
Abstract
Background:
Untreated or residual developmental dysplasia of the hip may cause significant morbidity. Periacetabular osteotomy (PAO) allows for surgical reorientation of the acetabulum but requires a significant recovery period. Because of the physical demands of active military service, hip dysplasia or its treatment with PAO may cause a significant impact on the careers of affected personnel.
Purpose:
To measure the impact of symptomatic acetabular dysplasia and its treatment with PAO on the physical readiness of personnel in the United States Armed Forces.
Study Design:
Case series; Level of evidence, 4.
Methods:
Records from an interservice hip-preservation practice were reviewed for all patients who underwent PAO while on active duty from January 2014 through April 2017. Collected information included branch of service, military occupation, preoperative duty restrictions related to the hip, and concomitant surgical procedures. Patients were evaluated for a minimum of 24 months and assessed for their time to return to duty, continued duty restrictions, and referrals to the medical evaluation board.
Results:
Twenty patients (15 female, 5 male) underwent a PAO while on active duty during the period assessed. The mean patient age at surgery was 25.9 years, and the mean follow-up was 3.3 years (range, 2.3-5.4 years). In the 6 months preceding surgery, 94% of the 17 patients with available records were on duty restrictions specific to their hip (14 temporary, 2 permanent). After PAO, 35% of patients (n = 7) returned to full duty and 85% were able to remain on active duty (n = 12) or complete their military service commitments (n = 5) without noted medical disability. Three patients were medically discharged after PAO, with 1 patient referred due to hip pathology.
Conclusion:
Acetabular dysplasia significantly affects physical readiness in affected servicemembers, with 94% requiring duty restrictions. PAO allowed 85% of patients to return to military service, and 1 in 3 were able to return to full duty.
The concentric development of the acetabulum and proximal femur is essential for the optimal function and long-term viability of the hip joint. Developmental dysplasia of the hip (DDH) demonstrates a variable spectrum of expression; some patients demonstrate gross instability during infancy, while others remain asymptomatic for decades with radiographically mild dysmorphic features. 12,23 Despite serial childhood screening examinations by pediatricians, many patients with mild dysplasia do not become symptomatic until the second or third decade of life when they are evaluated for pain about the hip. 22 These patients often have significant physical activity demands and are entering the formative years of their working life. 16,22 As dysplasia is a known risk factor for premature osteoarthritis of the hip, periacetabular osteotomy (PAO) has emerged as a tool to correct acetabular pathoanatomy and better distribute joint reactive forces across the hip. 8,9,12,13,27 For this reason, the initial focus of PAO literature has been the survivorship offered before total hip arthroplasty. 15,26,28 However, as our awareness and diagnostic abilities have improved, the long-sighted nature of this endpoint overlooks the short- and medium-term impacts of this procedure on the young, active patients in whom DDH is often first recognized.
Military service requires a high level of physical fitness and places significant emphasis on operational readiness. While the specific tasks and physical demands vary according to a servicemember’s occupation within the military, all personnel are required to maintain a baseline level of physical fitness. In the United States, this physical readiness is assessed semiannually through tests of body composition, aerobic endurance, and muscular fitness. The specific events and passing requirements of these fitness assessments are unique to each branch of service, but most include a timed run of 1.5 to 3 miles (2.4-4.8 km), sit-ups, push-ups, and pull-ups. Personnel unable to complete these assessments due to injury or illness may be granted temporary duty restriction (TDR; or “temporary profile” or “limited duty”) by a medical professional to permit recovery. Depending on the branch of service, personnel with conditions that are unlikely to resolve may be granted permanent duty restriction (PDR; or “permanent profile”) to allow for modification of their future fitness assessments or occupation-specific tasks.
If the condition is deemed to render the servicemember unfit to continue service in his or her current occupation, a review by the medical evaluation board (MEB) may be recommended by a health care professional. After a comprehensive evaluation, the MEB may make a number of recommendations, which most often entail retention on active duty in full capacity, retention on active duty with permanent duty modifications (ie, PDR), or medical discharge from service. For those individuals medically discharged from service, the MEB also assigns a disability percentage rating (0%-100%) per unfitting condition, according to a system utilized by the US Department of Veterans Affairs (VA).
Given the natural history of hip dysplasia, the implications of its treatment are particularly relevant to afflicted military servicemembers. The purpose of this study was to assess the impact of acetabular dysplasia and its treatment with PAO on the careers of active-duty US military servicemembers.
Methods
After approval by our institutional review board, the institution’s surgery scheduling system (S3) was queried for patients who underwent a PAO performed in a military interservice hip-preservation practice from its inception in January 2014 through April 2017. All procedures were performed by a single surgeon (M.R.S.). Patients were excluded if they were not on active-duty US military service at the time of surgery, were referred for MEB before evaluation by the treating surgeon, had radiographic evidence of osteoarthritis (Tönnis grade ≥1), or lacked a minimum of 2 years of follow-up.
Based on the nature of the practice, active-duty patients were referred by orthopaedic surgeons at military treatment facilities throughout the world. The radiographic evaluation consisted of an anteroposterior pelvis, false-profile views, Dunn lateral views, and computed tomography of the pelvis and proximal femur with 3-dimensional reconstruction. Patients with appropriate symptoms and radiographic evidence of dysplasia were indicated for surgical treatment with a PAO using the technique described by Ganz et al. 13 Patients with corresponding morphologic variations of the proximal femur were treated with concomitant osteochondroplasty or femoral osteotomy. Labral tears identified at arthroscopy were repaired.
Postoperatively, patients were restricted to toe-touch weightbearing for 6 weeks and provided with a continuous passive motion machine. Patients treated with concomitant arthroscopy received heterotopic ossification prophylaxis with indomethacin 75 mg daily for 4 days before transitioning to naproxen 500 mg twice daily until 6 weeks after surgery. At 6 weeks postsurgically, patients progressed to weightbearing as tolerated if there was radiographic evidence of healing at the osteotomy site, and formal physical therapy was initiated. At 12 weeks postsurgically, strengthening exercises of the core, hip abductors, hip flexors, and quadriceps were introduced with the addition of resistance to training on the stationary bicycle. Functional exercises to include running, plyometrics, proprioceptive training, and dynamic strengthening were initiated at 16 weeks from surgery if the patient was able to demonstrate normal walking gait and symmetric stability when jumping on both legs. Sport-specific exercises were introduced at 20 weeks postsurgically, and therapy was continued until the patient was able to return to full functional activity without pain.
Patients’ medical, radiographic, and military records were reviewed. General demographic data were collected regarding the patients’ age, sex, body mass index, and prior surgical procedures on the ipsilateral hip. Military demographic data included the branch of service, rank, and military occupation. Military rank was aggregated into 2 categories consisting of junior enlisted personnel (below level E-5) and senior enlisted personnel or officers. Military occupations were classified as either combat arms or combat support to better estimate the functional demands of the position. 5 Combat arms occupations represent the fighting elements of each branch of service. Examples include Infantry, Armor, Artillery, Air Defense, and Aviation. Combat-support occupations supply and sustain the fighting strength. Examples include logistics, cybersecurity, and health care. Information regarding concomitant surgical procedures was collected. Radiographic data included the preoperative and postoperative lateral center-edge angle (LCEA), anterior center-edge angle (ACEA), and acetabular index (AI) (Figures 1 and 2). Preoperative and postoperative duty restrictions were noted, and the status of referrals to the US Army and Air Force MEBs was queried.

Preoperative (A) standing anteroposterior pelvis, (B) right false-profile, and (C) left false-profile radiographs obtained in a 21-year-old man treated with staged right and left periacetabular osteotomy for bilateral hip dysplasia.

Standing anteroposterior pelvis radiographs at (A) 6.8 months after right periacetabular osteotomy (PAO) and (B) 9.6 months after left PAO. (B) This patient had undergone right PAO 18.1 months before the image was taken.
Results
A total of 38 patients underwent PAO during the period studied. Seventeen patients were spouses or children of servicemembers and excluded from review. One servicemember underwent a PAO to treat iatrogenic dysplasia and gross instability of the hip after hip arthroscopy at an outside medical center. This patient was excluded from the analysis due to an ongoing MEB at the time of initial evaluation. Thus, the study sample consisted of 20 patients (15 female, 5 male) who were on active-duty service in the US military at the time of surgery and had a minimum of 28 months postoperative follow-up (Table 1). Patients were from either the US Army (n = 12) or US Air Force (n = 8). The mean age at surgery was 25.9 ± 6.0 years (range, 20-40 years), with 2 patients having undergone an arthroscopic hip procedure before PAO. Sixteen patients were on some form of duty restriction related to their hip within 6 months of surgery (TDR = 14; PDR = 2), 1 patient was a collegiate athlete without fitness restrictions, and preoperative duty restriction records were not available on 3 patients.
Demographic Information of the Study Patients (N = 20) a
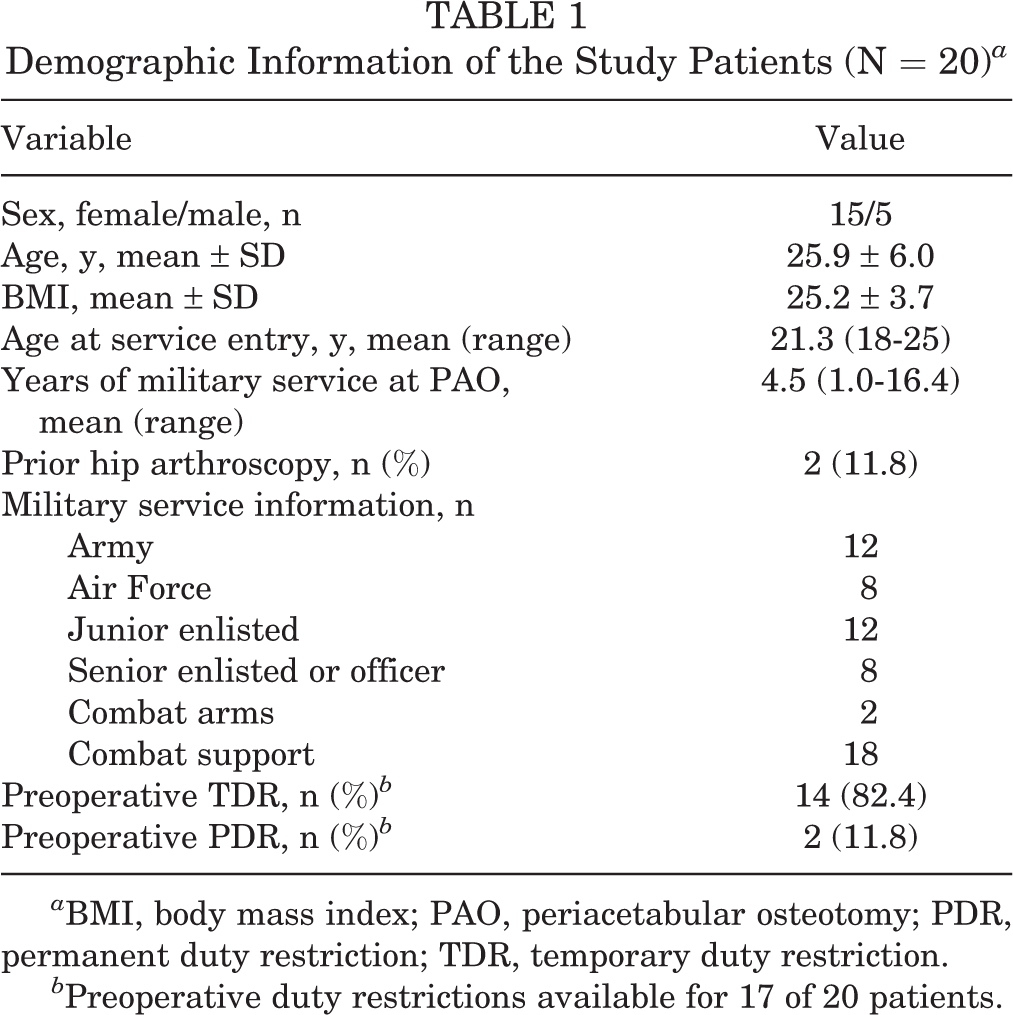
a BMI, body mass index; PAO, periacetabular osteotomy; PDR, permanent duty restriction; TDR, temporary duty restriction.
b Preoperative duty restrictions available for 17 of 20 patients.
Surgical Evaluation
Twelve patients (60%) underwent concomitant procedures at the time of PAO. The most common adjunct procedure was femoral head/neck osteochondroplasty (n = 10), which was performed arthroscopically (n = 8), via surgical hip dislocation (n = 1), and via open arthrotomy without dislocation at the time of PAO (n = 1). Additional notable concomitant procedures included 2 intertrocanteric femoral osteotomies (1 for post--slipped capital femoral epiphysis deformity and 1 for increased anteversion) and 1 curettage of acetabular aneurismal bone cyst. Five patients (25%) returned to the operating room for procedures on the ipsilateral hip over the course of the study, excluding isolated hardware removals (n = 3). Three patients underwent arthroscopic osteochondroplasty for symptomatic femoroacetabular impingement. One patient underwent revision open reduction and internal fixation for loss of fixation in a concomitant intertrochanteric osteotomy. One patient underwent heterotopic ossification excision with combined hardware removal. Three patients also underwent a PAO on the contralateral hip while on active-duty status (range, 9-28 months from index procedure) (Figure 2). Table 2 provides the mean pre- and postoperative LCEA, ACEA, and AI for all study patients.
Pre- and Postoperative Radiographic Parameters a
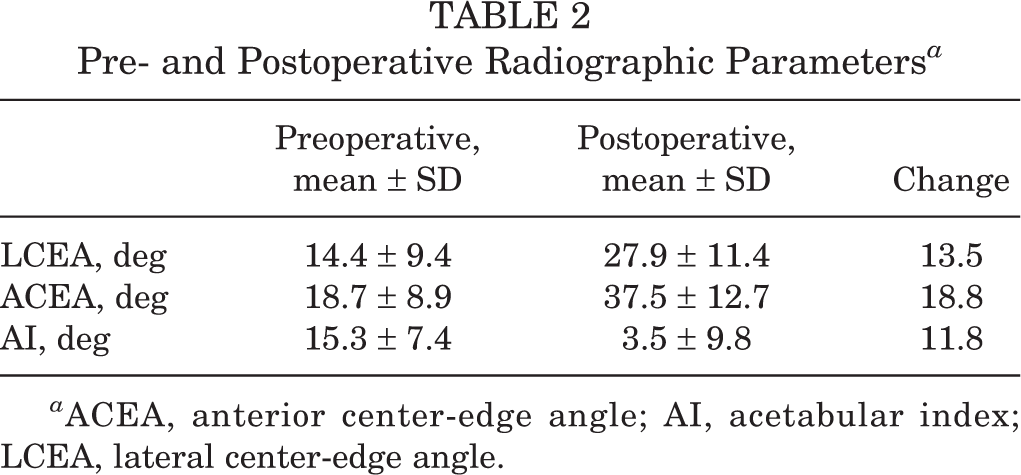
a ACEA, anterior center-edge angle; AI, acetabular index; LCEA, lateral center-edge angle.
Follow-up Evaluation
At 1 year postoperatively, 6 patients had returned to unrestricted duty, 6 remained on TDR, 3 advanced from temporary to permanent restricted duty, 2 remained on PDR, and records were unavailable on the remaining 3 patients. The average total follow-up at the time of review was 3.3 years (range, 2.3-5.4 years) (Table 3). At the final review, 7 patients of the total 20 (35%) had returned to unrestricted duty, including 2 who later separated from the military. The average time for return to unrestricted duty among these patients was 9.3 ± 5.5 months (range, 5.0-20.3 months).
Of the patients who returned to full duty, 3 were classified as junior enlisted at the time of surgery (3 of 12; 25%) and 4 were classified as senior enlisted or officers (4 of 8; 50%) (Table 3). At the final review, 12 patients (60%) remained on active duty, 5 patients (25%) had completed their service commitments and separated from the military, 2 (10%) were medically discharged for unrelated conditions, and 1 (5%) was medically discharged due to complications with a posterior column stress fracture after the PAO. Of the 5 patients referred to MEB, 2 were deemed fit to remain on active duty with only a modification of the aerobic component in the physical fitness assessment. The patient who was medically retired was granted a 20% VA disability rating for hip pathology.
When assessing military status at the final review by rank at time of surgery, 6 junior enlisted personnel remained on active duty, 3 had medically separated from service, and 3 had undergone nonmedical separation. Among the senior enlisted or officer cohort, 6 remained on active duty and 2 had undergone nonmedical separation (Table 3). When assessing military status at the final review among combat arms servicemembers, both remained on active duty (2 of 2; 100%). One returned to full duty, and 1 remained in her occupation, underwent a contralateral PAO, and was retained on active duty with a modification of the aerobic component in the physical fitness assessment.
Military Status at Final Follow-up a

a Data are presented as No. of patients or mean ± SD unless otherwise indicated. AD, active duty; PDR, permanent duty restriction; TDR, temporary duty restriction; VA, Veterans Affairs.
Discussion
This is one of the first studies to look at the impact of PAO on the activity levels and careers of active patients with symptomatic acetabular dysplasia. It is the first to evaluate the outcomes of this procedure in active-duty military personnel. The impact of this pathology on the activity and occupational effectiveness of these personnel is reflected in the finding that of 17 patients with available preoperative military records, 94% were on duty restrictions before PAO (temporary, n = 14; permanent, n = 2). Such duty restrictions have a significant impact on troop readiness and can compromise the viability of a military career. Of those with preoperative temporary restrictions, 35.7% (n = 5, of 14 that had temporary duty restrictions preoperatively) returned to full duty at an average of 9.3 months (range, 5.0-20.3 months; SD, 5.5 months) after surgery. However, in the reviewed period, 85% of patients were able to remain on active duty (n = 12) or complete their military service commitments (n = 5) without noted medical disability.
Since its introduction, the use of the PAO has expanded in an effort to preserve the articular integrity of the hip in patients with acetabular dysplasia and symptomatic hip instability. 13 In recent years, the focus of many centers has shifted toward patient-reported outcomes and the impact of the procedure on their level of activity. In a review of 51 patients who underwent PAO over a 2.5-year period at a single institution, Novais et al 17 found significant improvements in the University of California, Los Angeles (UCLA) activity score at 1 year and a minimum of 2 years postoperatively. Furthermore, they found that age <28 years and preoperative activity level were strong independent predictors of activity level after PAO. 17 Similar findings were reported by Bogunovic et al, 6 who reviewed postoperative activity levels in a cohort of active patients with acetabular dysplasia who underwent PAO at a single center with preoperative UCLA activity scores ≥7. They found no significant change in patient activity level after PAO, with 71% of patients returning to their presurgical or higher activity levels and 97% of patients satisfied with the procedure. 6 With an average 6.8-year follow-up, Okoroafor et al 19 found that 67% of the 58 patients in their case series maintained a UCLA score ≥7 and only 4 patients (7%) cited hip pain as limiting their activity after PAO.
Return to activities has also been assessed in a subgroup analysis of athletes undergoing PAO. In a cohort of 41 patients (46 PAOs) who met the criteria for being an athlete, Heyworth et al 14 found that UCLA activity scores were maintained at a high level (>8/10) and return to play was achieved in 80% of patients at a median of 9 months after PAO. Among a cohort of female dancers, return to dance was noted in 63% at an average of 8.8 months (SD ±3.6 months) after PAO. 18 These metrics are also an area of focus for the Academic Network of Conservational Hip Outcomes Research study. 7 In its first report of prospectively collected patient outcomes, significant improvement was noted in UCLA activity score, modified Harris Hip Score, Hip disability and Osteoarthritis Outcome Score, and 12-Item Short Form Health Survey score among 320 patients who underwent PAO for symptomatic acetabular dysplasia at multiple centers over a 3-year period. 7
This study has several limitations beyond its single-center design, small sample size, and retrospective nature. First, this cohort represents the initial patients treated after the establishment of this referral-based program and thus could represent the early learning period of the surgeon and the system. This likely contributed to the relatively high rate of patients returning to the operating room, which was also magnified by the small sample size. In addition, this early cohort lacks pre- or postoperative patient-reported metrics or objective measurements of patient activity, which have since been incorporated into the practice. This makes it difficult to compare these results with previous studies on civilian populations. Second, the inclusion of only active-duty US military personnel limits its generalizability, as the draws and demands of voluntary military service attract a unique subset of the population. Beyond the call of patriotic duty, the US military also provides opportunities for leadership, academic scholarship, health care benefits, and retirement pensions. It must also be recognized that the activity demands vary between military occupations, and certain career fields may permit more physical accommodations (ie, PDR) than others. While TDR or PDR allows servicemembers to postpone or modify fitness assessments, some branches only permit 12 months of restriction before automatic referral to a MEB. Considering that nearly all of this cohort was already on some form of duty restriction in the 6 months preceding surgery and the average time for return to duty was 9.3 months, such an automatic MEB referral situation could jeopardize the career aspirations of patients with symptomatic dysplasia. This system may dissuade them from considering surgery while on active duty or require them to return to full activity prematurely.
Finally, return to duty is an imperfect surrogate for activity level as measured by the UCLA activity score or return to play in athletes. Some have even compared it with workers’ compensation data in civilians. 4,20,24 Nonetheless, troop readiness is an important metric for military commanders, and return to duty is a manifestation of this important task. As with high-level professional athletes, personnel in combat arms roles or special operations units have historically demonstrated higher rates of return to duty after orthopaedic surgical procedures. 1,2,10 When considering athletes in general, common psychological responses associated with a higher likelihood of returning to preinjury level of participation include motivation, confidence, and low fear level. 3 Such characteristics are also likely innate or carefully trained among battlefield soldiers and special operators. Among personnel in combat support roles, return-to-duty rates have been less encouraging. In a review of 470 active-duty personnel who underwent primary anterior cruciate ligament reconstruction, 52.6% required either MEB referral, PDR, or both after surgery. 2 Similar findings were also seen in personnel who underwent meniscal allograft transplantation. 1 US military personnel have already demonstrated suboptimal results after arthroscopic hip procedures with unrestricted return-to-duty rates of only 39% to 59% in select populations. 11,21,25
Conclusion
Acetabular dysplasia significantly affects physical readiness in affected servicemembers, with 94% requiring duty restrictions before PAO. Evaluating surgeons should counsel patients on the short- and long-term implications of their dysplasia for both their military career and the articular integrity of their hip. PAO allowed 85% of patients to return to military service, with 1 in 3 able to return to duty without residual restrictions. Despite the unique features inherent to US military service and return-to-duty metrics, servicemembers are not exempt from the physical limitations and degradative sequelae of acetabular dysplasia. In these young, active patients with symptomatic acetabular dysplasia, PAO may provide a surgical option for return to high-level activities within the military. Further prospective data collection with the inclusion of patient-reported outcomes and activity levels will be required to better assess the impact of the procedure in this patient population.
Footnotes
Acknowledgment
The authors thank James Aden, PhD, for his assistance with the statistical analysis and Kara Carrier for her assistance with the image formatting.
Final revision submitted September 16, 2021; accepted October 12, 2021.
The views expressed herein are those of the authors and do not reflect the official policy or position of San Antonio Military Medical Center, the US Army Medical Department, the US Army Office of the Surgeon General, the Department of the Army, the Department of the Air Force, the Department of Defense, or the US Government.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.S.M. has received education payments from Alon Medical Technology and Medinc of Texas and hospitality payments from Stryker. M.R.S. has received education payments from Arthrex and Stryker, publishing royalties from Elsevier, and hospitality payments from Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from San Antonio Military Medical Center.