
Abstract
Background:
Street workout (SW) is an urban sport based on calisthenic exercises. Injury profiles and risk factors are widely explored in various sport disciplines. However, because of the lack of research in SW, injury profiles have not yet been established.
Purpose:
To investigate the characteristics and prevalence of injuries and variables that may increase these odds in SW practitioners.
Study Design:
Case-control study; Level of evidence, 4.
Methods:
An electronic survey was conducted between September 2018 and March 2019 in order to obtain practitioner information, physical activity level, training characteristics, and injury information of SW practitioners. Responses from 93 practitioners were eligible for analysis. Univariate and multivariate binary logistic regression analyses were used to examine the association among several variables and the presence of injury in the past 12 months based on odds ratios (ORs).
Results:
Overall, 62.4% of the 93 participants reported an injury in the previous 12 months, and tendinopathy was the most reported diagnosis (31.0% of injured practitioners). High injury frequency was reported in the shoulder (23.0%) and back (upper and mid) (18.4%). Overtraining was the most reported perception of cause of injury (56.9%). Most injured practitioners (20.7%) performed freestyle exercises before the injury, followed by upper body exercises. A history of previous injuries (OR, 4.078; P = .005) and the middle and higher tertiles of vigorous physical activity (OR, 4.370; P = .015 and OR, 5.634; P = .003, respectively) were associated with a higher odds of injury.
Conclusion:
In SW, the shoulder and back (upper and mid) were the most injured body parts, with tendinopathy being the most frequent diagnosis. Overtraining was typically reported as the perceived cause of injury, with freestyle and upper limb exercises the most performed exercises when injured. A history of previous injuries, along with vigorous physical activity, was found to augment the odds of injury. More research is needed to corroborate our findings, along with increased knowledge about SW practice and injuries.
Street workout (SW) is an urban sport based on calisthenic exercises. It is considered a type of bodyweight training, performed with or without a handheld apparatus, commonly used for improving strength, body composition, and posture. 23,36,39 According to a recent survey by the American College of Sports Medicine, calisthenic exercises ranked seventh in fitness trends for 2020. 37 Research has shown that adolescents and young men tend to practice SW, with various approaches in social networks. 35 Male SW practitioners typically have a low fat mass and a high muscle mass in the upper arms and trunk. 33
SW practitioners usually perform isometric and isotonic bodyweight exercises, as well as various swings and combinations, called freestyle/dynamic exercises. Calisthenic exercises include some variations to modify muscle recruitment patterns and load. 4,9,24 Freestyle also has some similarities with exercises in gymnastics, such as the high bar, parallel bars, and uneven bars, in which several transitions, release moves, and dismounts are often used. The biomechanics of SW exercises have not been explicitly explored, although based on the similarity of these exercises with gymnastics, specific mechanical requirements and functional phases may be involved. 18
Some exercises commonly performed for SW training have been linked to injuries. For example, it has been suggested that wide and reverse pull-ups may trigger shoulder impingement due to compression of the rotator cuff and subacromial bursa during the exercises. 31 The wide pull-up decreases the range of protraction and retraction, and the reverse pull-up has an excessive glenohumeral internal-external rotation, reducing subacromial space. 31 Other SW exercises (ie, muscle-up with wide hand placement or human flag) have similar pulling mechanics; thus, we hypothesized that they may increase the shoulder’s injury rate. During the push-up, another exercise in SW, a hyperextended wrist position has been shown to increase and change the direction of dynamic forces in the wrist to areas less prepared to absorb forces, such as the triangular fibrocartilage complex. 30 Repetitive execution of exercises is typical among SW practitioners, and the cumulative effects of microtraumatic forces during movements may contribute to overuse injuries. 14 The relationship between freestyle exercises and injuries is unknown; however, some similarities may exist with injuries in gymnastics exercises with the bars. For example, in gymnasts, researchers have reported injuries on the uneven bars mainly due to contact with the surface or apparatus, causing concussions, shoulder muscle/tendon strains, or hand/wrist sprains. 20 Several upper extremity injuries occur in gymnasts on the high bar, 41 linked to gymnastics events, and with floor exercises, followed by the still rings, horizontal bars, and parallel bars. 26 Freestyle and bodyweight exercises in SW are commonly performed, and thus a link between injuries and these exercises may exist.
Other factors associated with injuries are physical activity levels, 28 sport specialization, 3 age, 15 body mass index (BMI), 15 and sex. 2,6 A multifactorial approach of how several factors are linked to injury risk must be assessed for knowledge of this discipline and a reduced injury rate. In this way, given the lack of research in SW and how injury profiles have not been established in the literature, this study aims to describe the epidemiology of injuries and examine whether practitioner or training characteristics are associated with an increase in injury.
Methods
Study Design and Participants
The study protocol was approved by the sponsoring university’s ethics committee and met the criteria of the Declaration of Helsinki. Through a retrospective observational design, study data were collected via an electronic survey using Google Forms (Google LLC); this was done between September 2018 and March 2019. Target respondents were SW practitioners. There were no incentives offered for completing the survey. Participation was voluntary, and contestants were informed that survey completion implied their consent.
SW practitioners were included if they were >18 years of age, were practicing SW in Chile, had sustained (or not) an injury during SW training, and successfully completed the survey. Exclusion criteria were incomplete responses and any injury that was not associated with SW training (in cases of reported injury).
Online Survey Assessment
The online survey was adapted to coincide with the scope of SW based on the study of Mehrab and colleagues 27 in CrossFit athletes. The survey was translated into Spanish and distributed to online Chilean SW social media platforms. The survey focused on participant information, anthropometric data, physical activity level, training characteristics, and injuries. The definition of injury was adjusted to coincide with the scope of SW based on the study of Weisenthal and colleagues 40 in CrossFit athletes. Thus, injury was defined as any new musculoskeletal pain, feeling, or injury that occurred from an SW practice and led to 1 or more of the following categories: (1) total removal from SW training and other outside routine physical activities for >1 week; (2) modification of normal training activities in intensity, mode, or duration for >2 weeks; and (3) any physical complaint severe enough to warrant a visit to a health professional. The definition of injury was included in the survey.
Practitioner data consisting of sex, age, and educational level were collected. Each participant also self-reported anthropometric data, including height and weight for computing BMI. Participants were categorized by BMI level: underweight (BMI, <18.5), normal weight (18.5-24.9), overweight 25.0-29.9), and obese (≥30).
Physical activity and components were assessed through the International Physical Activity Questionnaire–Short Form (IPAQ-SF), 7 which was included with the online survey shared with participants. Participants were asked about their physical activity for the previous 7 days. The frequency and duration of vigorous physical activity (VPA), moderate physical activity (MPA), and time spent walking on a typical weekday were collected. Data were processed based on previous recommendations. 17 This included data cleaning, exclusion of cases (missing data or outliers), truncation of data, and calculation of metabolic equivalent of task (MET) hours per week. Physical activity was classified as low, moderate, or high based on IPAQ guidelines. 17 The level of walking, MPA, VPA, moderate to vigorous physical activity, and total MET hours per week were categorized in tertiles, as lower, middle, and higher.
Regarding training characteristics, the survey focused on information such as training experience, modality, duration, frequency, and training location. Participants self-reported about injuries in SW, which included the number of injuries over the past 12 months, the medical diagnosis of the injury (bursitis, concussions, cramps, fractures, dislocations, periostitis, strains, tendinopathies, and others), the injured body parts, the exercise that triggered the injury, the perception of the cause of the injury, and history of previous injuries. The athletes’ perception of the causes of injury, through questionnaires, has been previously used. 22,27
Statistical Analysis
Data analysis was performed using IBM SPSS Statistics Version 25 for Mac (IBM Corp). Practitioner, anthropometrics, training, and injury data were used to describe the sample and injury patterns. Univariate binary logistic regression was used to examine associations between these variables and the history of injury over the previous 12 months based on odds ratios (ORs). The dependent variable of logistic regression was dichotomous: injury history compared with no injury history. Variables associated with univariable analyses were included in a multivariable binary logistic regression. The significance level was set at P < .05.
Results
A total of 127 responses were collected, and as the survey was an open platform, we could not determine the number of surveys sent. Six duplicated responses were removed, and 28 responses were excluded because of incomplete answers (n = 9), injury not associated with SW training (n = 5), age <18 years (n = 13), and practice of SW not in Chile (n = 1). In total, 93 practitioners’ responses were eligible for inclusion. The practitioner and anthropometric data of the participants are presented in Table 1. Male practitioners (82.8%) comprised most of the sample, and most participants (82.8%) reported a normal weight. The majority of participants (84.9%) were university students or professionals, and 47.3% of respondents participated in SW competitions/tournaments.
Participant, Anthropometric, and Physical Activity Data of Street Workout Practitioners a

a Data are expressed as mean ± SD or n (%).
The physical activity characteristics of the participants are shown in Table 2. Based on the IPAQ-SF responses, most participants (91.4%) declared a high level of physical activity, and 89 out of 93 practitioners (95.7%) reported a weekly VPA time >75 to 150 minutes. The information on tertiles of time spent (walking, MPA, VPA, and moderate to vigorous physical activity) and MET hours per week is shown in Table 2.
Physical Activity Characteristics of Street Workout a
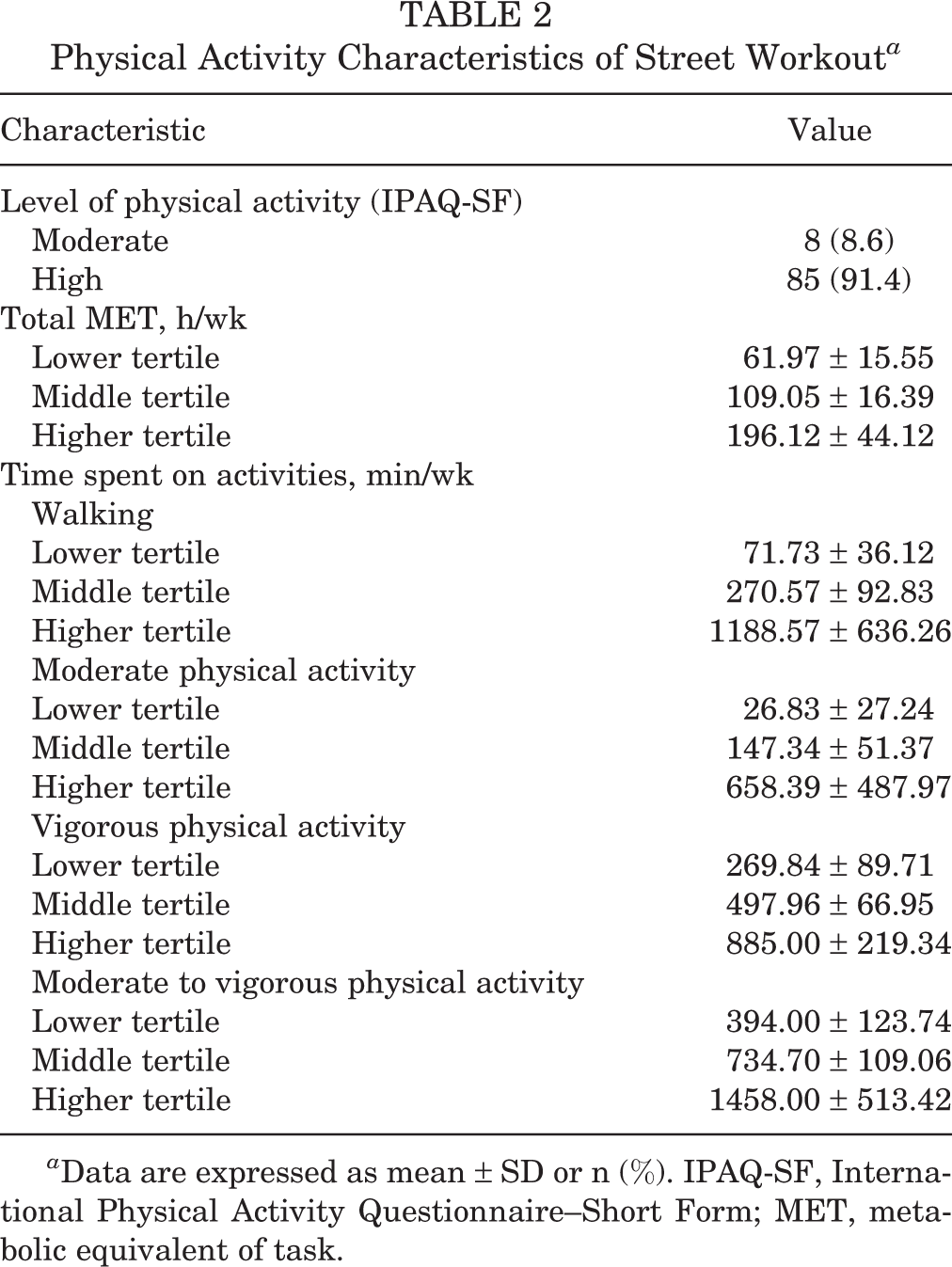
a Data are expressed as mean ± SD or n (%). IPAQ-SF, International Physical Activity Questionnaire–Short Form; MET, metabolic equivalent of task.
The distribution of training experience and characteristics of SW practitioners can be seen in Figure 1. Most respondents (n = 56) were experienced practitioners (>2 years of training). Regarding training characteristics, most participants performed individual training sessions (n = 47), and one-third had multiple training sessions per day. Most participants committed (89.2%; n = 83) to at least 1 hour per training session. The most common training location was SW/calisthenics parks (90.3%; n = 84), followed by fitness centers (26.9%; n = 25), playgrounds (10.8%; n =10), and home (10.8%; n = 10). Of the practitioners, 37 (39.8%) used only 1 training location, 37 (39.8%) used 2, 17 (18.3%) used 3, and 2 practitioners (2.2%) used 4 locations for training.

Training experience and training characteristics of street workout practitioners.
The weekly training distribution is presented in Table 3. The mean ± SD SW training frequency was 4.03 ± 1.32 d/wk, and most sessions were performed through bodyweight training, followed by skill/technique, mobility, and weight training. Dynamic/freestyle training was carried out the least.
Weekly Training of Different Exercises Among Street Workout Practitioners

The number of injuries in the past year and the history of previous injuries are shown in Figure 2. Most participants (62.3%; n = 58) were evaluated with at least 1 injury in the past 12 months. In addition, 60 out of 93 participants (64.5%) declared a history of previous injury. Regarding injured practitioners, most had tendinopathies (31.0%; n = 18), followed by sprains (10.3%; n = 6), muscle strains (8.6%; n = 5), bursitis (5.2%; n = 3), dislocations (3.4%; n = 2), cramps (3.4%; n = 2), fractures (1.7%; n = 1), periostitis (1.7%; n = 1), and other (20.7%; n = 12), while 22.4% declared that they did not have a medical diagnosis (n = 13). When injured, 72.4% of participants stopped training sessions, with healing taking a mean ± SD of 4.0 ± 5.7 weeks. The most perceived cause of injury was overtraining (n = 33; 56.9% of injured practitioners), followed by inappropriate execution of the exercise (27.6%), fatigue (25.9%), and no warm-up (19.0%) (Figure 3A). When injured, most practitioners stated they were performing freestyle/dynamic exercises (20.7%), followed by muscle-ups (12.1%), planches (12.1%), front levers (10.3%), and other exercises (10.3%) (Figure 3B). When asked on what they were exercising at the time, the bar was the most reported structure (50.0%), followed by parallel bars (24.1%), the ground (19.0%), gymnastics rings (5.2%), and other (1.7%).
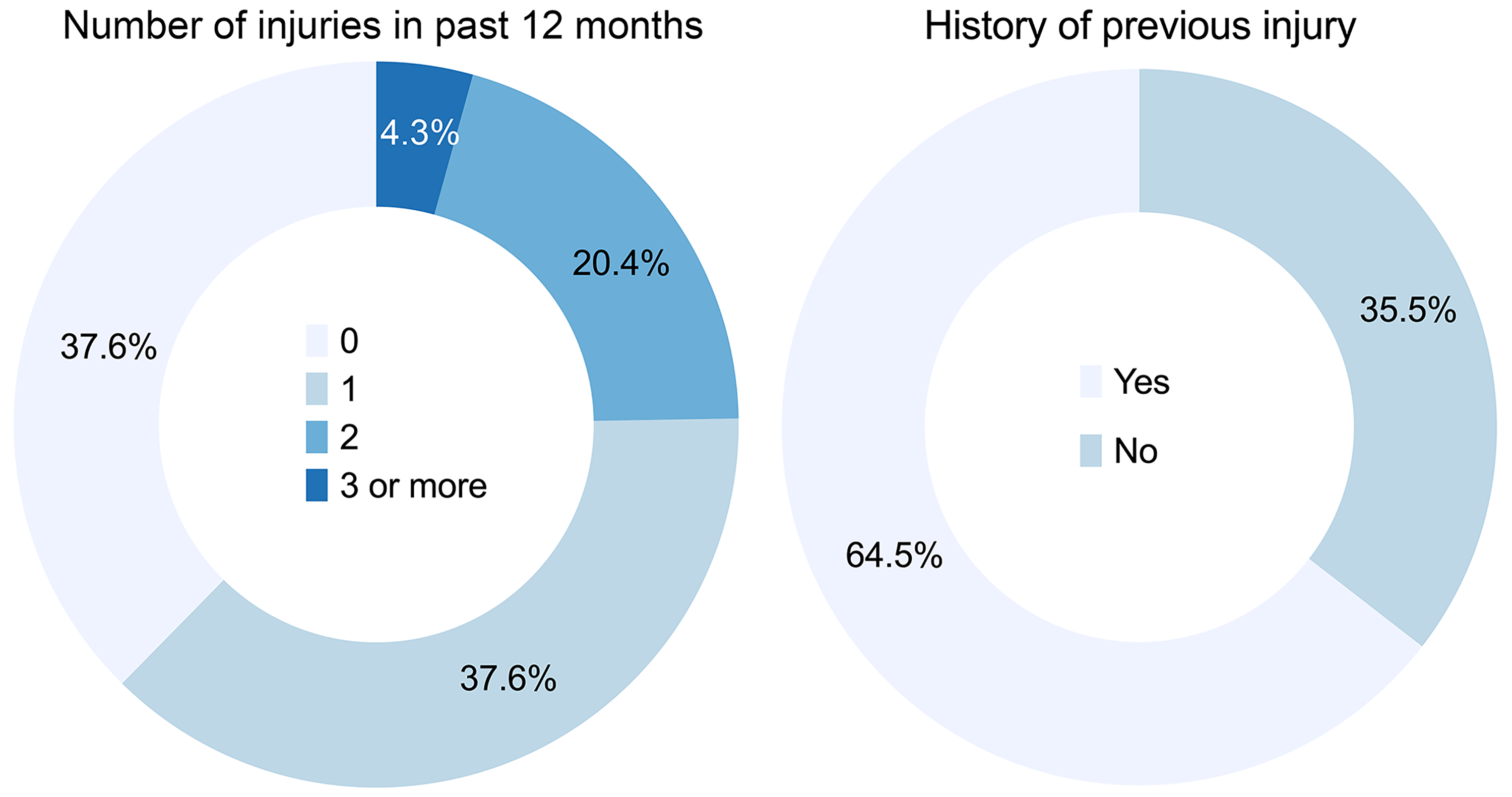
Proportion of number of injuries in the past year and history of previous injuries among street workout practitioners.
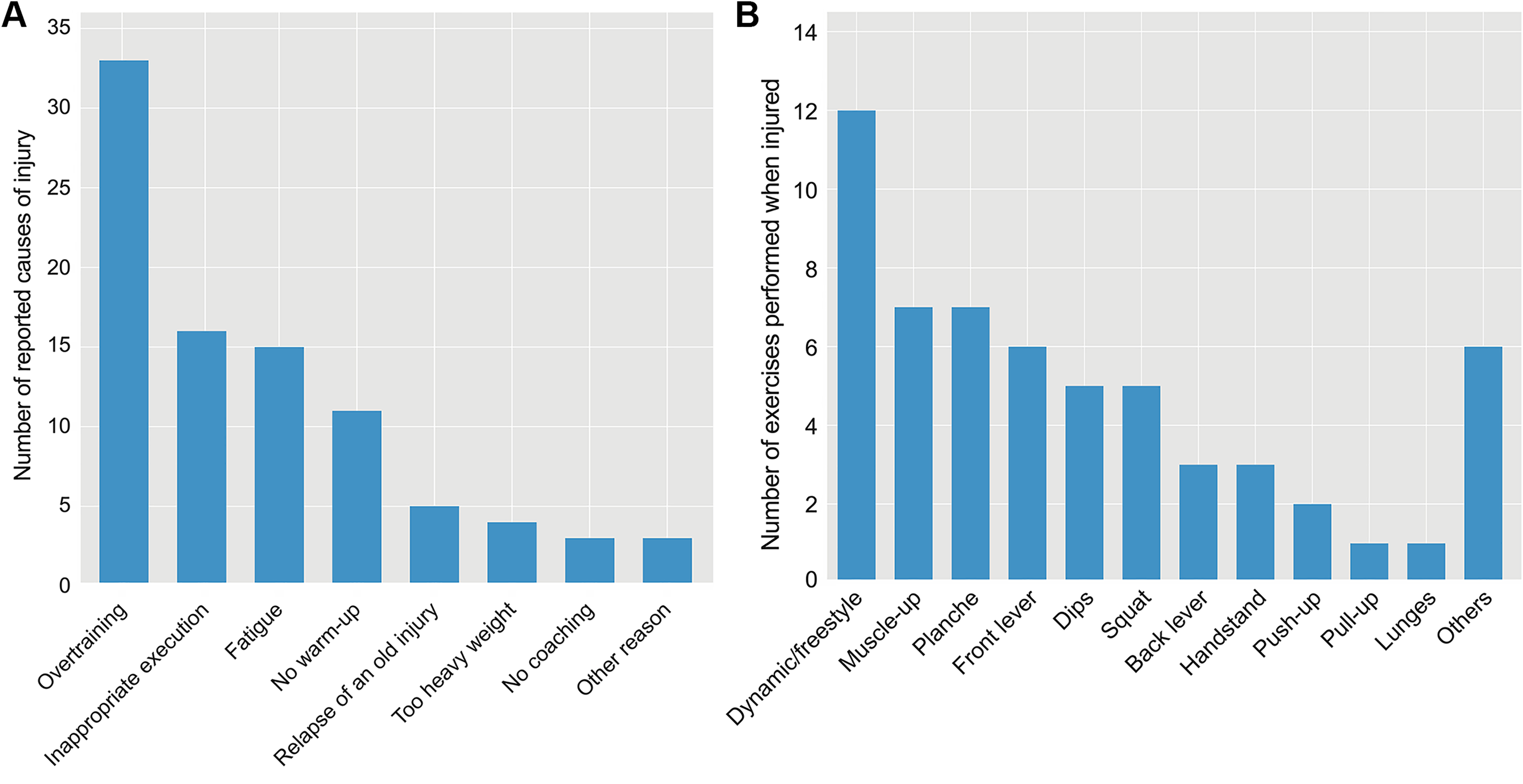
(A) Number of perceptions of injury cause and (B) number of exercises performed when injured among street workout practitioners.
The number of injured body parts among SW practitioners can be seen in Figure 4. The total number of reported injured body parts was 87, and the most injured body part was the shoulder, followed by the back (upper and mid), elbow, and wrist.

Number of injured body parts among street workout practitioners.
The univariate analyses of practitioner characteristics, anthropometrics, history of injury, physical activity characteristics, and training characteristics are provided in Appendix Tables A1 to A3. All variables with P < .05 were used for the multivariate analysis, which included the history of previous injury (OR, 3.732 [95% CI, 1.522-9.149]; P = .004), middle and higher tertiles of VPA (OR, 3.563 [95% CI, 1.183-10.731]; P = .024 and OR, 5.542 [95% CI, 1.905-16.117]; P = .002, respectively), ≥3 weekly sessions of technique/skill training (OR, 7.273 [95% CI, 1.230-43.004]; P = .029), and 2 and 3 training locations (OR, 3.176 [95% CI, 1.202-8.395]; P = .020 and OR, 3.824 [95% CI, 1.049-13.953]; P = .042, respectively).
In terms of the multivariate analysis, the independent factors found to escalate the odds of injury were a history of previous injury (OR, 4.078 [95% CI, 1.530-10.869]; P = .005) and middle and higher tertiles of VPA (OR, 4.370 [95% CI, 1.332-14.341]; P = .015 and OR, 5.634 [95% CI, 1.828-17.365]; P = .003, respectively).
Discussion
This is the first study describing the injury profile in SW. Based on our results, most injuries occurred at the shoulder and back (upper and mid), with tendinopathy being the most reported injury diagnosis. Overtraining was the most commonly perceived case of injury. Freestyle and upper body exercises were the exercises being performed the most when participants were injured. In addition, it was found that a history of previous injuries and higher levels of VPA raised the odds of an injury.
A high percentage of shoulder and upper limb injuries are described in sport activities similar to SW in which upper body exercises are commonly used. 5,27 The exercises most often linked to injury in SW are freestyle/dynamic and upper body exercises, such as muscle-ups, planche, and front lever. On the one hand, freestyle exercises are similar to movements performed on uneven bars and high bar gymnastics, which could explain the similar pattern of injured body parts. 20,41 However, the lack of a structured training program with progression is common in SW, which suggests a higher rate of injury than that in gymnastics. On the other hand, vigorous upper body exercises such as the muscle-up, in which the practitioner hangs from the bar or rings, requires a pull-up and then transitions into a triceps dip position; this may apply high stress to the shoulder and upper body limb. The glide kip is a gymnastics movement, similar to the muscle-up, except it has a marked kip phase. 21 It has been suggested that reductions in the leg swing during the glide kip may increase the stress on the hands and shoulders, 1 which could explain why performing the muscle-up can result in injury. Upper body isometric exercises, such as the planche and front lever, were also reported as injury-prone exercises. The planche has been described to require a high level of upper body strength, specific biomechanical phases for execution, and correct training progression. 19 As such, injuries attributed to these exercises could be due to noncompliance with the above-mentioned requirements. Freestyle and upper body exercises in SW demand repetitive movements of the shoulder above the horizontal plane; moving the shoulder above 90° has been found to be a risk factor for rotator cuff tendinopathy. 25 Tendinopathies were the most common injury in this study and may be linked to SW exercise characteristics.
Despite these findings and assumptions, weekly freestyle training, bodyweight, and overall SW were not factors that increased the odds of injury. Moreover, freestyle sessions were carried out the least among SW practitioners, suggesting that acute injuries during freestyle exercises may be due to inappropriate execution of the movement; overtraining was the most reported cause of injury. It is assumed that strenuous bodyweight training sessions (63.4% of participants spent >90 minutes per training session) affected the quality of movement, explaining how freestyle sessions can result in injury. A similar assumption was made between bodyweight exercises and injuries. Because the sample size was small, it was not possible to obtain a clear distribution of exercise, injury, and perception of the injury’s cause. Future studies with more athletes should explore whether some factors of movement execution and training characteristics may be linked to injury.
Looking at the levels of weekly VPA, technique/skill training sessions and the number of training locations were associated with injury prevalence in univariate analyses. An unstructured high physical demand for movement execution in technique sessions, high levels of vigorous training, and an excess of training in different locations could partially explain these findings. Moreover, the VPA time was seen as an independent factor that increased the odds of injury. Previous studies have found a positive relationship between training loads and injury rates: the higher the training intensity, the more injuries athletes sustained. 12 Most practitioners (95.7%) reported a weekly VPA time >75 to 150 minutes, as recommended by physical activity guidelines. 29 Meeting physical activity guidelines was related to higher activity-related injuries. 16,28 However, the relation between VPA and injury must be carefully assessed: people have reported higher moderate and vigorous physical activity times in questionnaires compared with the objective measurements of physical activity. 8
The history of previous injuries was found to be a crucial factor that independently increased the odds of injury in SW. Again, most practitioners (64.5%) claimed they had a history of previous injuries. Several studies have reported that a history of previous injuries would increase the risk of reinjury. 13,34 This association can be explained by a change in strength, proprioception, and kinematics in the injured state, which may lead to changes in motor control and function. 10 Maximal effort in SW freestyle and bodyweight exercises may be a challenge for practitioners, especially those injured before and not fully recovered. Some injured practitioners (22.4%) declared that they did not have a medical diagnosis; it is unknown whether the rest of the injured practitioners completed a rehabilitation program. More research must be done to evaluate the effect of physical therapy and preventive interventions in common injuries of SW.
The present study has some limitations. Given the nature of retrospective design, there may have been registry bias or a recall bias when participants answered the survey, so this study on SW may not provide a complete picture of injury epidemiology in Chile. The sample size’s representative value is unknown because of the lack of a national registry of SW practitioners. A number of potential respondents could be obtained based on the number of total followers of SW groups in social media; however, response rates could not be calculated, as it was not possible to calculate the number of people who viewed the advertisement. As a result, the number of surveys sent could not be determined. It was clarified that study participation was directed at whether SW practitioners sustained an injury while performing. It is unknown what motivated participants to respond to the survey, but a potential reason could be a history of injuries. 11,32 For this reason, there may have been a selection bias.
The medical diagnosis of injury was unknown, so results must be taken with caution. Future studies need direct access to medical history in order to corroborate our findings. Because most participants were male, our results could have been influenced by sex. 38 Finally, future studies with larger sample sizes should corroborate our results. Longitudinal studies that follow training sessions and competitions are also needed to identify which exercises, biomechanical patterns, sex, or modifiable factors result in injury to the shoulder, back (upper and mid), and upper limbs.
Conclusion
In our SW survey, the shoulder and back (upper and mid) were the most injured body parts, and tendinopathy was the most frequent diagnosis. Overtraining was the most reported perceived cause of injury, with freestyle and upper limb exercises the most performed when injured. A history of previous injuries and more VPA were found to increase the odds of injury. Further research should corroborate our findings, as well as enhance the knowledge about the practice of SW.
Footnotes
Acknowledgment
The authors thank the study respondents for their invaluable participation. They also thank the editor and reviewers for providing insightful comments and suggestions that improved the quality of the paper.
Final revision submitted September 4, 2020; accepted November 5, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.S.-U. was supported by a grant from CONICYT/BECAS Chile/72180543. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Pontificia Universidad Católica de Valparaíso (BIOEPUCV-H248-2018).
Appendix
Odds Ratios for Injury by Training Characteristics a

| Characteristic | Injured, n | Odds Ratio (95% CI) | P Value | |
|---|---|---|---|---|
| Yes | No | |||
| Multiple sessions per day | 23 | 8 | 2.218 (0.859-5.725) | .100 |
| Training modality | ||||
| Individual (ref) | 30 | 17 | 1 | |
| Group | 22 | 16 | 0.779 (0.324-1.872) | .577 |
| Combined | 6 | 2 | 1.700 (0.308-9.374) | .542 |
| Training duration, min | ||||
| ≤90 (ref) | 23 | 11 | 1 | |
| >90 | 35 | 24 | 0.697 (0.287-1.693) | .426 |
| Training frequency (d/wk) | ||||
| Street workout training | ||||
| 1-2 (ref) | 5 | 6 | 1 | |
| 3-4 | 28 | 18 | 1.867 (0.496-7.032) | .356 |
| ≥5 | 25 | 11 | 2.727 (0.684-10.868) | .155 |
| Bodyweight training | ||||
| ≤2 (ref) | 14 | 14 | 1 | |
| ≥3 | 44 | 21 | 2.095 (0.848-5.179) | .109 |
| Bodyweight training with weights | ||||
| 0 (ref) | 19 | 10 | 1 | |
| 1-2 | 31 | 17 | 0.960 (0.365-2.526) | .934 |
| ≥3 | 8 | 8 | 0.526 (0.152-1.825) | .312 |
| Dynamic/freestyle training | ||||
| 0 (ref) | 29 | 23 | 1 | |
| 1-2 | 21 | 10 | 1.666 (0.657-4.225) | .283 |
| ≥3 | 8 | 2 | 3.172 (0.613-16.408) | .169 |
| Technique/skill training | ||||
| 0 (ref) | 2 | 5 | 1 | |
| 1-2 | 24 | 19 | 3.158 (0.551-18.114) | .197 |
| ≥3 | 32 | 11 | 7.273 (1.230-43.004) | .029 b |
| Mobility training | ||||
| 0 (ref) | 8 | 6 | 1 | |
| 1-2 | 25 | 12 | 1.562 (0.442-5.523) | .488 |
| ≥3 | 25 | 17 | 1.103 (0.324-3.754) | .875 |
| Participation in other sports (d/wk) | ||||
| 0 (ref) | 28 | 17 | 1 | |
| 1-2 | 19 | 13 | 0.887 (0.351-2.244) | .801 |
| ≥3 | 11 | 5 | 1.336 (0.396-4.510) | .641 |
| Warm-up | ||||
| General (aerobic) | 40 | 21 | 1.481 (0.617-3.556) | .379 |
| Static stretching | 36 | 17 | 1.733 (0.741-4.049) | .204 |
| Dynamic stretching | 43 | 28 | 0.717 (0.260-1.979) | .520 |
| Movement-specific exercises | 40 | 26 | 0.769 (0.300-1.970) | .584 |
| Technique training | 28 | 14 | 1.400 (0.598-3.276) | .438 |
| Joint movements | 4 | 2 | 1.222 (0.212-7.046) | .822 |
| Number of training locations | ||||
| 1 | 17 | 20 | 1 | |
| 2 | 27 | 10 | 3.176 (1.202-8.395) | .020 b |
| 3 | 13 | 4 | 3.824 (1.049-13.953) | .042 b |
| 4 | 1 | 1 | 1.176 (0.068-20.262) | .911 |
a Ref, reference variable.
b Statistically significant; included in multivariate analysis.