).
For copers, the SPM{χ2} CCA of the operated leg showed a significance between 0 and 3 milliseconds after IC (P = .049). The post hoc SPM{t} regression analysis showed significant correlations between gastrocnemius medialis and lateralis muscle activity and ATTd over some time points (Table 2).
For noncopers, the SPM{χ2} CCA showed a significance between 12 and 15 milliseconds after IC (P = .040) in the operated leg and between 4 and 6 milliseconds after IC (P = .049) and between 16 and 19 milliseconds after IC (P = .048) in the contralateral leg. The post hoc SPM{t} regression analysis for the operated leg showed significant correlations between knee flexion moment and ATTd between 13 and 19 milliseconds after IC (Table 2). The post hoc SPM{t} regression analysis for the contralateral leg showed significant correlations between gastrocnemius medialis and lateralis activity and ATTd over some time points (Table 2).
Discussion
This research shows that after ACLR, patients who were able to return to sports and who had larger activation of the gastrocnemius muscles just after IC during a unilateral landing with the operated leg had less ATTd. Moreover, patients who were not able to return to sports had a larger knee flexion moment during a unilateral landing with the operated leg and had greater ATTd. ATTd of the operated knee was less in noncopers who had less ATTp, but there was no significant association present in copers.
Correlation of ATT Between Legs
In the current study, we found a positive association between ATTp of the operated and contralateral leg. We also found a positive association between maximal ATTd of the operated and contralateral leg. This may suggest that surgeons are able to reconstruct the ACL at a comparable length as that of the native ACL in the contralateral knee or that, during rehabilitation, the length of the reconstructed ACL adapts to its use. Miura et al 30 also found that ACLR could reduce knee laxity close to the level of that of the contralateral knee. However, there is also a study that found higher ATTp in the operated leg compared with the contralateral leg. 29
General Joint Laxity and ATT
It has been shown that general joint laxity is associated with a higher risk of ACL injuries and an increased risk of graft failure after ACLR and is more common in patients with an ACL injury. 3,43 We found an association between the Beighton score and ATTp for the entire cohort, showing that patients with larger general joint laxity also had larger amounts of specific ATTp. In addition, our analysis showed that just before a unilateral landing with the operated leg, patients who had a higher Beighton score also had a larger amount of ATTd. These results imply that in passive situations, ATTp (or in dynamic situations with no external forces, ATTd) is associated with general joint laxity. After IC, there was no association between general joint laxity and ATTd for copers or noncopers, and this suggests that during a jump landing, ATTd is limited by joint kinetics and/or muscle activation. In girls with large general joint laxity, a different muscle activation pattern was shown during a static balance task, which supports our suggestion. 21
Relationship Between ATTp and ATTd
Previous studies showed no correlation between ATTp and ATTd during gait, active extension, heel raises, cycling, single-leg squats, and chair squats in ACL-deficient, ACL-reconstructed, and healthy knees. 27,41 One previous study, using the same technique as the present study, showed a weak negative correlation between ATTp and ATTd in healthy participants. 23 Contrarily, the present study showed a positive association between ATTp and ATTd of the operated leg for noncopers but not for copers. This difference may be because of the injury. Noncopers with larger amounts of ATTp also had larger amounts of ATTd during unilateral landing in the operated leg, and this suggests that noncopers rely more on the strain of the ACL during impact than copers. The absence of a significant association in copers supports the hypothesis that those who are able to return to sports are able to control ATTd and develop an effective strategy during their rehabilitation to reduce ATTd during landing. Consequently, copers rely less on the strain of the ACL to limit ATTd. This was also shown in healthy participants who amended their knee flexion moment to reduce their ATTd. 23
In the following subsections, we discuss the underlying mechanisms of how joint kinematics, kinetics, and/or muscle activation can contribute to an effective strategy that reduces ATTd during a unilateral jump landing in patients after ACLR.
Kinematics, Kinetics, and ATTd
We can divide a unilateral jump landing into different phases: preparation, loading response, and stabilization. The preparation phase is during flight, and the knee is extending to prepare for IC. Our analysis showed that during this preparation phase, there were no crucial differences in kinematics, kinetics, or muscle activation between the operated and nonoperated legs and/or between copers and noncopers. The second phase, loading response, is characterized by a rapid knee flexion movement that enables shock absorption and deceleration of the body’s center of mass. We found larger knee flexion angles during the loading response phase and more ATTd. This finding is in line with previous findings in healthy participants using the same measurement methods. 23 Previous cadaveric studies using a strain transducer on the anteromedial bundle of the ACL showed that the ACL is most strained when the knee is flexed between 0° and 30° and that the strain becomes less by larger amounts of knee flexion. 7,34 Similar results were shown in healthy knees using magnetic resonance imaging– and fluoroscopy-based modeled jump landings. 42 These studies showed that when the knee is flexed more than 30°, the ACL is less strained. Consequently, there is more room for ATT, and this is thus in line with our findings on ATTd.
More knee flexion during jump landing results in less strain on the ACL, 7,34 and physical therapists usually instruct their patients to land with a more flexed knee to prevent reruptures. 12,46 However, when the ACL is slack (at high knee flexion angles), greater translational acceleration can occur in the tibia relative to the femur, which subsequently is decelerated by the ACL, resulting in greater peak stress of the ACL in uncontrolled sudden movements. Only the noncopers, with their operated leg, decreased their knee flexion moment and showed less ATTd. A decreased knee flexion moment is possible because of less knee flexion, which limits energy absorption around the knee joint during landing. Future studies should focus on the combination of knee flexion during landing and mechanical properties of the ACL to obtain more insight into the optimal and patient-specific landing technique that lowers the strain on the ACL.
Muscle Activation and ATTd
Gastrocnemius activity limits ATTp, 8,19,26 and we, for the first time, showed that increased gastrocnemius activity also limited ATT during a dynamic hopping task. The reason for this may be the tibial plateau angle, posteriorly lower than anteriorly, 22 which favors ATT. Fleming et al 19 showed that the gastrocnemius is an antagonist for the ACL. This seems contrary to our results. That study measured ACL strain, which is related to ATT, but its authors evoked isolated muscle activity by electrical stimulation, which is different from muscle group activation in the task used in the present study. A future study could investigate the influence of the anatomy of the knee on ATTd. In healthy participants, in contrast with the findings of the present study, there is no significant association between muscle activation and ATTd also during a unilateral jump landing. 23 This difference may be explained by the injury. After ACLR, patients may learn to limit their ATTd in different ways than healthy participants. Another possible explanation is that the significant correlation that we found between gastrocnemius activity and ATTd is caused by the pattern of activation of all muscles together during landing.
Vastus lateralis activity was negatively associated with ATTd. Indeed, patients with greater activation of the vastus lateralis just after IC showed less ATTd. This negative correlation is not expected, as a previous study showed that the quadriceps causes an increase in ACL loading. 44 A previous study in healthy participants also found a negative weight coefficient between the vastus lateralis and ATTd; however, the findings were not statistically significant. 23 Increased vastus activity reduces further knee flexion, and we found that the knee flexion angle was positively correlated with ATTd. The knee flexion angle may make a larger contribution to ATTd than vastus activity, which may explain that at the moment that vastus lateralis activity is increased (and the knee flexion angle is smaller), ATTd is smaller than with less vastus lateralis activity.
Because of the harvest of the medial hamstring tendon, it is a self-evident hypothesis that the activity of the hamstring is reduced, shifting the balance toward the quadriceps. 36 However, we did not find a difference in hamstring activity of the injured leg compared with the uninjured leg. This is in line with a previous study that showed that the medial hamstring tendon regenerates and strength returns. 40 Consequently, harvesting of that tendon may not have been the cause of the observed differences.
Summary of Copers Versus Noncopers
We found that copers and noncopers, in their operated and contralateral legs, showed differences in the association between muscle activity and ATTd and between kinetics and ATTd. Copers increased their gastrocnemius activity to reduce ATTd of the knee in the operated leg. Noncopers amended their knee flexion moment in their operated leg to reduce ATTd. Moreover, in their contralateral leg, noncopers also used muscle activation of the gastrocnemius to reduce ATTd. These results may imply that copers use muscle activation of the gastrocnemius to limit ATTd, whereas noncopers fail to do this. Instead, noncopers limited their knee flexion moment to limit ATTd. Figure 6 summarizes the results of this study. Only the significant variables on ATTd are depicted.

Relationship between significant variables and dynamic anterior tibial translation (ATTd). Dashed line: whole cohort. Dotted line: only the copers. Continuous line: only the noncopers. ATTp, passive anterior tibial translation.
Limitations
A limitation of this study may be that as we have no information on the unstrained length of the ACL, we have no way to determine clinical benchmark values of ATTd in particular patients. A second limitation is that the measured ATTd is influenced by wobbling masses. In another experiment in which we identified the sensitivity of the method used to quantify ATTd on marker placement (wobbling masses) and the Vicon position error, we found an error in the measured ATTd of 2.32 mm. 25 All differences between patients on 1 SLHD of less than 2.32 mm should be interpreted with caution. This limitation is used to interpret the results of the current study. Thereby, previous studies showed comparable ATTd ranges with our study. 5,23,25,28 A third limitation is the method of normalization of muscle activity. We chose to normalize muscle activity to the percentage of the mean muscle activity during the SLHD. This normalized muscle activity might be more comparable between participants than nonnormalized electrical muscle activity because the influence of variables such as conductance and body fat is bypassed. We used muscle activation over a longer time window in the same task for normalization, which forms a background to detect peaks at certain moments in time. Because of large variations in peak activation in maximal isometric contractions between and within patients, especially of the semitendinosus muscle, we did not scale to this muscle activity. Maximal isometric contraction tasks are notorious for these kinds of large variations. Another limitation is that we measured the absolute ATTp using the KT-1000 arthrometer, which may have introduced effects of the weight of the lower legs on ATTp, thus yielding different net loads in different limbs of varying masses. A future study may analyze the effect of lower leg mass using the KT-1000 arthrometer.
Conclusion
The study findings indicated that ATT during a unilateral jump landing was limited by knee flexion moment and gastrocnemius muscle activation but differed between copers and noncopers. Copers used increased gastrocnemius activity to limit ATTd in their operated leg, whereas noncopers limited their knee flexion moment to reduce ATTd.
Footnotes
Final revision submitted October 5, 2020; accepted November 19, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University Medical Center Groningen (reference No. 2017.658).