
Abstract
Background:
Autologous fascia lata (AFL) graft use in arthroscopic superior capsular reconstruction (ASCR) is effective for the treatment of irreparable rotator cuff tears (RCTs). Although donor-site morbidity (DSM) is a recurrent argument against AFL graft use, scientific evidence for this argument is lacking.
Purpose:
To report the midterm clinical follow-up evaluation of DSM in ASCR using minimally invasively harvested AFL grafts and compare thigh function and patient satisfaction with those of an unharvested control group.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Of 66 consecutive patients who underwent ASCR using a minimally invasively harvested AFL graft, 39 patients with a minimum follow-up of 24 months were retrospectively evaluated (ASCR group) and compared with 39 randomly selected patients who underwent arthroscopic RCT repair by the same surgeons (control group). The functional outcomes of both thighs were evaluated using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). Patient satisfaction was evaluated using the Patient Scar Assessment Questionnaire (PSAQ) and a subjective questionnaire. Pain was quantified using a visual analog scale (VAS).
Results:
The ASCR group had a mean age of 65 years (range, 51-77 years) and a mean follow-up of 47 months (range, 24-66 months). The WOMAC score in the harvested thigh differed by 0.8% from that in the contralateral thigh (P = .002). The mean PSAQ score differed by 6 points from the minimum PSAQ score (P < .001). Overall, 95% of the patients indicated that they would undergo the same surgery again and that the shoulder outcome compensated for the thigh symptoms. There was no significant association between the presence of residual thigh symptoms and the willingness to undergo the same surgery again (P = .354). The mean VAS score in the harvested thigh was 0.6 (range, 0-5). There was no significant difference in the average WOMAC score or VAS score between groups (P = .684 and P = .148, respectively).
Conclusion:
Despite the proportion of residual symptoms, the associated functional effects were small and not clinically significant, and the vast majority of patients were accepting of the harvest symptoms given the improvement in shoulder function.
Superior capsular reconstruction (SCR) was first described in 1993, in a study by Hanada et al, 19 for the treatment of a recurrent posterosuperior rotator cuff tear (RCT) in a patient with paraplegia. Twenty years later, Mihata et al 32 reported the first groundbreaking clinical results of arthroscopic SCR (ASCR) in irreparable posterosuperior RCTs using an autologous fascia lata (AFL) graft. ASCR has been rapidly popularized worldwide in an attempt to reproduce promising clinical results and fill a gap in the RCT treatment algorithm.
In SCR, the main role of the graft is to work as a fulcrum to the deltoid ascending force vector in the first degrees of forward flexion and abduction in the scapular plane, reestablishing the glenohumeral vertical force couple. The chosen graft must be able to counteract the deltoid force, maintaining the joint center of rotation, without losing its integrity throughout the shoulder range of motion. The ideal viscoelastic properties and position of fixation of the graft remain to be determined.
Fascia lata is a complex layer of fibrous tissue, composed of highly oriented collagen and elastin fibers that are connected by an extracellular matrix composed of proteoglycans. During hip and knee movements, the fascia lata tissue sustains high strains in multiple directions, and its resistance and elasticity make it an attractive and versatile autograft. 37,43 When harvested postmortem, the fascia lata loses a large percentage of its proteoglycans, which has an effect on its viscoelastic properties, 43 highlighting the importance of in vivo AFL harvesting.
Concerns about AFL harvesting time and donor-site morbidity (DSM) arose in the international orthopaedic community, and off-the-shelf graft options were proposed as an alternative. Despite the increase in the total cost of the procedure, and the initial lack of biomechanical or clinical studies documenting the efficacy of these alternative grafts, they were widely adopted, removing the need to harvest an autograft and reducing the theoretical resultant DSM. In the past 8 years, several biomechanical and clinical studies of SCR using off-the-shelf allografts or xenografts have been published. #
Because of the inconsistent results obtained with off-the-shelf grafts and to avoid AFL harvesting time and DSM, other authors have proposed ASCR techniques using the long head of the biceps tendon (LHBT). 5,6,18,27 Barth and colleagues 5 reported the clinical results using LHBT, at a minimum 2-year follow-up, with improved active range of motion and patient-reported outcome measures (PROMs). An ultrasound-controlled graft tear rate of 8.3% at 12 months of follow-up was reported, but magnetic resonance imaging (MRI) was not used. In their 2-year follow-up study of ASCR using AFL for the treatment of irreparable posterosuperior RCTs, de Campos Azevedo et al 10 found that 50% of the patients had an absent LHBT at the time of surgery, suggesting that this local autograft alternative may be an inconsistent graft type choice for the treatment of such a condition.
In ASCR, as in any other graft-dependent surgery, DSM remains an important factor when choosing an alternative graft type, even though scientific evidence on DSM is lacking and even though, historically in orthopaedic surgery, the use of an autograft has produced better and more permanent results than xenografts or allografts; this has been extensively studied in knee surgery. 4,23,33,52
The AFL graft used by Mihata et al 32 was harvested through a longitudinal incision over the proximal lateral thigh, with the aim of harvesting a part of the tensor fascia lata, including the septum attached to the greater trochanter. In the present study, we harvested a biomechanically equivalent AFL graft using a minimally invasive technique that spares the tensor fascia lata and the iliotibial band. 2,10,11 The purpose of this study was to report the midterm clinical follow-up evaluation of DSM in ASCR using AFL grafts harvested with this minimally invasive technique and to compare thigh function and patient satisfaction with results from a control group. The hypothesis was that the AFL graft would not produce significant DSM and that the improvement in shoulder function would outweigh any residual symptoms in the thigh.
Methods
Study Design
The study protocol was approved by the ethics review board of our institution. A comparative study of the thighs of consecutive patients who underwent ASCR performed by 2 experienced shoulder surgeons (A.C.L.P.G.A. and C.I.d.C.A.) was designed to compare thigh function and patient satisfaction using a control group of patients who underwent arthroscopic RCT repair by the same surgeons. Patients who underwent ASCR between 2015 and 2021 were included in the ASCR group, and the control group of patients was randomly selected from the database of patients who underwent arthroscopic RCT repair by the same surgeons between 2018 and 2021. Patients who had less than 24 months of follow-up, had sustained subsequent injuries to either of the lower limbs, or had died were excluded.
The harvested thighs in the ASCR group were retrospectively evaluated for PROM scores, cosmesis, subjective satisfaction, and residual symptoms. The contralateral thighs in the ASCR group and the thighs in the control group were evaluated utilizing PROMs. The average PROM scores of the 2 thighs of the patients in the control group were calculated and compared with the scores of the harvested thighs in the ASCR group.
Patient Evaluation
Each patient was assessed by an experienced shoulder surgeon (A.C.L.P.G.A.). Functional outcomes were assessed in the thighs with the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC; range, 0-100), and thigh pain was quantified using a visual analog scale (VAS; range, 0 [no pain] to 10 [worst pain]). In the harvested thighs, patient satisfaction and cosmesis were evaluated using the 39-item Patient Scar Assessment Questionnaire (PSAQ; range, 39-158), which comprises 5 subscales: cosmetic appearance, symptoms, consciousness, satisfaction with appearance, and satisfaction with symptoms. The mean total PSAQ score and the mean score for each subscale were compared with the minimum score value (no scar) for each item.
Each of the patients in the ASCR group answered a satisfaction questionnaire regarding the harvested thigh that included the following dichotomous questions: (1) Do you have residual thigh symptoms?, (2) Does the thigh still bother you?, (3) Do you consider the thigh symptoms to be compensated for by the outcome obtained in the shoulder?, and (4) Would you undergo the same surgical procedure again? Patients with residual symptoms were asked to specify what their symptoms were (pain, numbness, local herniation, and/or claudication). Age, sex, professional activity type (manual/administrative), and professional status (active/retired) were evaluated and compared between groups.
A subgroup analysis of the ASCR group according to the presence or absence of residual symptoms in the harvested thigh was conducted. The primary predefined outcome measures were the WOMAC, PSAQ, and VAS scores. The secondary outcome measures were the responses to the satisfaction questionnaire.
Surgical Technique
The AFL was harvested from 1 thigh of each patient in the ASCR group using the minimally invasive technique that has been previously described in the literature 2,10 (Figure 1) through 2 transverse 2-cm cutaneous incisions. Each midthigh graft was harvested 15 cm distal to the anterosuperior iliac spine, 10 cm proximal to the lateral femoral epicondyle, and 4 cm anterior to the lateral femoral intermuscular septum and was typically 150 × 35 mm in the longitudinal × transverse directions. The intermuscular septum was not included in the harvest. After the percutaneous harvesting of the AFL, each patient was instructed to maintain a compressive dressing for 48 hours and wear a compressive stocking for at least 6 weeks. During this period, vigorous activities involving the lower limbs were discouraged. No specific rehabilitation program was followed, and full weightbearing on the harvested thigh was immediately allowed.
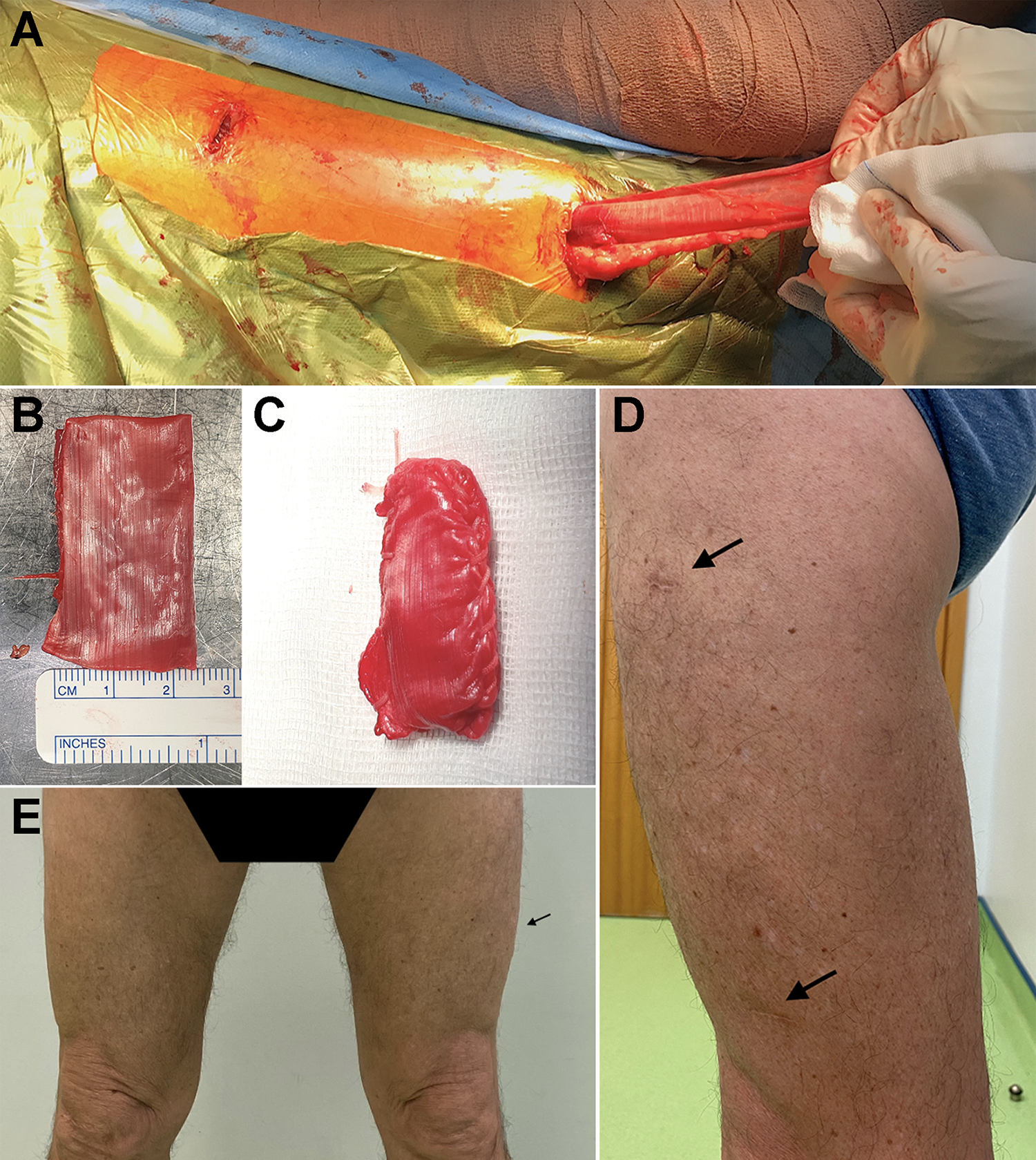
(A) The autologous fascia lata percutaneously harvested from a left thigh through the proximal 2-cm transverse skin incision using the minimally invasive harvesting technique in the beach-chair position. (B, C) The prepared and folded fascia lata graft before and after peripheral suturing, according to the original technique. 2,10 (D, E) Pictures of the left thigh of patient 38 at the 3-year follow-up evaluation showing the scars in frontal and side views (arrows).
Statistical Analysis
The Pearson chi-square and Fisher exact tests were used to analyze the categorical variables. Shapiro-Wilks and Kolmogorov-Smirnov tests were used for normality testing of the continuous variables. When comparing variables in the same group, the paired-samples t test was used to compare normally distributed variables, and the Wilcoxon signed-rank test was used to compare nonnormally distributed variables. When comparing variables between the 2 groups, the independent 2-tailed t test and the Mann-Whitney U test were used for normally and non-normally distributed variables, respectively.
For the a priori power analysis, the chosen variable was the WOMAC score. The independent 2-tailed t test was used for the sample size calculation, and the study was designed to achieve a power of 90% (beta = 0.100) at a significance level of P < .05 (alpha = 0.05) with a Cohen d effect size of 0.8 and an allocation ratio of n2/n1 = 1. The numbers of patients required to show a difference between groups were n1 = 34 and n2 = 34; therefore, the minimum total sample size determined for the current study was n = 68. For the post hoc power analysis of the subgroups with or without symptoms, the chosen variable was the WOMAC score and the independent 2-tailed t test was used to compute the achieved power, given an alpha of 0.05, with a Cohen d effect size of 0.5. G*Power 3.1.9.6 for Mac OS 14 was used for the power analysis, and SPSS Statistics Version 27 (IBM) was used for the statistical analysis, with the statistical significance level set at P < .05.
Results
Study Population
A total of 66 consecutive patients who underwent ASCR between 2015 and 2021 were identified. Twenty patients who had less than 24 months of follow-up; 6 patients who experienced subsequent injuries to either of the lower limbs, unrelated to the harvesting procedure; and 1 patient who had died were excluded. Therefore, 39 patients (78 thighs) were included in the ASCR group. Thirty-nine patients who underwent arthroscopic RCT repair by the same surgeons between 2018 and 2021 (78 unharvested thighs) were included in the control group.
Characteristics of the Study Population
A total of 156 thighs (78 patients) were evaluated. In the ASCR group, 59% of the patients were women and 41% were men. The mean age was 65 years (range, 51-77 years), and the mean follow-up time was 47 months (range, 24-66 months). Seventy-seven percent of the patients who underwent AFL harvesting performed manual professional activity, and 54% were retired at the time of the evaluation. As shown in Table 1, there was no significant difference between the ASCR and control groups regarding sex (P = .09), professional activity type (P = .21), or professional status (P = .11), but the average age significantly differed between groups (P = .003), with the control group being younger.
Characteristics and PROMs of the Study Population a

a Data are presented as means unless otherwise indicated. ASCR, arthroscopic superior capsular reconstruction; NA, not applicable; PROM, patient-reported outcome measure; PSAQ, Patient Scar Assessment Questionnaire; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Arthritis Index.
b Minimum PSAQ value (no scar).
c Presented values for PROMs are the mean value between the score in the 2 thighs in the control cohort.
d Value obtained when comparing the control group with the harvested thigh in the ASCR group.
PROM and Satisfaction Scores
As shown in Table 1, the average WOMAC score significantly differed by 0.7 points between the harvested and contralateral thighs (P = .002), and the 2 scores were strongly correlated (r = 1). The average total PSAQ score differed from the minimum PSAQ score (no scar) by 6 points (P < .001). There was no significant association between the presence of residual thigh symptoms and the willingness to undergo the same surgical procedure again (P = .354). The WOMAC score in the harvested thigh was lower in patients with donor-site residual pain (P < .001), and no other specified symptom was significantly correlated with this score. Female sex correlated with a positive response to the question “Does the harvested thigh bother you?” (P = .04) but not to the questions “Do you have pain?” (P = .07), “Do you have symptoms in the harvested thigh?” (P = .4), and “Would you undergo the same surgery again?” (P = .136). When comparing the ASCR and control cohorts, there was no significant difference in the mean WOMAC score (P = .684) or mean VAS score (P = .148).
Every patient in the ASCR group answered the dichotomous questionnaire, and 51% reported the presence of residual thigh symptoms (Table 2). Of the 39 patients, 37 (95%) reported that they would undergo the same surgery again and considered that the postoperative shoulder outcome compensated for the residual thigh symptoms, shown in Table 3. Twenty-three percent of the patients reported that the thigh still bothered them, and of these, 89% said that they would undergo the same surgical procedure again. Regarding the harvested thigh, 94.9% of the patients reported a VAS score of 3 or less, with a mean score of 0.6 (range, 0-5).
Harvested Thigh Symptoms in the ASCR Group as Assessed by the Subjective Satisfaction Dichotomous Questionnaire a

a ASCR, arthroscopic superior capsular reconstruction.
Subgroup Analysis According to the Presence or Absence of Residual Symptoms in the Harvested Thigh a

a ASCR, arthroscopic superior capsular reconstruction; PSAQ, Patient Scar Assessment Questionnaire; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Arthritis Index.
Subgroup Analysis on the Residual Thigh Symptoms in the ASCR Group
As shown in Table 3, the willingness to undergo the same procedure again or the subjective feeling of the benefit of the final result obtained in the shoulder outweighing the residual thigh symptoms did not significantly differ between the subgroups with or without residual thigh symptoms. The average WOMAC, PSAQ, and VAS scores did not significantly differ between the 2 subgroups. Of the patients who reported residual thigh symptoms, 55% reported that the thigh did not bother them, and 90% reported that the shoulder outcome compensated for the thigh symptoms and would undergo the same surgery again. The achieved power for this subgroup analysis was 33%.
Discussion
The main findings of this study were that despite minor donor-site symptoms being present in over half of the patients, 95% of the harvested patients were willing to undergo the same surgery again and considered that the postoperative shoulder outcome compensated for the residual thigh symptoms. Additionally, there were no considerable differences between the ASCR and control groups in the results of the PROMs.
The average WOMAC score differed by 0.8 points between the harvested and contralateral (unharvested) thighs. This average value, although statistically significant, is considerably below the minimal clinically important difference (MCID) and minimally important change (MIC) in the average WOMAC score reported in the literature for patients who have undergone total hip replacement (21.5 and 29, respectively). 40,48 This score, widely used for the evaluation of hip and knee osteoarthritis, was selected by us to address each residual symptom that could result from the AFL harvesting. The only residual symptom that significantly correlated with a lower average WOMAC score was pain. Nevertheless, 94.5% of these patients had a VAS score ≤3, which is the threshold value for which pain is considered clinically significant. 34,47
Regarding the PSAQ score, there was a significant difference between both the harvested and contralateral thighs, and the harvested and control groups. Despite being significant, this difference was quantitatively small and represented a limited percentage of the total score. This significance probably relates to the fact that both in the unharvested thigh and in the control group, the values obtained for the PSAQ were consistently the same (the lowest result possible), considering that none of these patients had a scar in the evaluated anatomic segment. There is no published MCID or MIC for PSAQ; therefore, the clinical importance of this statistically significant difference is unknown.
Twenty of the harvested patients reported having residual donor-site symptoms, which represents half of the total harvested cohort and can be considered a high proportion of residual symptoms. To determine the real impact of the presence of these residual symptoms on donor-site function and subjective satisfaction, a subgroup analysis was conducted comparing the average PROMs and the subjective satisfaction between the patients who reported residual thigh symptoms and those who did not. The average PROMs and subjective satisfaction were not significantly different between the 2 subgroups, suggesting that a high proportion of residual symptoms did not equate with a significantly high morbidity and should be interpreted with caution. Additionally, 90% of the patients reporting residual donor-site symptoms considered the results obtained in the shoulder to compensate for the symptoms. This supports the hypothesis that the minimally invasively harvested AFL graft did not produce significant DSM and that the results obtained in the shoulder compensated for the residual changes in the thigh in the vast majority of the patients.
DSM is a certainty when autologous tissue is harvested. The questions that should be addressed are whether DSM is clinically significant, whether its disadvantages are outweighed by the benefits of the results obtained in the main surgical procedure (ASCR), and whether these results can be reproduced by off-the-shelf graft types. To date, clinical studies of ASCR that used AFL have reported an MRI-based graft tear proportion ranging from 0% to 41% at a minimum follow-up of 6 months to 5 years. Eight of these 9 studies reported a revision rate of 4% or less. ** In contrast, of the 16 clinical studies of ASCR that used allografts or xenografts published to date that reported a minimum follow-up of 6 months to 2 years, †† only 4 studies 13,29,41,50 reported an MRI evaluation of graft integrity for each of the enrolled patients, and the calculated graft tear proportion ranged from 18.5% to 50% in the first 6 to 12 months of follow-up. In the remaining 12 studies of ASCR that used allografts or xenografts, a selected subgroup of patients underwent MRI evaluation, resulting in a proportion that reflects only this selected subgroup’s graft tear rate. Therefore, no off-the-shelf graft has been shown to be able to reproduce the imaging results that were obtained using AFL. 26 Systematic reviews could not compare clinical outcomes between different types of grafts and highlighted the heterogeneity among the studies. 9,22,30,42,45,51
The good results of ASCR that uses AFL come with a price: the additional harvesting procedure and the resultant residual symptoms. According to the current study, 95% of the patients considered the price to be fair and would be willing to undergo the procedure again. Historically, graft-dependent surgeries have always led to a dilemma between graft survivorship and DSM. Ideally, to mimic or replace organic tissue, the chosen graft should be biocompatible and possess viscoelastic properties similar to those of the native tissue. In this line of thought, autologous tissue is a reliable, versatile, and highly available option that produces consistent results. Autologous iliac crest bone, fascia lata, hamstrings, and palmaris longus are a few examples of autografts commonly used in orthopaedic surgery with excellent long-term results that are hardly replicated by allografts, xenografts, or synthetic grafts. Despite DSM, autografts continue to be an option and, in most cases, the first option. Nevertheless, it is important to acknowledge that if similar clinical and imaging results can be obtained with an off-the-shelf graft, it might be preferable, as it avoids any possible donor-site symptoms.
Harvesting AFL utilizing the minimally invasive technique is designed to spare the tensor fascia lata and iliotibial band and aims to minimize the functional damage to the adjacent hip and knee joints, which may have contributed to the observed low morbidity in this study. Therefore, this result cannot be extrapolated to other harvesting techniques. The surgeon must consider and value the morbidity of the main surgical procedure itself, which is ASCR. The choice of a type of graft that has a higher tear rate, or an unknown or unreported tear rate, to avoid DSM must take into account that the failure of the main surgical procedure will compromise the final outcome in each patient, regardless of the type of revision options that can be utilized afterward. 8,21,44
Limitations and Strengths
The current study has some limitations. The study was retrospectively designed and included an unmatched control group whose average age significantly differed from that of the ASCR group. Nevertheless, the average age was lower in the control group, which means that the ASCR group epidemiologically had a higher probability of hip or knee degenerative diseases that could translate into worse PROM scores. The surgeon who performed the outcome assessment was not blinded with regard to the patients’ allocation, and this may have biased the results. The subgroup analysis was underpowered, suggesting that a larger sample size was needed to achieve adequate power for this particular analysis. Nevertheless, the emphasis of the discussion remained on the results obtained from the total study sample.
The current study has some strengths. First, the ASCR group had a minimum follow-up of 2 years, and the study was adequately powered to objectively determine DSM after AFL harvesting in ASCR. Second, to the best of our knowledge, this is the first study to compare the harvested thighs both to the contralateral thighs of the same patients and to the thighs of a control group of patients who did not undergo AFL harvesting, thus contributing new and valuable information to assist surgeons in the choice of type of graft, harvest location, and technique in ASCR.
Conclusion
Despite the proportion of residual symptoms, the associated functional effects were small and not clinically significant, and the vast majority of patients were accepting of the harvest symptoms given the improvement in shoulder function. The minor morbidity of AFL harvest should be discussed with patients before performing an ASCR.
Footnotes
Final revision submitted November 1, 2021; accepted November 8, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.C.L.P.G.A. and C.I.d.C.A. have received consulting fees from ConMed. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Centro Hospitalar de Lisboa Ocidental (ref. No. 20170700050).