
Abstract
Background:
Core muscle injury (CMI), often referred to as a sports hernia or athletic pubalgia, is a common cause of groin pain in athletes. Imaging modalities used to assist in the diagnosis of CMI include ultrasound (US) and magnetic resonance imaging (MRI).
Purpose:
To determine if preoperative MRI findings predict clinical outcomes after surgery for CMI.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective cohort study was performed on a consecutive series of patients who were operatively treated for CMI by a single surgeon. CMI was diagnosed based on history, physical examination, and a positive US. In addition, all patients underwent a preoperative MRI. Patients were divided into 2 groups based on whether the MRI was interpreted as positive or negative for CMI. All patients underwent mini-open CMI repair. Patient-reported outcomes (PROs) were collected both pre- and postoperatively and included a visual analog scale (VAS) for pain, the University of California, Los Angeles (UCLA) activity score, and the modified Harris Hip Score.
Results:
A total of 39 hips were included in this study, of which 17 had a positive MRI interpretation for CMI (44%) and 22 had a negative MRI interpretation (56%). Mean age at the time of surgery was 35 years (range, 17-56 years), and mean follow-up was 21 months (range, 12-35 months). No significant difference was found between groups in mean age or time to follow-up. Patients in both groups demonstrated significant improvement from preoperative to most recent follow-up in terms of the UCLA activity score (P < .05). VAS scores significantly improved for patients with a positive MRI interpretation (P = .001) but not for those with a negative MRI interpretation (P = .094). No significant difference on any PROs was found between groups at the most recent follow-up.
Conclusion:
Successful clinical outcomes can be expected in patients undergoing surgery for CMI diagnosed based on history, physical examination, and US. Patients with a preoperative MRI consistent with CMI may experience greater improvement in pain postoperatively, although MRI does not predict postoperative activity level in these patients.
Core muscle injury (CMI) is a common cause of groin pain in athletes characterized by concomitant injury to the insertion of the adductor longus and the rectus abdominis on the pubis. 16,20 Often called a “sports hernia” or athletic pubalgia, these injuries often respond to nonoperative treatment, with CMI repair reserved for patients who do not respond to conservative management. 3,21
The clinical diagnosis of CMI is challenging because of the many potential causes of groin pain in athletes, including CMI, intra-articular hip-related groin pain, and other causes of groin pain. 5,11,20,22,23 History and physical examination, including tests such as the cross-body sit-up test and the presence of an adductor contracture, are important in establishing a diagnosis of CMI. 8 Ultrasound (US) and magnetic resonance imaging (MRI) also serve a role in the diagnosis of a sports hernia. 5,18 The treating surgeon must sometimes make a diagnosis when aspects of the history, physical examination, and imaging do not all coincide with a CMI. 8 Therefore, it is important to continue to research the most critical aspects of the workup in diagnosing a CMI and how these aspects affect patient outcomes. The purpose of this study was to determine if preoperative MRI findings predict clinical outcomes after surgery for CMI. The authors hypothesized that patients with MRI interpreted as positive for CMI would demonstrate improved postoperative clinical outcomes compared with those with a negative MRI interpretation.
Methods
Patient Selection
After institutional review board approval, we performed a retrospective analysis of prospectively collected data on CMI patients. A single, sports-medicine fellowship-trained orthopaedic surgeon’s
Rehabilitation Protocol
All patients were instructed to avoid trunk/hip hyperextension, rectus abdominis contractions, heavy lifting, and any activities that increase abdominal pressure for the first 2 weeks postoperatively. During this time, the goals were to gradually restore range of motion (ROM) and flexibility with gentle stretching exercises, hip active/passive ROM, and treadmill walking. Plank progression was started in weeks 3-4, along with jogging, more aggressive stretching, leg presses, and single-leg activities. Light, sport-specific activities were initiated in weeks 4-5 followed by planting/pivoting in weeks 5-6. Criteria for return to competition for athletes included full and pain-free ROM, hip strength equal to the contralateral side, and the ability to perform sport-specific drills without pain.
Physical Examination
All patients who presented with symptoms consistent with CMI underwent a thorough physical examination. To narrow the differential diagnoses, the hip, pelvic, groin, and thigh region were assessed. Among CMI patients, point tenderness was often localized about the pubic symphysis, lower rectus abdominis musculature, anteromedial thigh, external ring of the inguinal canal, and pubic tubercle. In patients with a history and initial physical examination consistent with CMI, 4 additional tests were routinely performed: (1) the cross-body sit-up test, (2) pain with straight-leg sit-up, (3) external rotation Stinchfield test, and (4) the presence of an adductor contracture. 8 Other tests, including the impingement test (flexion, adduction, and internal rotation), were performed to assess for femoroacetabular impingement (FAI). Patients were treated with concomitant CMI repair and arthroscopic labral repair/femoroplasty under the same anesthetic in patients with a positive impingement test, less than 10° of internal rotation, and labral tears on MRI and radiographs consistent with hip impingement. In these cases, repair of the CMI was performed first, after which the patient was redraped and the hip arthroscopy procedure performed.
Imaging Protocol
Each patient underwent an ultrasonogram by a fellowship-trained, board-certified sports medicine specialist. US was considered positive for CMI if hypoechoic areas along the distal rectus insertion and the proximal adductor longus tendon were observed on transverse and linear views, as previously described (Figure 1). 8 In addition, each patient underwent an MRI survey of the pelvis without contrast. The sports hernia MRI protocol at our institution consists of coronal short tau inversion recovery (STIR) and T1 large field-of-view (FOV) (38 cm) sequences and axial T2 fat-saturation, coronal proton density, and sagittal STIR small FOV (24 cm) sequences.
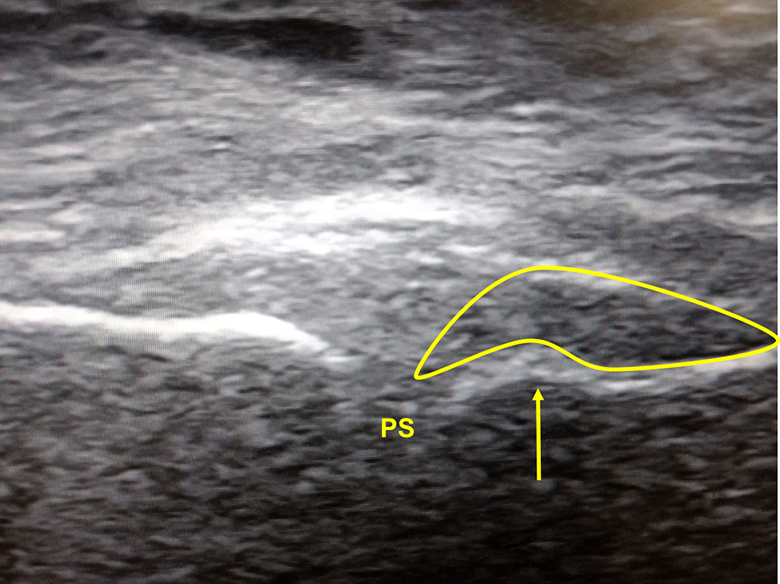
Transverse ultrasound demonstrating hypoechoic area (yellow curved shape) about the right pubic body (arrow) consistent with core muscle injury. PS, pubic symphysis.
The MRIs were read by a musculoskeletal fellowship-trained radiologist (E.M.) and considered positive if a tear along the rectus abdominis-adductor aponeurosis was visualized. Other findings associated with an aponeurotic lesion, including abnormal marrow signal intensity and a secondary cleft sign, were also noted as a positive MRI. 18 On MRI, some patients had bone marrow edema (BME) or osteitis pubis, FAI, and/or irregularities of the symphysis, but tears of the rectus abdominis and adductor longus were not appreciated and therefore considered negative (Figure 2). As such, many patients with a positive US did not have MRI findings specific for a CMI.

(A) Positive MRI. Coronal T2 fat-suppressed sequence demonstrating linear fluid signal extending to the midline, consistent with left adductor aponeurosis. Example of cleft sign (yellow arrows) indicating a core muscle injury. (B) Negative MRI. Coronal short tau inversion recovery sequence. Bright signal on both sides of symphysis pubis (yellow arrow), consistent with osteitis pubis. No aponeurosis tear was identified. MRI, magnetic resonance imaging.
Patient-Reported Outcomes
Preoperatively, patient-reported outcomes (PROs) were collected, including the visual analog scale (VAS) for pain and University of California, Los Angeles (UCLA) activity score. 1 At the most recent follow-up, patients’ VAS and UCLA scores were calculated, as was the modified Harris Hip Score (mHHS). 12
Statistical Analysis
All data were deidentified in an Excel spreadsheet (Microsoft). Data analysis was performed using SPSS; Version 20 (IBM). Patients were divided into 2 groups based on whether a preoperative MRI was read as positive or negative. Characteristics and PROs were compared between the 2 groups using a Student t test. A matched-pair t test was used to determine improvement in PROs within each group from preoperatively to latest follow-up. A post hoc power analysis was performed on VAS scores within the negative MRI group with power set to 0.8. An α value of <.05 was considered statistically significant.
Results
A total of 39 hips met inclusion criteria for this study, with a mean age of 34.8 years at the time of surgery (Table 1). Men accounted for 36 of the 39 hips included (92%). Mean follow-up at the time of the study was 20.9 ± 6.9 months (range, 12-35 months). Four hips (4/39; 10%) underwent concomitant hip arthroscopy with femoroplasty and labral repair, all of which had a negative MRI interpretation for CMI. No patients underwent revision surgery after the primary procedure.
Patient Characteristics a
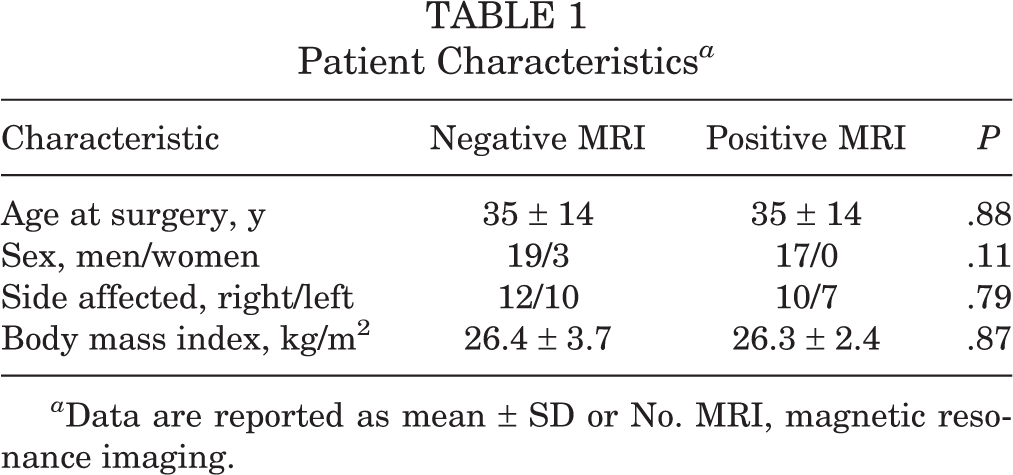
a Data are reported as mean ± SD or No. MRI, magnetic resonance imaging.
MRI Findings
MRI was interpreted as positive for a CMI in 17 hips overall (44%). Of the 22 hips remaining with a negative MRI interpretation (56%), osteitis pubis was the most common pathology noted on MRI (Table 2). Two hips were found to have signs of cam-type FAI on MRI, while 2 additional hips had clinical and plain radiographic findings of FAI, but this was not noted on MRI. Four hips were noted to have no pathology appreciated on MRI.
Magnetic Resonance Imaging Interpretations a

a Some patients had multiple pathologies noted on MRI. FAI, femoroacetabular impingement.
Patient-Reported Outcomes
No significant difference in baseline scores was found between groups (VAS, P = .93; UCLA, P = .36). Patients in both groups demonstrated significant improvement from preoperatively to latest follow-up in terms of the UCLA score (Table 3). Patients with a positive MRI interpretation demonstrated significant improvement on the VAS (P = .001), while those with a negative MRI interpretation did not demonstrate a statistically significant improvement in this score (P = .094). However, a post hoc power analysis demonstrated that a sample size of 27 patients in the negative MRI group would be needed to detect a significant difference based on the results in our cohort. No significant differences were found between groups with regard to postoperative VAS (positive MRI, 0.9; negative MRI, 2.1; P = .16) or UCLA score (positive MRI, 9.6; negative MRI, 8.4; P = .062). There were higher postoperative mHHS scores in patients with a positive preoperative MRI interpretation, although this was nonsignificant (positive MRI, 93.7; negative MRI, 86.0; P = .079).
Patients with MRI consistent with osteitis pubis demonstrated a significant improvement in VAS pain scores (6.5-1.5; P < .01), with no change in UCLA score (8.3-9.3; P = 0.23). Mean postoperative mHHS was 97.0.
Patient-Reported Outcomes a

a Bolded P values indicate statistically significant difference between groups (P < .05). Dashes indicate that this data was not collected. mHHS, modified Harris Hip Score; MRI, magnetic resonance imaging; UCLA, University of California, Los Angeles; VAS, visual analog scale.
Discussion
Despite its increasing prevalence among athletes 6 , CMI remains difficult to diagnose for several reasons. These include the nonspecific symptoms and clinical findings during examination as well as the other potential causes of groin pain (such as FAI and associated acetabular labral tears) in athletes. 2,22,23 In many athletes, groin pain may be the result of a combination of findings, and the clinician must decipher the symptomatic pathology that requires surgical treatment. As a result, there is a lack of standardized diagnostic workup for a CMI. Therefore, this study evaluated the potential of preoperative MRI in predicting clinical outcomes in patients undergoing surgery for a suspected CMI. We hypothesized that patients with a positive MRI interpretation would demonstrate improved postoperative clinical outcomes compared with those with a negative MRI interpretation.
Our study demonstrates no significant correlation between preoperative MRI findings and postoperative outcomes after mini-open CMI repair. As an entire cohort, our patients demonstrated significant improvements in the VAS for pain and the UCLA Activity Score, with no significant difference in follow-up scores between patients with a positive versus negative MRI interpretation. Patients with a negative MRI interpretation did not demonstrate statistically significant improvement in the VAS score from preoperative to latest follow-up (mean 4.1-2.1; P = .094), although this was found to be due to a low sample size based on a post hoc power analysis. In addition, we identified a nonsignificant, higher postoperative mHHS score in patients with a positive MRI interpretation (positive: 93.7; negative: 86.0; P = .079), although the clinical impact of this difference is unclear as no minimal clinically important difference in PROs has been published after surgery for CMI. It is possible that the forced rest and rehabilitation after CMI repair resulted in a beneficial impact on patients with other pathologies noted on MRI, in addition to those with classic findings of CMI.
In a previous, similar study, Kuikka et al 7 attempted to correlate the presence of preoperative BME at the pubic symphysis on MRI with postoperative outcomes in a series of 30 patients (25 men, 5 women) undergoing surgery for athletic pubalgia. The authors found that patients with (21) and without BME (9) had similar preoperative pain scores. At 3 months postoperatively, patients with BME had significantly higher pain scores (P = .03), although scores normalized at 1 and 2 years after surgery. In a follow-up study, Matikainen et al 13 performed a similar evaluation in a series of 15 female patients undergoing athletic pubalgia surgery. The authors found that female patients with BME demonstrated significantly higher preoperative pain scores than patients without BME. Furthermore, the mean time to return to sport after surgery was 5.6 months versus 3.6 months in female patients with versus without BME, respectively. Although both of these studies provide some insight into the findings related to CMI and associated outcomes, neither study attempted to differentiate outcomes between MRI findings consistent with osteitis pubis versus classic findings of a CMI indicated by a tear along the rectus abdominis-adductor aponeurosis. 18
A thorough history and physical examination are the most important aspects in accurately identifying the root cause of an athlete’s groin pain and determining the appropriate treatment thereof. In a recently published study, Kurowicki et al 8 performed a set of 4 physical examination tests in patients with suspected CMI, all of whom underwent subsequent CMI repair. The authors calculated the sensitivity and specificity of each of these tests based on a reference standard of MRI. The cross-body sit-up test as well as the presence of an adductor contracture were found to be highly sensitive but nonspecific tests for the presence of a CMI. Thus, physical examination must be assessed in combination with an appropriate history and diagnostic imaging before arriving at an appropriate diagnosis.
Among the patients in our study with a preoperative negative MRI for CMI, common pathologies noted by the radiologist were osteitis pubis and an acetabular labral tear. Two patients were noted to have findings of cam-type FAI. Palisch et al 19 noted that MRI in a patient with a unilateral rectus abdominis/adductor aponeurosis injury (ie, CMI) may demonstrate mild osteitis pubis or pubic tubercle BME. Likewise, several authors 4,9,10,17,20 have demonstrated a correlation between intra-articular hip pathology, such as FAI, and extra-articular CMI. Munegato et al 17 postulated that the restriction in hip ROM due to FAI likely contributes to the pathology identified in CMI. In a case series of 37 hips with diagnosed symptomatic athletic pubalgia and symptomatic intra-articular hip pathology, Larson et al 10 found suboptimal outcomes in those patients treated initially for only 1 of the 2 pathologies, with a high proportion of patients undergoing subsequent surgery to address the untreated pathology. In our study, 4 of 39 hips (10%) underwent CMI repair and hip arthroscopy under the same anesthetic.
By improving the clinical evaluation of CMI, we may reinforce our diagnostic capabilities and treatment options, thereby helping athletes to return to sports earlier. All patients in this study underwent surgery for a CMI, taking into account a combination of history and physical examination, positive US findings, and MRI findings. Thus, no single test was considered the gold standard in making a diagnosis of CMI. Rather, a combination of history, physical examination, and imaging findings was collectively used to arrive at a diagnosis. Given that US is examiner-dependent and therefore prone to more false readings, MRI is likely a more reliable imaging modality in the diagnostic workup for CMI. Despite this, the results of this study demonstrate that a negative MRI interpretation should not exclude this diagnosis and that patients with MRI findings that are nonspecific for CMI may still benefit from undergoing surgical intervention consisting of lengthening of the adductor longus and direct repair of the rectus abdominis to the pubis. 21
The limitations of this study should be noted. In particular, this was a retrospective study. MRI findings may be nonspecific in the setting of suspected CMI, and pathologic findings may not always appear on MRI. However, improved knowledge regarding the anatomic structures and pathophysiological changes associated with CMI has allowed improved imaging techniques. 18 This study reports on only short-term follow-up after CMI repair, and additional studies on this topic with longer follow-up are necessary. The mHHS was not assessed preoperatively in our cohort, and therefore it is possible that the groups were not equivalent with regard to this score at baseline. Last, this is a single-surgeon series, and to broaden the applicability of these tests in the diagnosis of CMI, participation of multiple centers specializing in the treatment of these patients could further validate our results.
Conclusion
Successful clinical outcomes can be expected in patients undergoing surgery for CMI diagnosed based on history, physical examination, and US. Patients with a preoperative MRI consistent with CMI may experience greater improvement in pain postoperatively, although MRI does not predict postoperative activity level in these patients.
Footnotes
Final revision submitted October 26, 2020; accepted November 29, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.J.S. has received education payments from Arthrex, consulting fees from DePuy/Medical Device Business Services, and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by St. Joseph’s Healthcare System.