
Abstract
Purpose:
To publish the Spanish translation of Version 12 of the sports injury classification system called Orchard Sports Injury Classification System and propose a modification to include a numerical code that reflects the impact of the injury on sports functionality.
Methods:
The members of the working group on the epidemiology of sports injury, of the Group for the Study of the Muscle-Tendon System (GESMUTE), and of the Spanish Society of Sports Traumatology (SETRADE), carried out a bibliographical review on the epidemiological classification systems of injuries, 3 face-to-face consensus meetings, and various online pieces of work, following the Delphi work methodology.
Results:
The Spanish translation of Version 12 of the Orchard Sports Injury Classification System is fully accessible and free of charge at https://gesmute.es/traduccion-espanola-osics-12/. The current project proposes to add, at the end of the current coding system of Version 12, a numerical code (0: No Functional impairment; 1: Limits Sports Activity; 2: Prevents Sports Activity; 3: Limits Daily Life Activities), to indicate any functional repercussions caused by the injury.
Conclusion:
We present the Spanish translation of Version 12 of the Orchard Sports Injury Classification System. We propose as an improvement the inclusion of functionality criteria in sports injury classifications; more specifically, our proposal could be an improvement to the Orchard Sports Injury Classification System Version 12.
Keywords
The Group for the Study of the Muscle-Tendon System (GESMUTE) is made up of specialists in various disciplines, all of them affiliated with the Spanish Society of Sports Traumatology (SETRADE). Within GESMUTE, the work group for the epidemiology of sports injury has analyzed the most commonly used classification systems in sports injuries, with the aim of assessing the pros and cons of each system used and to propose one of them to GESMUTE so that it may apply such a system for any of its future studies.
There are many classifications (Table 1), and one of the most commonly used was created in 1992 by Dr Orchard, named the Orchard Sports Injury Classification System (OSICS), 14 which is currently in its 12th version. Version 10 had previously been translated into Spanish, 7,14,17,18 and it was now Version 12’s turn to be translated also into Spanish. 4

The various aforementioned systems proposed
2,8,10,14
usually include a questionnaire-based document that collects data related to the injury or sports accident, which are later introduced into a database to be analyzed and studied with the aim of Establishing preventive measures. Optimizing the rules of the game for every sport. Enabling institutions to adequately plan health assistance during sporting events.
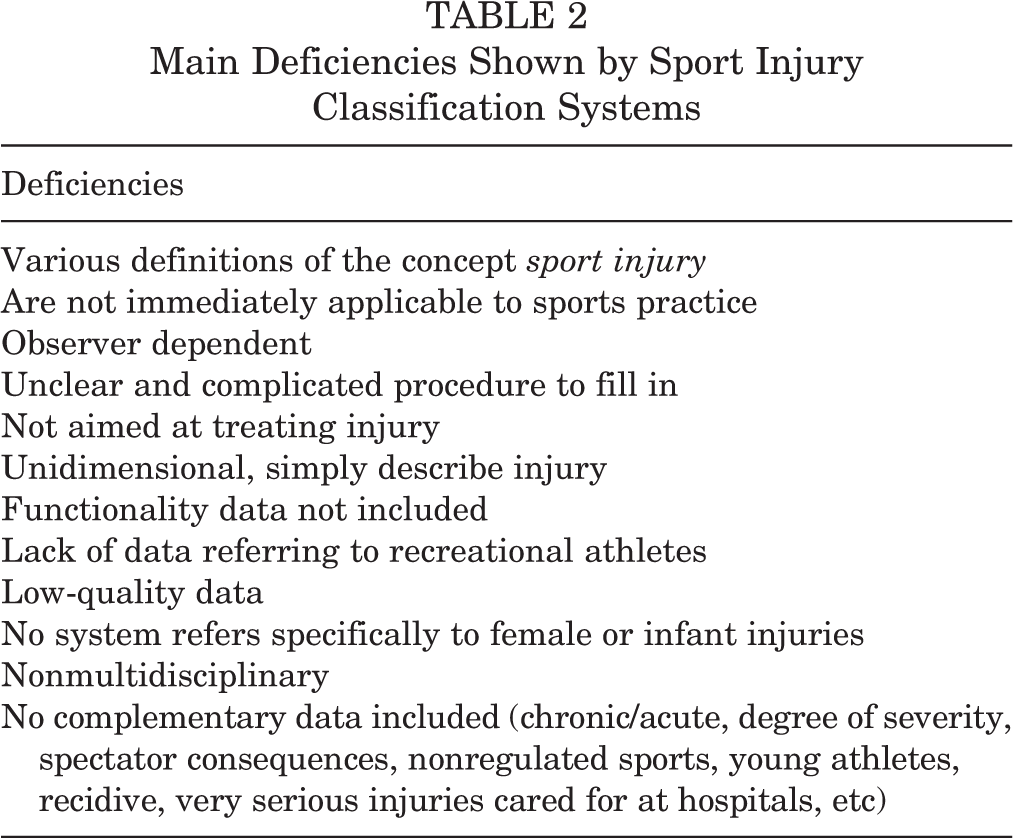
Despite being useful when it comes to performing epidemiologic studies and providing health care support, these systems are not constraint-free (Table 2) 2,7,8,14,17 : enough reason to spur multiple groups to improve them 7,9,11 (Table 2) and reach consensuses in order to narrow the gap caused by discrepancies. 2
Main Deficiencies Shown by Sport Injury Classification Systems
After considering all the aforementioned, the GESMUTE work group decided to meet in Madrid on 22 September 2018 and agreed to analyze the different epidemiological code assignment systems used in sport injury classification, with the aim of choosing a single one to be applied in the future by the group. This study describes the results obtained and level of agreement reached.
Methods
Using the Delphi methodology
16
(work and consensus following an in-line process structure used in group meetings), members of GESMUTE’s epidemiology work group carried out the following activities: 1 September 2018 to 20 September 2018: Agreed on consensus to establish task goals to achieve. 22 September 2018: GESMUTE agreed to revise and analyze all aforementioned injury classification systems so that one of them may be used and applied by GESMUTE in the future. 23 September 2018 to 30 March 2019: revised references and analyzed the various epidemiological sport injury classification systems. 30 March 2019: GESMUTE chose the OSICS-12 classification system and reached consensus to use it in future studies. It additionally agreed to add a numerical code system that defines functional impact caused by injury. 30 March 2019 to 11 November 2019: contacted Dr Orchard so that he may approve translation of the OSICS-12 classification system into Spanish. Additionally, established points to discuss for the next meeting to be held on 23 November 2019 by GESMUTE. 23 November 2019: Modifications proposed for the OSICS-12 classification system were approved and a functional code added. 25 November 2019 to 15 December 2019: consensus reached upon work methodology to follow when translating and also regarding full translation of OSICS-12 into Spanish. 15 December 2019 to 30 January 2020: discrepancies solved and consensus reached concerning OSICS-12 translation proposals. 13 January 2020 to 20 January 2020: the Ibero-American group (Chile, Argentina, Uruguay, and México) of specialists in sports medicine was contacted and joined the main group in order to translate OSICS-12 into Spanish. 30 January 2020 to 5 March 2020: OSICS-12 translation consensus was finalized. 24 April 2020: Spanish version of translated OSICS-12 and proposed improvements were published in Spanish scientific journals.
All group meetings where held at Clínica CEMTRO on 22 September 2018, 30 March 2019, and 23 November 2019.
Results
All 1733 diagnostic terms, 41 injury categories, and 13 body areas that make up the OSICS-12 system were translated. Translated information and full text in spreadsheet format are available for free at https://gesmute.es/traduccion-espanola-osics-12. The most important decisions taken by all of GESMUTE work group members at their meetings were To use the OSICS code system of sports injuries for future epidemiological studies. To translate OSICS-12 into Spanish.
4
To categorize each injury into corresponding anatomic regions. We believe such categories help to make a more efficient use of this classification system. To propose the introduction of a modification in the OSICS-12 system
4
that includes adding a number code at the end of the already existing code, with the aim of indicating how the injury affects this area functionally (Table 3).
Proposed Codes to Indicate Functional Repercussion of Every Injury

Additionally, validation of OSICS-12 Spanish translation has started both in Spain and Latin America.
Discussion
Main results in this study include GESMUTE’s adopting the OCICS classification system and translating it into a Spanish version of OSICS-12. 4 The translated information and full text in spreadsheet format may be accessed for free on https://gesmute.es/category/publicaciones/. Additionally, a proposal to improve OSICS’s injury classification system was made by which a final figure is added at the end of each code, which indicates functional repercussion of the injury when practicing sport.
The OSICS-12 system follows a 4-character structure, assigned to each injury. 10,14,17,18 The first letter in this structure indicates an anatomic region; the second letter corresponds to a specific injured tissue or the name of the pathology present; the third and fourth letters describe the pathology and provide further diagnosis. This system 7,14,18 is constantly updated; it is flexible enough to include new categories and adapt to new concepts 4 without invalidating previous versions; and it has a wide-enough range to include all types of injuries. Since it was first published, its authors have refused to have any copyright ownership. It has been validated 10 ; its applicability has been proven 7 ; and it is widely used in sport injury epidemiology. 1,14,18 The main reasons for this system’s being mentioned so often in papers are that it provides a precise encoding system and that forthcoming modifications have always led to improved versions. The OSICS system has improved over time, adding new codes and categories that allow structural anomalies to be included, as well as pathologies shown by para-athletes, pediatric injuries, postsurgical conditions, medical pathologies, administrative actions taken, and data collected regarding uninjured athletes. 7,14,18 Additionally, it has been translated into several languages, including Spanish. 4,17,18
Classifying an injury implies describing it, as well as including it in a category and establishing its level of severity. 12
Keeping all 3 of the above in mind,
3,5,6,12,15,19
–21
the applied taxonomy should Show reproducibility. Establish clear differences among categories. Be easily remembered. Be concise and easily understandable. Include prognosis variables.
However, the OSICS system begins to lack precision when the encoding system is applied by non–health care staff, 10 giving ground to the proposal of variations that may somehow assess injury relapses (subsequent injury categorization model). 9
Sports injury research needs an appropriate encoding system for the different pathologies, with the aim of truly knowing their incidence, a precise location, the injury mechanism that caused them, any efficient preventive measures to be taken, the efficacy of all different treatments applied to the same injury, 1,2,9,14,18 and making the right return-to-play decisions. Nevertheless, the same injury may have various effects on a given sports activity, such as when an Achilles paratendinopathy (code OSICS-12: ATAP) is invariably assigned the same code such that it becomes uncertain whether the injury is totally incapacitating for the athlete or if it allows him or her to continue to train per usual. If we wish to analyze the efficacy of various treatments or choose the kind of exercise we may apply when treating an injury, it is essential to know to what extent the injury affects sport activity. This is why the GESMUTE epidemiology work group agreed to add a number indicating the extent to which an injury functionally affects the athlete. 4 As an example, take an Achilles paratendinopathy, which may not hinder an athlete’s physical activity; that is, without functional side effects. We would code it as ATAP-0. But if such an injury does produce pain that does not allow any kind of physical practice, we would code it ATAP-2. Such coding could be useful when establishing a treatment protocol to apply to the injury—for example, in the case of a nonlimiting Achilles paratendinopathy (ATAP-0), we may use eccentric and plyometric exercises almost limitlessly, whereas in the case of a highly functionally limiting Achilles paratendinopathy (ATAP-2), those exercises would be unadvisable. We are thus favoring a collaborative approach from all sports health care specialists, from diagnosis, treatment, and rehabilitation to the prevention of injuries—hence, our position on considering it advisable to add a number after every OSICS-12 code with the aim of referencing the functional impact of each and every injury.
For the future, we are considering validating the Spanish translation of OSICS-12 in both Spain and Latin America, as well as translating into Spanish any future versions of OSICS. Furthermore, GESMUTE is promoting the development of an application program that facilitates injury code assignment using OSICS-12.
Footnotes
Acknowledgment
The authors acknowledge the following: Dr Tomás Fernández Jaén for his unconditional support and partnership leading to this project’s coming to life. Clínica CEMTRO, in the person of its founder, Prof P. Guillén, for hosting every necessary meeting, for nurturing this project from the very beginning and for their support in any project related to sports medicine in Spain. Dr Jean Christophe Romagnoli Prado, Dr Begoña Zubieta Planella, Dr Diego Barriga González, and Dr Claudio Troncoso Sepúlveda, all from the School of Sports Medicine of the Santiago de Chile University, Chile, for their contribution to the English-to-Spanish translation.
This article, “Translation Into Spanish and Proposal to Modify the Orchard Sports Injury Classification System (OSICS) Version 12,” was originally published in Spanish in Revista Andaluza de Medicina del Deporte in Volume 13, Issue 2, June 2020 (available at ![]() ) and is republished here in English with the permission of Apunts Sports Medicine (doi: 10.1016/j.apunsm.2020.05.002) where the article originally appeared in 2020, Volume 55, Issue 207 (pp 105-109).
) and is republished here in English with the permission of Apunts Sports Medicine (doi: 10.1016/j.apunsm.2020.05.002) where the article originally appeared in 2020, Volume 55, Issue 207 (pp 105-109).
Final revision submitted August 6, 2020; accepted August 6, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.