
Abstract
Background:
Acute tendon injury can limit motion and thereby inhibit tendon healing. Positive results have been found after the use of platelet-rich plasma (PRP) to treat tendon injury; however, the early effects of PRP on tendon regeneration are not known.
Purpose/Hypothesis:
The purpose of this study was to evaluate the effects of PRP releasate (PRPr) on the early stages of tendon healing in a rat partial tenotomy model. It was hypothesized that PRPr can promote early healing of an Achilles tendon in rats.
Study Design:
Controlled laboratory study.
Methods:
PRP was prepared by a 2-step method of manual platelet concentration from 10 rats. PRPr was isolated from the clotted preparation after activation by thrombin and was applied to an Achilles tendon on 1 side of 30 rats on the second day after partial tenotomy, with normal saline used as the control on the other side. Achilles tendon samples were harvested 5 and 10 days after tenotomy. At each time point, 15 Achilles tendon samples were obtained, of which 5 samples were evaluated by Masson trichrome staining, apoptosis, and cell proliferation, while the other 10 samples were tested for tensile strength using a material testing machine.
Results:
Compared with saline-treated control tendons, the PRPr-treated tendons showed increased collagen synthesis near the cut edge and fewer apoptotic cells (P = .01). An immunohistochemical analysis revealed more Ki-67–positive cells but fewer cluster of differentiation (CD) 68+ (ED1+) macrophages in PRPr tendons compared with saline-treated tendons (P < .01). Tendons treated with PRPr also showed higher ultimate tensile strength than those treated with saline (P = .03).
Conclusion:
PRPr treatment promotes tissue recovery in the early phase of tendon healing by stimulating tendon cell proliferation and collagen production while inhibiting cell apoptosis and CD68+ (ED1+) macrophage infiltration.
Clinical Relevance:
These findings suggest that with PRPr treatment, higher loads can be applied to the healing tendon at an earlier time, which can help the patient resume activity earlier.
Tendon injuries are a common problem among sports participants. In acute tendon injury, partial or complete rupture of the tissue disrupts tissue continuity and ultimately leads to loss of motion, which limits activities and may require cast immobilization. However, the latter has a detrimental effect on tendon healing, 35,37 whereas increased activity has been shown to improve tendon repair in both size and material properties. 48 A similar observation has been made in tendons loaded soon after injury, which improved the longitudinal orientation of cells and matrix. 19 Therefore, to maximize tendon regeneration during the natural healing process, it is imperative to resume activity early on.
Platelet-rich plasma (PRP) contains autologous growth factors and bioactive molecules and has been used for decades to promote tissue healing. 11,30 Platelets are small, nonnucleated bodies in the peripheral blood that function primarily in hemostasis. 1,11 Platelet-derived growth factor, transforming growth factor (TGF)-β, epidermal growth factor, and vascular endothelial growth factor in platelets play key roles in tissue healing. 12,30,32,44 PRP is readily harvested from whole blood via a few centrifugation steps 9,16 and is low cost and safe to use. 11,12,30,44
Recent clinical investigations have shown the successful application of PRP for the treatment of tendon injury. 30,31,39,44 However, these studies have focused on chronic tendinopathy, and it is unclear whether acute tendon injury would benefit from PRP treatment. In acute tendon injury, healing begins with an early influx of inflammatory cells, followed by the formation of fibrovascular interface tissue. 33 As healing proceeds, collagen fibers are generated between ruptured tendons. In contrast, chronic tendinopathy is a degenerative condition or failure of the healing process 24,26 in which fibroblast proliferation and morphology are perturbed and proteoglycan, glycosaminoglycan, and water content along with hypervascularization and collagen fibril disorganization are increased 26 ; moreover, there is no evidence of inflammatory cells in tendinopathic tissue. 43 Therefore, PRP may have different effects in chronic tendinopathy as compared with acute tendon injury.
Clinical research of PRP in the treatment of acute tendon injury has been limited to studies on its use as surgical augmentation for acute Achilles tendon repair 17,51 ; the effects of nonoperative treatment with PRP alone have not been evaluated. Therefore, the present study investigated the effects of PRP on the early phase of tendon healing using a rat model of partial tenotomy of the Achilles tendon. In this experiment, we used PRP releasate (PRPr; a cell-free preparation), which is released from platelets after PRP is activated. It can be stored frozen, so it can be used for continuous applications. It is also suitable for allogeneic purposes, especially for small-animal experiments that need to draw a large amount of blood at the same time. We hypothesized that the healing process of ruptured Achilles tendons of rats and the mechanical strength of healing tendon could be improved by an injection of PRPr.
Methods
All animal use procedures were approved by the Institutional Animal Care and Use Committee of our institution, and all experiments were carried out in accordance with relevant guidelines and regulations. A total of 48 adult Sprague-Dawley rats were used as follows: 10 rats were used for PRP preparation; 30 rats were used for the main experiment, of which 10 were used for the tissue sections and 20 were used for the tensile strength test; and an additional 8 rats were used to test the tensile strength of the Achilles tendon with or without partial tenotomy for reference.
Collection and Preparation of PRPr
Adult Sprague-Dawley rats (n = 10; 250-300 g) were anesthetized, and blood (9 mL) was drawn from the heart into a 10-mL syringe with a 21-gauge needle (BD Biosciences) containing 1 mL anticoagulant (acid citrate dextrose solution) for a total volume of 10 mL. PRP was isolated with a 2-step manual platelet concentration method according to previously described protocols. 47,50 Briefly, sampled blood was centrifuged at 800g for 20 minutes for separation into plasma and red blood cells; the plasma fraction was again centrifuged at 3000g for 20 minutes to separate PRP from platelet-poor plasma. A 1.5-mL volume of PRP was obtained from each 10-mL sample. Isolated PRP was clotted by adding a 10% (vol/vol) thrombin solution (500 U/mL in 100 mM CaCl2) for 1 hour. After another round of centrifugation at 5500g for 15 minutes, releasate of PRP was isolated from the clotted preparation. The final PRPr was filtrated (0.22 μm) and frozen at −80°C. All prepared PRPr was used within 1 month to ensure its best effect. 29
Partial Tenotomy of the Achilles Tendon
A total of 38 adult Sprague-Dawley rats (250-300 g) comprised the experimental model. The animals were anesthetized with 5% isoflurane (Abbott) in an anesthetic chamber, followed by 2.5% to 3.5% isoflurane delivered through a mask. The hair on the skin over the posterior region of both posterior limbs was trimmed. After cleaning the skin with iodized alcohol, a lateral incision was made over each Achilles tendon, which was isolated along with the plantaris from the surrounding fascia. The tendinous portion of the plantaris was removed to prevent it from acting as an internal splint. 4,36,37 An intrasubstance, full-thickness round defect was created with a 2-mm biopsy punch (Miltex) at a point approximately 5 mm from the calcaneal insertion of each tendon. The procedure was performed unilaterally on 8 rats to observe the difference between the tensile strength of the partially incised tendon and the uninjured tendon. The skin incision was then closed with 4-0 monofilament nonabsorbable nylon sutures, and the site of injury was marked on the skin. Rats were kept in a cage unrestricted, and no cast or dressing was applied during recovery.
PRPr Infiltration of Transected Achilles Tendon
Rats were anesthetized on the next day and 0.1 mL PRPr was injected around the Achilles tendon with a 1-mL syringe (BD Biosciences) through the marked skin in 1 posterior limb. In the other posterior limb of each animal, 0.1 mL saline solution was injected as a control.
Tissue Preparation and Histological Analysis
Rats have a high ability to heal. To assess the early process of tendon healing, treated rats were sacrificed 5 or 10 days after treatment with reference to the previous literature. 4,22,48 The Achilles tendon between the calcaneus and the musculotendinous junction was harvested for histological evaluation. Briefly, the tissue was fixed for 1 week in 10% neutral buffered formalin and then embedded in paraffin and cut into 5-µm sections that were mounted on slides and stained with Masson trichrome after deparaffinization. Sections were randomly sampled and 4 histological images per slide were imaged at a magnification of ×200 for morphological assessment.
Biomechanical Testing
Biomechanical testing was carried out as previously described, 4,36,37 with some modifications. The Achilles tendon—including the calcaneus and the gastrocnemius muscle—was harvested 5 or 10 days after injury, wrapped in cotton gauze soaked with balanced salt solution (BSS), and stored in a covered plastic container at −20°C, and experiments were carried out within a week. Gastrocnemius-soleus muscle specimens were thawed at room temperature in BSS 2 hours before testing and mounted onto a tendon clamp 46 such that the distal edge of the clamp was 1.0 cm from the calcaneal insertion. At the distal end of the specimen, the calcaneus was fixed with a clamp positioned at a 45° angle relative to the direction of the applied load. The specimen was kept moist with BSS, and mechanical testing was carried out with a material testing machine (LS Series; Ametek/Lloyd Instruments). The specimen was not preconditioned or cyclically stretched before tensile testing. 4 The Achilles tendon was preloaded to 0.5 N and then pulled at a constant speed of 10 mm/min until failure. A load-time curve was generated. Each specimen was examined for the location of failure, and the proximal grip was inspected to determine whether any of the muscle or tendinous fibers had pulled out from the grip (ie, slippage had occurred) and rule out these conditions. The ultimate failure load was defined as the peak force of the load-time curve.
TUNEL Assay
Tendon sections mounted on slides were deparaffinized, rehydrated, and pretreated with proteinase K (20 μg/mL in 10 mmol Tris [pH 8.0]) for 10 minutes at 37°C. Slides were rinsed 3 times in phosphate-buffered saline (PBS) and incubated with the terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) reaction mixture (BioVision) for 1 hour at 37°C. After washing with PBS, converter-peroxidase solution was applied for 30 minutes at 37°C. After another wash in PBS, the samples were incubated for 5 minutes at ambient temperature with 3,3′-diaminobenzidine and then counterstained with hematoxylin and mounted under glass coverslips. The region close to the cut tendon surface was visualized at ×200 magnification. Three images per slide were acquired and randomly evaluated. Positively and negatively stained nuclei were brown and blue, respectively. The percentage of positive cells was calculated as the ratio of the number of brown-stained to both brown- and blue-stained nuclei.
Immunofluorescence Staining
Tissue sections were deparaffinized and rehydrated. Antigen retrieval was performed with 1 mM EDTA buffer (pH 8.0). Sections were blocked with Blocker FL fluorescent blocking buffer (Thermo Fisher Scientific) for 1 hour. Tissue sections were incubated with anticleaved caspase-3 (Cell Signaling Technology) diluted in antibody diluent (ab64211; Abcam) overnight, and then incubated with anti-rabbit IgG Alexa Fluor 488 (Thermo Fisher Scientific) for 1 hour. After washing with PBS, sections were covered with DAPI (Abcam) in a fixed medium. Six images per slide were randomly acquired under a fluorescence microscope (Eclipse Ni-U; Nikon) at ×200 magnification.
Immunohistochemistry
Paraffin-embedded tendon blocks were cut into 5-µm sections that were deparaffinized, washed, and then blocked with 1% bovine serum albumin and 1% goat serum in PBS. After 3 washes in PBS, sections were incubated for 2 hours with antibodies against Ki-67 (Thermo Fisher Scientific) and cluster of differentiation (CD) 68 (ED1) (Santa Cruz Biotechnology). Immunoreactivity was detected with a streptavidin-biotin labeling system and incubation with diaminobenzidine substrate-chromogen for 5 to 10 minutes. Hematoxylin was used as a nuclear counterstain. Six images per slide were acquired at ×200 magnification and randomly evaluated. Positively and negatively stained nuclei were brown and blue, respectively. The percentage of positive cells was calculated as the ratio of the number of brown-stained to both brown- and blue-stained nuclei.
Statistical Analysis
Data are expressed as mean ± SEM and were analyzed using IBM SPSS Statistics 20 software (IBM Corp). Comparisons between the results of histological data were performed using the Kruskal-Wallis test. Biomechanical data were evaluated with the Student t test. P values <.05 were considered significant.
Results
PRP Preparation Quality
Platelet and white blood cell counts were performed on whole blood and PRP preparations from rats. The number of platelets in acid citrate dextrose–treated whole blood was 1058 ± 41 × 106/mL; the count in PRP was 3.4-fold higher at 3597 ± 251 × 106/mL. The numbers of white blood cells were 4843 ± 611/mL for whole blood and 4037 ± 917/mL for PRP. TGF-β1 and PDGF-BB levels in whole blood and in PRPr were quantified in the first 3 samples. The mean concentrations of the 2 growth factors in PRPr were 129.72 ± 36.63 and 23.21 ± 4.79 ng/mL, respectively, which were 2.6 and 3.8 times higher, respectively, than in whole blood releasate.
Biomechanical Testing
The load failure of the Achilles tendon–calcaneal complex was determined in the uninjured tendon (n = 6), tendon with partial tenotomy (n = 6) (Figure 1A), and saline- and PRPr-treated rats on postoperative days 5 (n = 7 [saline] and n = 8 [PRPr]) and 10 (n = 8 for both groups) (Figure 1B). If the tendon complex slipped in the clamp, then the data were not included in our analysis. The average load at failure of uninjured tendon was 32.9 ± 1.0 N (range, 29.5-35.3 N). A significant decrease of load at failure to 13.3 ± 1.3 N (range, 9.8-17 N; P < .01) occurred in tendon with partial tenotomy. The average load at failure was 15.6 ± 1.1 N (range, 10.4-18.9 N) on day 5 and 31.7 ± 1.4 N (range, 27.9-36.3 N) on day 10 for the saline group, and 20.3 ± 2.0 N (range, 15.2-32.3 N) and 37.2 ± 1.7 N (range, 32-45.7 N), respectively, for the PRPr group. Thus, PRPr increased the maximum force before failure on both days relative to the saline control (P = .03 for both).
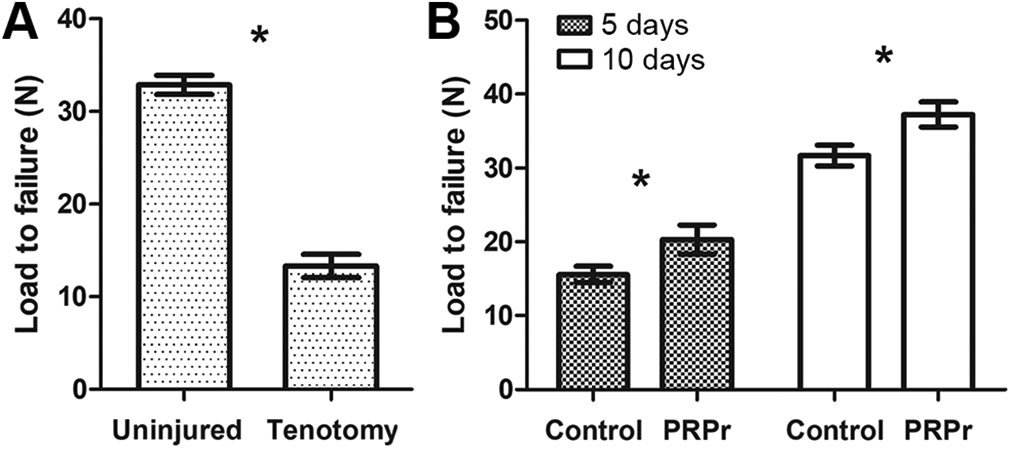
(A) Ultimate failure load required to induce rupture of uninjured rat Achilles tendons (load at failure) and tendons with partial tenotomy (n = 6). *P < .05. (B) Tendons treated with PRPr show higher load at failure than saline-treated controls on postoperative days 5 (n = 8) and 10 (n = 8). *P < .05. PRPr, platelet-rich plasma releasate.
Histological Analysis
Histological evaluation of tendon specimens harvested 5 days after injury showed evidence of an inflammatory response. Both PRPr- and saline-treated tendons showed increased cellularity, with a mix of spindle-shaped fibroblasts and mononuclear cells. A region of fibrous connective tissue was observed at the site of cutting. In specimens from the PRPr group, fibroblast orientation was less random and there was more collagen matrix between the cells than in controls (Figure 2). By postoperative day 10, the inflammatory response had abated. Both PRPr- and saline-treated tendons showed little cell infiltration; however, collagen fibers were more abundant in the PRPr group with traces of newly formed tendon fibers.

Histological analysis of tendon tissue from rats with Achilles tendon injury. Representative photomicrographs are shown of a longitudinal section of the Achilles tendon excluding the intact margin fiber in the left lower corner, stained with Masson trichrome from rats treated with saline as a control (left) and PRPr (right) at 5 and 10 days after injury (×200 magnification). PRPr, platelet-rich plasma releasate.
Cell Apoptosis Analysis
The TUNEL assay was used to evaluate cell apoptosis in the injured tendon after treatment with saline or PRPr (Figure 3, A and B). Saline-treated tendons showed more TUNEL-positive cells than PRPr-treated tendons during the first 5 days after the operation (32.0% ± 2.0% vs 14.8% ± 0.9%; P < .01). On day 10, there was no difference between the 2 groups (9.8% ± 0.4% vs 8.0% ± 2.0%; P = .43). Although the TUNEL assay is very sensitive and widely used, it has limitations. 10 Therefore, we used cleaved caspase-3 immunofluorescence staining (a more specific and reliable method) to identify and quantify apoptotic cells in tissue sections. On the fifth day, the caspase-3–positive cell of the PRP-treated tendon was reduced by 42.2% compared with the control group (P = .01). These results indicate that PRPr inhibits cell apoptosis at the early stage of tendon healing.

Apoptosis in injured tendon tissue as determined by the TUNEL assay and caspase-3 immunofluorescence staining. (A) TUNEL-positive tendon cells (brown nuclei) were counted in tendons treated with saline (controls) and PRPr 5 and 10 days postinjury. (B) Fewer positive cells were observed in the PRPr as compared with the control group on day 5 (n = 3). *P < .05. (C) Representative sections of cleaved caspase-3 immunofluorescence staining on day 5. (D) Fewer positive cells were observed in the PRPr as compared with the control group (n = 3). *P < .05. PRPr, platelet-rich plasma releasate; TUNEL, terminal deoxynucleotidyl transferase dUTP nick end labeling.
Immunohistochemical Analysis of Ki-67 and CD68
The fraction of Ki-67–positive cells was higher in PRPr-treated as compared with control tendons on day 5 (48.5% ± 2.8% vs 17.4% ± 1.8%; P < .01) (Figure 4). On day 10, both PRPr and saline groups showed a significant reduction in Ki-67 immunoreactivity (28.1% ± 2.3% and 25.1% ± 0.7%, respectively; P = .28), with no difference between the 2 groups. ED1+ macrophages were detected by anti-CD68 antibody labeling (Figure 5); the fraction of ED1+ macrophages was higher in the saline as compared with the PRPr group (48.3% ± 2.3% vs 27.4% ± 0.6%; P < .01). On day 10 postinjury, the percentage of ED1+ macrophages was reduced in both groups (14.2% ± 0.7% for saline and 12.0% ± 1.2% for PRPr), with no difference between them (P = .20).

Cell proliferation in injured tendon tissue. (A) Representative images of rat Achilles tendon with Ki-67 immunoreactivity (brown nuclei). (B) Quantitative analysis of Ki-67–positive nuclei in injured tendon. More positive cells were observed in the PRPr (right) as compared with the saline (left) group on day 5 postinjury (n = 3). There was no difference between groups in the number of Ki-67–positive cells on day 10 postinjury. *P < .05. PRPr, platelet-rich plasma releasate.

Macrophage infiltration in injured tendon tissue. (A) Representative sections of CD68 (ED1) immunoreactivity (brown staining) in the Achilles tendon. (B) Fewer CD68+ (ED1+) macrophages were detected in tissue samples from the PRPr (right) as compared with the saline control (left) group 5 days postinjury; there was no difference between groups on day 10 (n = 3). *P < .05. CD, cluster of differentiation; PRPr, platelet-rich plasma releasate.
Discussion
The present study found that PRPr application in a rat model of Achilles tendon injury improved tissue repair and functional recovery in the early phase of healing. Previous studies have shown that early mobilization of the injured tendon accelerates the restoration of function 40 —for instance, breaking strength increases with motion and tension 23 ; however, the major concern with early motion after Achilles tendon injury is that it could increase tension in the tendon across the tear site, which could in turn cause stretching of the tissue and possible rupture during healing. Our results suggest that PRPr treatment is a promising strategy for the early treatment of Achilles tendon injury that can improve tensile strength in the tendon so that it can better respond to mechanical loading and allow activity to resume at an earlier time point. This may be beneficial in the clinical setting regarding rehabilitation of a tendon injury. Earlier weightbearing and mobilization are associated with fewer adhesions, increased postoperative range of motion, earlier return to activity, and greater patient satisfaction. 25
The biomechanical properties of the tendon are mostly attributed to the extracellular matrix and collagen, which constitute around 60% of dry mass of the tissue in tendons. 42 A higher collagen content increases the tensile strength of tendon, 13,34,45 while the number of tendon fibroblasts is closely related to collagen production. 8 Thus, for improved material properties, the tendon requires a sufficient number of fibroblasts and a matrix capable of transferring load. Many studies have shown that PRP enhances tenocyte proliferation and total collagen production in vitro 8,12,50 ; our immunohistochemical and histological analysis demonstrated that it also exerts these effects in vivo.
Thus far, a great number of PRP investigations have been devoted to studying the proliferation of tenocytes, whereas cellular apoptosis remains poorly understand. Apoptosis is an active and genetically controlled process of cell death initiated in cells exposed to cytotoxic stress. Acute trauma in the tendon can induce apoptosis of tenocytes in a poorly vascularized environment. The rate of tenocyte apoptosis was found to be highest in the first week after acute tendon transection. 49 Platelets promote cell survival and tissue repair by secreting antiapoptotic factors such as hepatocyte and stromal cell-derived growth factors, serotonin, and adenosine diphosphate. 15 The results of the present study show that PRPr exerts antiapoptotic effects in the injured tendon, although further study is needed to clarify the underlying mechanism.
After tendon injury, activated leukocytes within the blood clot release growth factors and cytokines to initiate the inflammatory response, which contributes to the progression of tendon degeneration 41 ; 24 h postinjury, macrophages become the predominant cell type and persist until the end of the inflammatory response. 27 However, inflammatory cytokines inhibit fibroblast proliferation and degrade the extracellular matrix 14 ; indeed, recent studies suggest that a persistent inflammatory response impairs healing. 2 Moreover, macrophage depletion has been shown to accelerate tissue healing 7 and improve the biomechanical properties of the ligament in a reconstruction model. 18 CD68 (ED1) is expressed by blood monocytes and exudative macrophages, and upregulation of this protein reflects increased lysosomal activity. 20 ED1+ macrophages are prominent between 1 and 5 days postinjury, 21 that is, during the inflammatory phase of wound healing. Macrophages secrete many inflammatory cytokines (eg, interleukin-1 and tumor necrosis factor [TNF]-α) that inhibit tendon cell proliferation and degrade the extracellular matrix 14 ; previous studies have suggested that ED1+ macrophages release molecules that stimulate tendon catabolism. 27,28 In addition, upregulation of TNF-α is associated with apoptosis. 41 Taken together with our findings, PRP dampened down the ED1+ macrophage–related inflammation just enough to create an ideal tendon healing environment that may contribute to tendon cell proliferation and inhibit cell apoptosis and collagen degradation.
The effects of PRP to augment healing in Achilles tendon ruptures have been promising in preclinical models. The majority of studies performed mechanical tests and calculated histological scores. Several in vivo studies have reported that a PRP-treated tendon healed at an early time point with better organization of fibroblasts and collagen bundles. 6,22,38 Studies that observed tensile strength and mechanical properties also found increased load to failure in the PRP-treated group, indicating an increased rate of repair. 3,22,48 However, the timing of these studies varies greatly, ranging from 3 days to 1 month. Our results reinforce these in vivo observations that a single injection of PRPr in ruptured rat Achilles tendon enhances the early phase of healing within 5 days. In addition, to the best of our knowledge, this is the first study to prove that PRPr can be associated with anti-inflammatory and reduced apoptosis in vivo, thereby enhancing tendon healing. Tendon healing comprises 3 phases: inflammation, cell proliferation, and tissue maturation. 5 An early event during healing is inflammation, in which new vasculature delivers inflammatory cells and tendon fibroblasts to the injury site, consequently increasing cellularity. 19 Therefore, it is very important to understand the impact of PRPr on inflammation in the early stage of tendon repair.
This study has several limitations. The first is that findings from a rat model may not be similar to tendon injury in humans because of the difference in the size of the tendons between species, which has significant effects in diffusion and cellular migration distances. Furthermore, rats tend to load their healing Achilles tendons to a greater extent than humans. In addition, our Achilles tendon ruptured model surgically created an acute lesion in the tendon, and the lesions were immediately treated with PRPr. Clinically, however, tears in chronic tendon pathologies are more common, and even acute injuries may present days to weeks after the initial trauma. Future in vivo research on PRPr and chronic tendon pathologies is warranted. Second, additional experiments must be carried out to determine whether PRPr accelerates tendon healing in the later stages. Finally, the relationship between inflammation and a clinically meaningful outcome such as reduced pain requires investigation in human trials.
Conclusion
PRPr treatment improved the ultimate tensile strength of the injured tendon in the early phase of healing, which was associated with increased tendon cell proliferation and collagen production, and reduced cell apoptosis and inflammatory cell infiltration at the site of injury. These findings can inform the development of effective therapeutic strategies based on PRP in acute tendon injury.
Footnotes
Final revision submitted August 27, 2020; accepted September 30, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study received funding from the Chang Gung Memorial Hospital, Taoyuan City (CMRPG3C1361). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Chang Gung University Institutional Animal Care and Use Committee (approval No. CGU13-044).