
Abstract
Background:
Nonoperative and operative treatment modalities have been used for symptom management of adhesive capsulitis, but neither has been shown to significantly alter the long-term natural history.
Purpose/Hypothesis:
The purpose was to evaluate the current trends in resource and treatment strategy utilization for patients with adhesive capsulitis. It was hypothesized that (1) patients with idiopathic adhesive capsulitis will primarily undergo nonoperative treatment and (2) patients with systemic medical comorbidities will demonstrate relatively higher utilization of nonoperative therapies.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
We searched the Mariner/PearlDiver database for Current Procedural Terminology and International Classification of Diseases codes to identify patients with adhesive capsulitis from 2010 to 2020 and to track their usage of diagnostic and therapeutic modalities, including radiography, magnetic resonance imaging (MRI), physical therapy, surgery, opioids, and injection. Patients with active records 1 year before and 2 years after initial diagnosis of adhesive capsulitis were eligible. Excluded were patients with secondary causes of adhesive capsulitis, such as fracture, infection, prior surgery, or other intra-articular pathology.
Results:
The median age of this 165,937-patient cohort was 58 years, with 67% being women. There was a high prevalence of comorbid diabetes (44.2%), thyroid disorder (29.6%), and Dupuytren contracture (1.3%). Within 2 years of diagnosis of adhesive capsulitis, diagnostic and therapeutic modality utilization included radiography (47.2%), opioids (46.7%), physical therapy (43.1%), injection (39.0%), MRI (15.8%), arthroscopic surgery (2.7%), and manipulation under anesthesia (2.5%). Over 68% of the diagnostic and therapeutic modalities were rendered from 3 months before to 3 months after diagnosis. Patients with diabetes, thyroid disorders, tobacco use, and obesity had greater odds for treatment with physical therapy, opioids, radiography, and injection when compared with patients without these comorbidities (odds ratio [OR] range, 1.05-2.21; P < .0001). Patients with diabetes and thyroid disorders had decreased odds for surgery (OR range, 0.88-0.91; P ≤ .003). Patients with Dupuytren contracture had increased odds for all therapeutic modalities (OR range, 1.20-1.68; P < .0001).
Conclusion:
Patients with adhesive capsulitis underwent primarily nonoperative treatment, with a high percentage utilizing opioids. The most active periods for treatment were from 3 months before diagnosis to 3 months after, and patients with medical comorbidities were more likely to undergo nonoperative treatment.
Adhesive capsulitis was first introduced as a concept of shoulder pathology in 1872 by Simon-Emmanuel Duplay, 9 which he termed “periarthritis scapulohumerale.” Almost 60 years later, Ernest Amory Codman 4 described this phenomenon as “frozen shoulder,” and he contributed more to our understanding by describing criteria for diagnosis, of which the hallmark feature was limited active and passive range of motion of the shoulder. 13 At the time, Codman described this entity as “difficult to define, difficult to treat and difficult to explain.”4 In 1945, Julius S. Neviaser 15 used the term “adhesive capsulitis” to define this disease. Despite significant advances in diagnostic imaging and treatment modalities since Codman’s description in 1934, 4 adhesive capsulitis remains difficult to define, treat, and indeed explain.
Primary adhesive capsulitis is defined as an idiopathic condition with functional restriction of passive and active shoulder motion, for which radiographs are unremarkable and there is no known underlying cause or associated condition. Secondary types of adhesive capsulitis include all cases where an underlying cause can be identified—ranging from intra- to extra-articular and some systemic conditions, such as diabetes and thyroid disorder. 31 The cause of adhesive capsulitis is not currently known, although researchers have hypothesized a role for inflammatory cytokines, genetic predisposition to fibrosis, and the hormonal influence of estrogen and thyroid-stimulating hormone. 1,5,19,29 Adhesive capsulitis is estimated to have an incidence of roughly 2% to 5%, with a predominance toward middle-aged women and the nondominant arm. 11,27 Additional risk factors associated with adhesive capsulitis include diabetes mellitus, thyroid disease, and genetic disposition, such as Dupuytren-like disease. 1,11,21,26
Treatment regimens for adhesive capsulitis vary significantly according to stage of presentation, age, prior treatments, and patient preference. Although there is no standard treatment plan, it is widely recommended to try conservative therapy before surgical intervention. 12 In a recent meta-analysis, Yip et al 27 compared treatment strategies such as physical therapy, nonsteroidal anti-inflammatory medications, intra-articular injection, hydrodilatation therapy, surgery, and manipulation under anesthesia (MUA), and they were unable to make a conclusive statement about the most appropriate first-line therapy based on the current available evidence. 10
The goal of this study was to evaluate the current trends in resource and treatment strategy utilization for patients diagnosed with adhesive capsulitis. We hypothesized that (1) patients with idiopathic adhesive capsulitis will primarily undergo nonoperative treatment and (2) patients with systemic medical comorbidities will demonstrate relatively higher utilization of nonoperative therapies.
Methods
Deidentified data from the Mariner database, which is composed of 122 million patients from multiple insurance payer types (commercial, Medicare, Medicaid, cash, and government), were queried using the PearlDiver program (PearlDiver Inc). A retrospective cohort analysis of all patients from 2010 to 2020 was performed. A CONSORT (Consolidated Standards of Reporting Trials) diagram in Figure 1 presents the complete cohort inclusion and exclusion criteria.
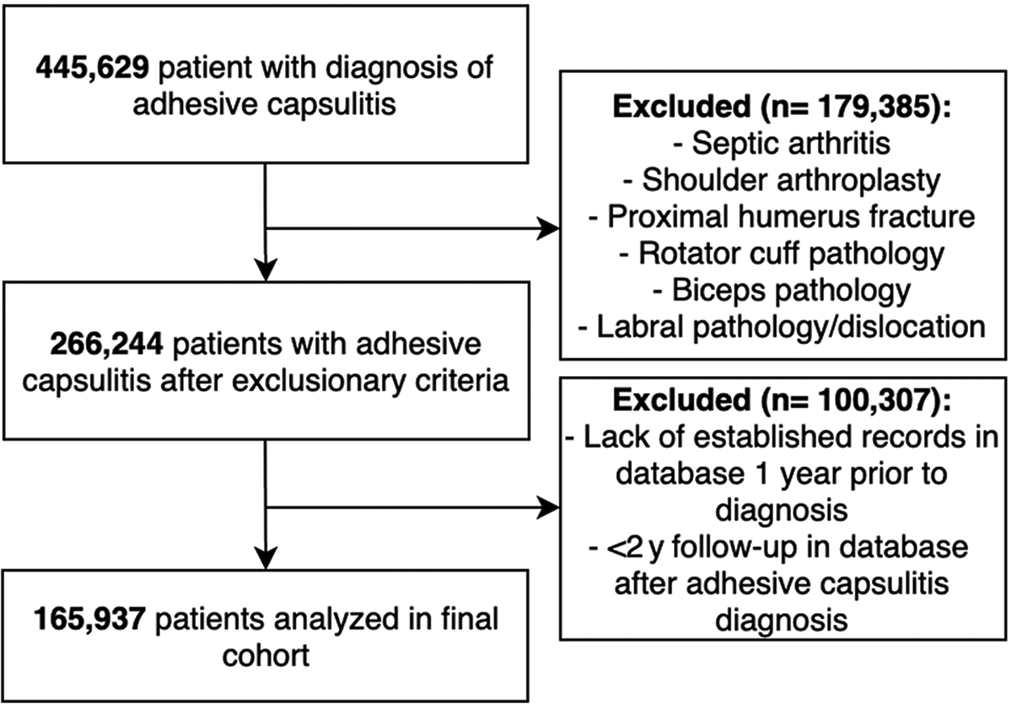
CONSORT diagram for cohort analysis.
Identification of Patients With Adhesive Capsulitis and Associated Diagnoses
A diagnosis of adhesive capsulitis was identified using codes from the International Classification of Diseases, Ninth and Tenth Revision (ICD-9, ICD-10): ICD-9-D-7260, ICD-10-D-M7501, and ICD-10-D-M7502. Associated diagnoses of prior shoulder arthroplasty, septic arthritis, proximal humerus fracture, rotator cuff pathology (including impingement and cuff tear), biceps pathology, SLAP (superior labrum anterior and posterior) tear, and prior shoulder dislocation were identified with codes from ICD-9, ICD-10, and Current Procedural Terminology (CPT) (Supplemental Table A1). Patients with these diagnoses were excluded from the adhesive capsulitis cohort. To minimize selection bias, only patients with active records in the database 1 year before their initial adhesive capsulitis diagnosis and for at least 2 years after were included in the study. Baseline demographics were identified with additional stratification of ICD-9 and ICD-10 codes for diagnoses of tobacco use, obesity, diabetes, Dupuytren contracture, and thyroid disorders (Supplemental Table A2). Additionally, data were collected on all patients for the Charlson Comorbidity Index, which is a widely used validated scoring instrument that allows for general assessment of patient health. 2 Patients with records 1 year before and 2 years after initial diagnosis of adhesive capsulitis were eligible for analysis, but utilization data were analyzed in the 6 months before and 2 years after initial diagnosis.
Identification of Patient Resource Utilization
Tracking of patient diagnostic and therapeutic modality utilization was performed using CPT codes for physical and occupational therapy, shoulder radiographs, upper extremity magnetic resonance imaging (MRI), large joint injection, arthroscopic procedure, and MUA (Supplemental Table A3). Opioid use was tracked using the Mariner drug prescription database for generic and brand name opioid medications containing hydrocodone, oxycodone, oral morphine, and oral hydromorphone. In the Mariner database, a drug prescription claim is created when the prescription is filled, so each instance of utilization represents a filled opioid prescription. Opioid utilization was evaluated from 6 months before and 24 months after adhesive capsulitis diagnosis, and it was binned into categories of 3 to 6 months prior, 0 to 3 months prior, 0 to 3 months after, 3 to 6 months after, 6 to 12 months after, and 12 to 24 months after diagnosis. All patients had a minimum of 2-year tracking in the PearlDiver database after their initial adhesive capsulitis diagnosis.
Statistical Analysis
Data analyses were conducted using Prism Statistics/Data Analysis software (GraphPad Software Inc) and R statistical software (R Project for Statistical Computing version 4.1.0) integrated with PearlDiver. P < .05 was considered statistically significant. A Shapiro-Wilk normality test was run to assess normality of the cohort. Pearson chi-square test with Yates continuity correction was used to test the significance of associations. R statistical software was used to calculate the odds ratio (OR) and 95% CI to determine the likelihood of a comorbidity group using an intervention.
Results
A total of 165,937 patients with adhesive capsulitis were identified, consisting of 111,432 women (67%) and a median age of 58 years (interquartile range, 50-67 years) (Table 1). The Shapiro-Wilk normality test's P value was <.001, indicating nonnormal age distribution with leftward skew (Figure 2). Age range data indicated that 77% of the patients were aged ≥50 years upon insurance claim diagnosis of adhesive capsulitis. Table 1 presents additional demographic information regarding this cohort, including the prevalence of diabetes (44.2%), obesity (31.8%), tobacco use (20.2%), thyroid disorder (29.6%), and Dupuytren contracture (1.28%), as well as the mean Charlson Comorbidity Index score.
Demographic Data a

a Data are reported as No. (%) of patients, unless noted otherwise. Percentages are based on the overall population (N = 165,937). CCI, Charlson Comorbidity Index; IQR, interquartile range.

Percentage of patients with adhesive capsulitis by age range (N = 165,937).
Utilization Trends
During this study’s active monitoring period for modality utilization (6 months before first instance of diagnosis to 2 years after), the percentage of patients by modality was as follows: radiographs, 47.2%; opioids, 46.7%; physical therapy, 43.1%; injection, 39.0%; MRI, 15.8%; arthroscopic surgery, 2.7%; and MUA, 2.5%. Figure 3 shows the breakdown of this utilization percentage by period, with the highest percentages of all modalities from 3 months before diagnosis until the first instance of diagnosis. The majority of diagnostic and therapeutic modalities were rendered during the 3 months before diagnosis to the 3 months after diagnosis: 76%, physical therapy; 68%, opioids; 83%, radiographs; 78%, MRI; 80%, injection; 74%, surgery; and 100%, MUA. Table 2 shows exact utilization by percentage at each time point stratified by sex. It also demonstrates a significantly higher percentage of utilization for women in every modality at every period (P < .01).

(A) Diagnostic and (B) therapeutic modality utilization by month from initial diagnosis. The percentage is the proportion of the total population with adhesive capsulitis (N = 165,937). MRI, magnetic resonance imaging (upper extremity); MUA, manipulation under anesthesia; PT, physical or occupational therapy; XR, shoulder radiograph. Opioids include hydrocodone and oxycodone.
Modality Utilization by Sex a

a Data are reported as No. (%) of patients based on the overall population (N = 165,937). MRI, magnetic resonance imaging (upper extremity); MUA, manipulation under anesthesia; PT, physical or occupational therapy; XR, radiographs (shoulder or humerus).
b Opioids include hydrocodone- and oxycodone-based medications.
Associated Diagnosis Trends
Table 3 demonstrates the association of different comorbidities and their effect on diagnostic and therapeutic modality utilization. The ORs represent a comparison between patients with and without the comorbidity of interest.
Effect of Comorbidities on Modality Utilization vs Patients Without the Comorbidity of Interest a

a MRI, magnetic resonance imaging (upper extremity); MUA, manipulation under anesthesia; PT/OT, physical or occupational therapy; XR, radiographs (shoulder or humerus).
b Opioids include hydrocodone- and oxycodone-based medications.
Diabetes
atients with an associated diagnosis of diabetes had higher odds of the following utilization (by percentage increase in likelihood): 10%, physical/occupational therapy; 15%, radiography; 17%, opioids; and 14%, injection.
Thyroid Disorders
Patients with an associated diagnosis of thyroid disorders had higher odds of the following utilization (by percentage increase in likelihood): 18%, physical/occupational therapy; 5%, radiography; 5%, opioids; and 19%, injection. They had 12% decreased odds of surgery.
Obesity
Patients with obesity had higher odds of the following utilization (by percentage increase in likelihood): 22%, physical/occupational therapy; 23%, radiography; 62%, opioids; 32%, injection; and 6%, MRI. There was no significant association with utilization of surgery or MUA.
Tobacco Use
Patients with a history of tobacco use had higher odds of the following utilization (by percentage increase in likelihood): 8%, physical/occupational therapy; 33%, radiograph; 121%, opioid; 9%, injection; 21%, MRI; 18%, surgery; and 15%, MUA.
Dupuytren Contracture
Patients with an associated diagnosis of Dupuytren contracture had higher odds of the following utilization (by percentage increase in likelihood): 50%, physical/occupational therapy; 20%, radiography; 43%, opioids; 47%, injection; 35%, MRI; 68%, surgery; and 57%, MUA.
Discussion
In this study, utilization trends demonstrated a predominance of nonoperative treatment of adhesive capsulitis, with a high percentage of opioid use and with the majority of diagnostic and therapeutic intervention occurring from 3 months before to 3 months after the first instance of diagnosis. Additionally, the demographic data show the greatest incidence of adhesive capsulitis in middle-aged to elderly women, as illustrated with the leftward skew in Figure 2. Our results are also consistent with literature suggesting a high comorbid incidence of diabetes and thyroid disorder.
The median age of our cohort was 58 years, and 67% of the patients were women. This aligns with previous studies 11,27 suggesting that adhesive capsulitis predominantly affects women aged 40 to 60 years. The prevalence of comorbid diabetes in our population was 44.2%, which is consistent with the literature's reports of 30% to 42%. 23,25,30 Likewise, the prevalence of comorbid thyropathy in our population was almost 30%, which is in agreement with a 2020 study by Cohen et al 5 where the prevalence was 34% in patients with adhesive capsulitis. We also evaluated the prevalence of comorbid Dupuytren contracture (1.3%), which was found to be similar to reports of 0.5% to 1% for the general population when defined by diagnosis or treatment. 6
Our study demonstrated that the most commonly used diagnostic and therapeutic modalities for adhesive capsulitis were radiography, opioids, therapy, and injection, which are all conservative measures that are noninvasive. Less commonly used modalities were MRI, surgery, and MUA, which are all advanced imaging techniques or invasive procedures. This treatment approach is consistent with a 2019 meta-analysis by Yip et al, 27 who described a consensus that nonoperative techniques should be used initially for the treatment of adhesive capsulitis. In that analysis, the authors were unable to conclude whether any treatment modality was superior, nor could they find that any treatments altered the long-term natural history of adhesive capsulitis. Physical therapy is one of the most frequently used nonoperative therapies for adhesive capsulitis, and the scope of treatment varies across modality, frequency, and setting of the therapy. Studies 3,7,20 have shown improvement in pain scores, range of motion, and quality-of-life scores for in-person therapy and home exercise programs, and they have supported a variety of special techniques, such as continuous passive motion and sustained stretching; however, there remains insufficient evidence to conclude that any form or setting of therapy is superior. Likewise, although they have found intra-articular corticosteroid injections to be effective in limiting short-term pain, they have not been able to demonstrate any long-term differences in outcome. 14,16,24,28
Our study revealed that most diagnostic and therapeutic modality utilization occurred within the 3 months before and 3 months after the first instance of diagnosis claim. This utilization rate is consistent with the self-limiting nature of adhesive capsulitis, and it is reflective of the current state of treatment being primarily early symptom management without the ability to alter long-term natural history. 27 In our cohort, surgery and MUA were seldomly utilized therapies (2.7% and 2.5% of patients, respectively). Interestingly, the most surgery and MUA occurred in the 3 months preceding and 3 months after diagnosis. This contradicts the conventional treatment strategy of first trying physical therapy, nonsteroidal anti-inflammatory drugs, and corticosteroid injection before considering arthroscopic debridement or MUA. The meta-analysis by Yip et al 27 recommended against early operative intervention, as there was insufficient evidence to support superior long-term outcomes as compared with physical and/or injection therapy.
In our cohort, 47.2% of the patients had a claim for shoulder or humerus radiograph in the studied period. While this number is lower than expected, adhesive capsulitis is a clinical diagnosis that relies on physical examination findings of limited active and passive range of motion for diagnosis, so radiographs are not necessary for diagnosis. It is also possible that patients had this imaging workup outside our queried window of 6 months before to 2 years after diagnosis. Interestingly, 15.8% of the patients had MRI during this queried window. This percentage of utilization is higher than what we would anticipate for evaluation of adhesive capsulitis, especially with the exclusion of patients diagnosed with rotator cuff, biceps, labral, and capsule pathology.
Opioid use in nearly half of patients was higher than what we would anticipate, as opioids are not a recommended therapeutic for the treatment of adhesive capsulitis, and to our knowledge this is a novel finding. Little is written on the use of opioids in the treatment of adhesive capsulitis, but review articles 18,27 in orthopaedic and primary care literature do not suggest opioids, even for refractory cases. One study 22 of nearly 89,000 patients with new musculoskeletal pain concluded that physical therapy within 90 days of initial diagnosis decreased opioid use by 10%. Interestingly, opioid prescription utilization in our study doubled from 6 to 24 months after initial diagnosis, which may suggest that some of the patients' refractory to traditional therapies rely on opioid medications for long-term management. Given the US Centers of Disease Control and Prevention’s and the American College of Physicians’ advocation for nonpharmacologic frontline therapy for the management of chronic pain, including musculoskeletal pain, further research is warranted to elucidate the use of prescribing opioids for adhesive capsulitis. 8,17
Our analysis evaluated the effect of various comorbidities on utilization rates. In general, patients with more medical comorbidities tended to have higher odds of conservative treatments. We saw that patients with diabetes, tobacco use, thyroid disorders, and obesity had increased ORs for physical therapy, radiography, opioids, and injection therapy (P < .001). This agrees with conventional wisdom that medically complex patients are first treated nonoperatively due to higher risk of surgical complication, particularly when there is no clear superiority for surgical intervention, as in the case of adhesive capsulitis. Similarly, patients with diabetes or thyroid disorder had significantly decreased ORs of undergoing arthroscopic debridement. We also found that patients with a diagnosis of Dupuytren contracture were significantly more likely to use all modalities, and their ORs were the greatest in all categories except for radiography and opioids. This supports a popular notion that the pathogenesis of adhesive capsulitis may be related to that of Dupuytren contracture, suggesting a genetic predisposition to the disease, although further research is needed to confirm this hypothesis.
Limitations
The findings of our study should be interpreted within the context of its limitations. The validity of our results is reliant on accurate ICD-9, ICD-10, and CPT codes submitted with insurance claims. We did apply specific inclusion and exclusion criteria to minimize any potential for misclassification or confusion. For assessment of shoulder injection, the CPT code is the same for shoulder aspiration, so it is not possible to delineate aspiration from injection with administrative coding. With the exclusion of diagnoses that would involve aspiration, such as septic arthritis, we hope to have minimized the number of patients who underwent aspiration; however, this would artificially increase our injection utilization percentage. The Mariner database does not provide granular data on patient function, pain, or response to treatment, which did not allow us to evaluate efficacy of treatment. Furthermore, tracking of opioid prescriptions could not be linked to the diagnosis of adhesive capsulitis, so one cannot isolate shoulder pain as the reason for opioid medication. Results of this study are limited to isolated adhesive capsulitis and do not assess secondary adhesive capsulitis.
Conclusion
Patients with adhesive capsulitis underwent primarily nonoperative treatment as compared with operative intervention, with a high percentage utilizing opioids. The most active periods for treatment were from 3 months before diagnosis to 3 months after, and patients with medical comorbidities were more likely to undergo conservative treatment. Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671211003521.
Supplemental material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211069577 - Evaluating Utilization Trends in Adhesive Capsulitis of the Shoulder: A Retrospective Cohort Analysis of a Large Database
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211069577 for Evaluating Utilization Trends in Adhesive Capsulitis of the Shoulder: A Retrospective Cohort Analysis of a Large Database by Charles J. Cogan, Nicolas Cevallos, Ryan D. Freshman, Drew Lansdown, Brian T. Feeley and Alan L. Zhang in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted August 22, 2021; accepted October 7, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.L. has received education payments from Arthrex and Smith & Nephew and hospitality payments from Wright Medical. B.T.F. has received education payments from Evolution Surgical and hospitality payments from Zimmer Biomet. A.L.Z. has received consulting fees from DePuy and Stryker and hospitality payments from Arthrex and Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval
Ethical approval was not sought for the present study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.