
Abstract
Background:
In patients with chronic lateral epicondylitis who have failed nonoperative treatment, open or percutaneous release of the common extensor origin (CEO) without subsequent reconstruction tends to result in good clinical outcomes. However, surgery can lead to iatrogenic injuries of the lateral collateral ligamentous complex, causing posterolateral rotatory instability (PLRI).
Purpose:
To determine the clinical outcomes of lateral ulnar collateral ligament (LUCL) reconstruction using a triceps tendon graft after failed open CEO surgery.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 103, patients underwent revision surgery at a single institution because of PLRI after failed open release of the CEO (Hohmann procedure) between January 2007 and October 2016. The primary surgery had been performed at other institutions in all cases. Of these patients, 72 were available for follow-up (49 by clinical examination, 23 by telephone interview). Standardized clinical examination; Mayo Elbow Performance Score (MEPS); 11-item version of the Disabilities of the Arm, Shoulder and Hand Score (QuickDASH); subjective elbow value (SEV); and patient satisfaction were assessed at least 2 years after LUCL reconstruction.
Results:
The mean age of patients in the study was 46.9 years (range, 21-74 years), and the mean follow-up was 2.8 years after revision surgery. The mean MEPS was 78.9, and the mean QuickDASH score reached 20.4. The mean SEV was 78.6%, and 75% of the patients rated the surgery as good to excellent. Complications were detected in 14% of the patients, and 9 needed revision surgery, primarily owing to graft failure with recurrent instability (n = 5).
Conclusion:
LUCL reconstruction in patients with PLRI after release of the CEO can restore elbow stability and achieve high patient satisfaction. However, outcome scores and revision rates in this cohort were inferior to published outcomes of primary LUCL reconstruction for treatment of noniatrogenic or traumatic PLRI.
Keywords
Lateral epicondylitis (LE) is a common cause of lateral elbow pain. 44 Nonoperative treatment remains the therapy of choice and leads to full recovery in up to 95% of patients. 13,26,44 However, the incidence of chronic courses with ongoing pain and impairment after 6 to 12 months has been reported to be as high as 11%. 8,22 In cases of failed nonoperative treatment, multiple surgical techniques may be utilized without one being superior to another. 7,22,23 The common extensor origin (CEO) can be released in 3 types of ways: open, percutaneous, or arthroscopic. Open release of the CEO comes in different variations: with or without debridement, denervation, resection of osteophytes, or repair of the CEO. 23
Open surgery achieves good-to-excellent results when performed correctly. 5,15,16,22 Complications after open release of the CEO seem to be rare and do not differ significantly from those of other techniques, except for a higher surgical-site infection rate. 34 However, although rarely reported, an accidental injury of the lateral collateral ligamentous complex (LCLC) and its primary stabilizer, the lateral ulnar collateral ligament (LUCL), is a major complication. The LUCL runs from the lateral epicondyle, inserts distally on the supinator crest of the ulna, and has a close relationship to the CEO. 12,37,38 Insufficiency of the LCLC often leads to posterolateral rotatory instability (PLRI) of the elbow. 10,27,40 Particularly in patients who undergo surgical release of the CEO without subsequent reconstruction, the accidentally injured LCLC is weakened, and PLRI might cause persisting pain at the lateral aspect of the elbow. 17,39
In patients with pain and PLRI, surgical stabilization is advocated. 3,43 The association of LCLC insufficiency and chronic LE as well as treatment recommendations have been described before. 4,21,43 However, clinical results after LUCL reconstruction for chronic PLRI as a salvage procedure are lacking.
The purpose of this study was to evaluate the clinical outcomes of LUCL reconstruction using a triceps tendon graft after failed open surgery for LE.
Methods
This retrospective study was initiated after gaining approval from the local institutional review board. Eligible for inclusion were 1160 patients who had undergone LUCL reconstruction as revision surgery for PLRI after failed open surgery for LE. All patients had been treated by 2 fellowship-trained high-volume elbow surgeons (B.H. and K.J.B.) between January 2007 and October 2016. Patients without prior surgery, or prior surgery other than open CEO release were excluded, leaving 103 patients who were eligible for study inclusion.
For all patients, the primary surgery had been performed at different institutions. All patients had undergone the Hohmann procedure as the primary surgery, in which the CEO was released and debrided without performing a reconstruction. The Hohmann technique differs from the procedure described by Nirschl and Pettrone, 26 who performed a reconstruction of the CEO. Standardized clinical examinations, including elbow stability tests, medical history recordings, and magnetic resonance imaging (MRI) were performed in all patients before LUCL reconstruction. Stability testing consisted of the posterolateral rotatory drawer test, chair push-up test, and tabletop relocation test.
A total of 24 patients were lost to follow-up because address data were no longer up to date; an additional 7 patients were not willing to be part of the study. Thus, of the 103 patients, 72 (70%) were evaluated at a mean of 2.8 years after LUCL reconstruction. There were 49 patients available for a clinical examination, and 23 participated in a telephone interview but refused to participate in an in-person consultation, owing primarily to travel and financial reasons. Figure 1 shows the flowchart of patient enrollment in the study.
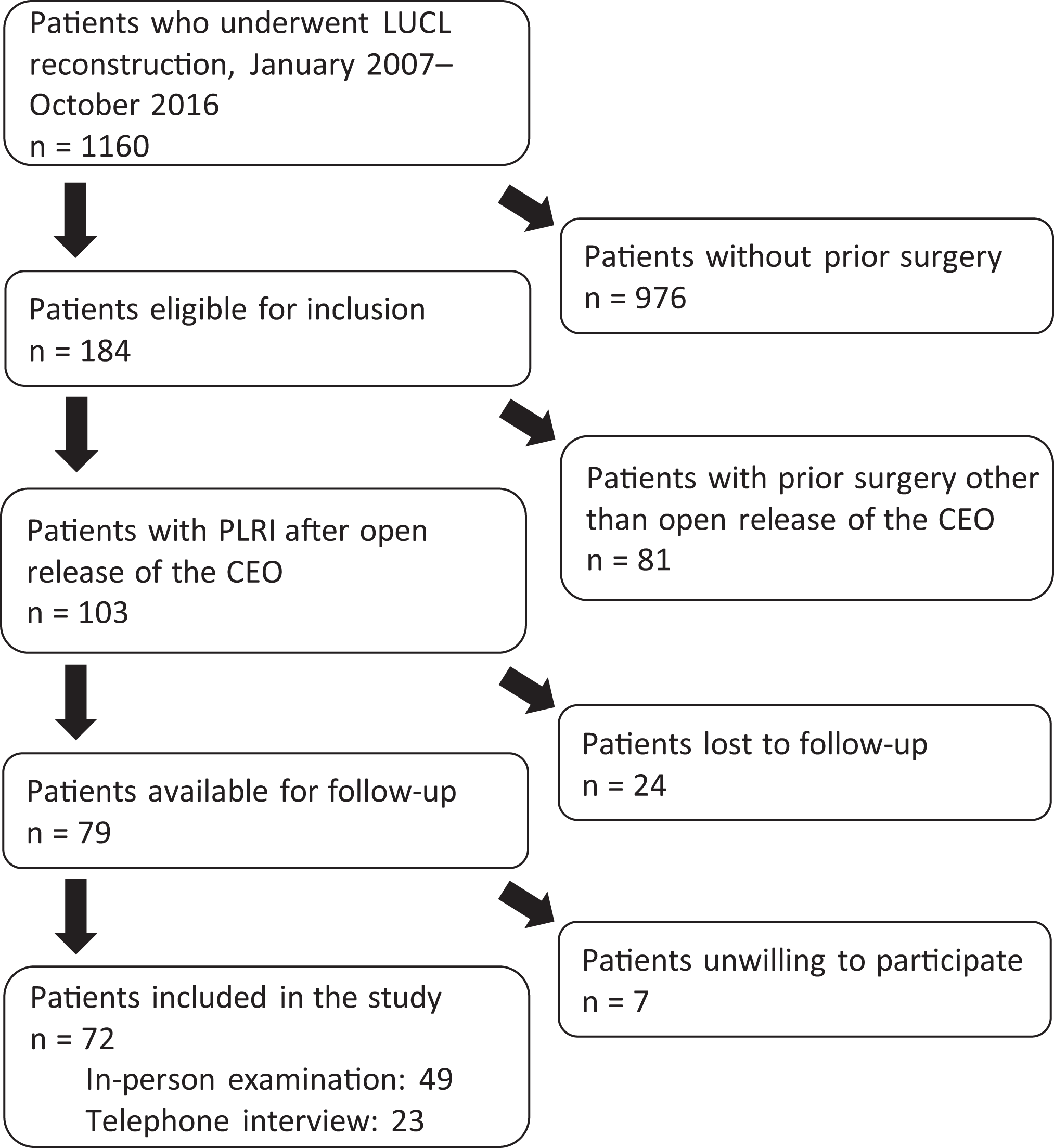
Flowchart of patient inclusion and exclusion. CEO, common extensor origin; LUCL, lateral ulnar collateral ligament; PLRI, posterolateral rotatory instability.
Data Collection
Table 1 summarizes the data collected during the preoperative, intraoperative, and postoperative assessments. The follow-up examination consisted of a clinical examination, including documentation of the range of motion, the 3 previously mentioned stability tests, and the following outcome measures: Mayo Elbow Performance Score (MEPS), 25 subjective elbow value (SEV) assessed by Single Assessment Numeric Evaluation, 36 11-item version of the Disabilities of the Arm, Shoulder and Hand (QuickDASH), 20 Patient-Related Tennis Elbow Evaluation (PRTEE), 33 and the Plazek score. 35 The MEPS was collected only in patients who returned for an in-person examination since the score is not validated for assessment by telephone. Furthermore, grip strength was measured using a hydraulic device (Hydraulic Hand Dynamometer; Rehaforum Medical). The highest value of 3 consecutive repetitions was defined as the maximal strength. In addition, patients were asked to grade their satisfaction with postoperative outcomes, to state whether they experienced an improvement of their symptoms after LUCL reconstruction, and to indicate whether they would undergo revision surgery again.
Overview of Collected Pre-, Intra- and Postoperative Data a
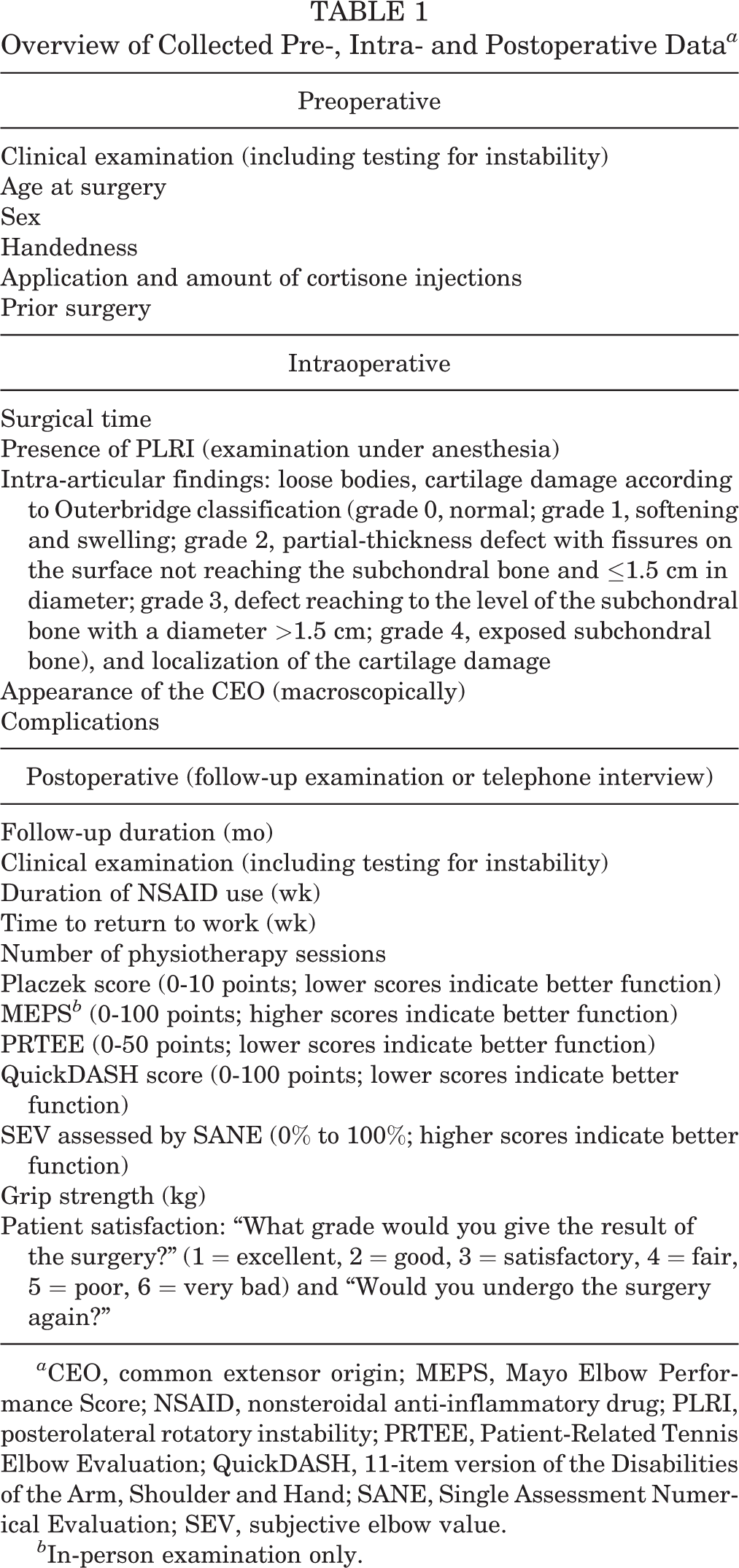
a CEO, common extensor origin; MEPS, Mayo Elbow Performance Score; NSAID, nonsteroidal anti-inflammatory drug; PLRI, posterolateral rotatory instability; PRTEE, Patient-Related Tennis Elbow Evaluation; QuickDASH, 11-item version of the Disabilities of the Arm, Shoulder and Hand; SANE, Single Assessment Numerical Evaluation; SEV, subjective elbow value.
b In-person examination only.
Surgical Procedure
All procedures were performed under general anesthesia with a continuous interscalene catheter. The patients were placed in the lateral decubitus position with a tourniquet on the affected arm (250 mm Hg). All patients underwent elbow arthroscopy with joint evaluation and assessment of PLRI, similar to the protocols described by Amarasooriya and Pladnis 2 and Geyer et al. 19 Cartilage lesions were assessed according to the Outerbridge classification. 31,32
Thereafter, an incision was made on the lateral aspect of the elbow at 90° of flexion, including the radial-sided portals, measuring approximately 12 cm. The fascia was incised at the lateral border of the triceps and distally between the extensor carpi ulnaris and the anconeus muscle. The attachment of the LCLC was exposed by detaching the CEO and the LCLC from the lateral epicondyle without lancing the anterior capsule. Then, a k-wire was placed in the humeral center of rotation, since this point is described as reproducing “the most isometry when assessing graft elongation over range of motion.” 1 Another k-wire was drilled into the supinator crest of the ulnar near the annular ligament at the height of the junction of the radial head to the neck. Isometry could be tested by placing a suture around the k-wires to mimic the LUCL.
After drilling, the triceps tendon graft was harvested at the ulnar third with the arm hanging in 90° flexion. We preferred a length of approximately 7 cm and a width of approximately 4.5 mm. The defect was closed with dissolving sutures. The tendon graft was prepared using a baseball stitch technique with a FiberLoop (Arthrex). The free ends of the sutures were threaded through a distal biceps button (Arthrex). Next, a 3.5-mm monocortical hole was drilled into the proximal ulna. The button was shuttled into the monocortical drill hole and flipped intramedullarily. The free ends of the FiberLoop were then tensioned to press the graft onto the proximal ulna. To secure the graft, both free ends were then stitched through the graft and knotted. Proximally, the graft was pulled into the drill hole and fixed with a 4.75-mm tenodesis screw (Arthrex) loaded with Vicryl sutures (Figure 2).
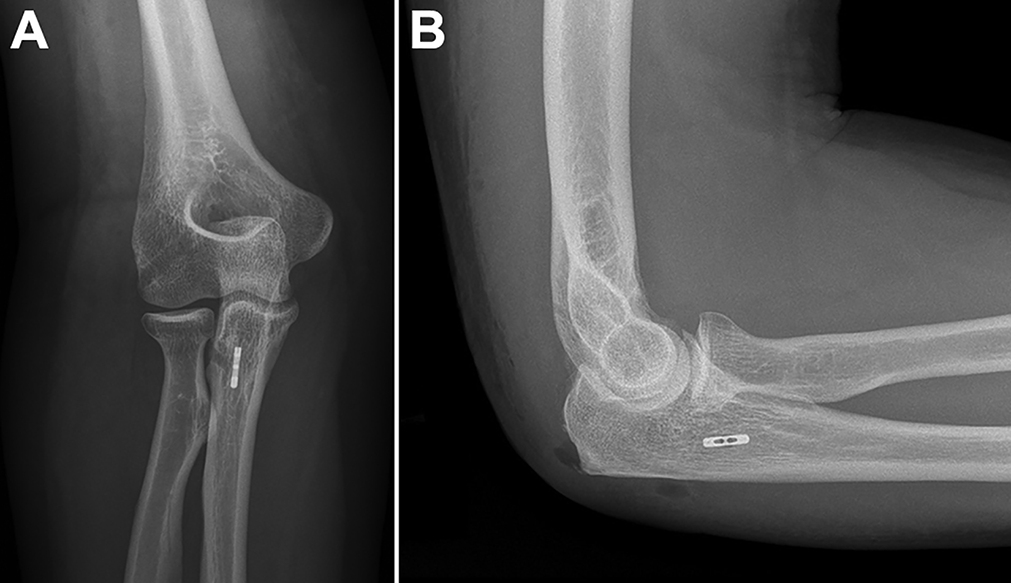
(A) Anteroposterior and (B) lateral radiographs of the elbow after lateral ulnar collateral ligament reconstruction with refixation by placing an EndoButton distally and a tenodesis screw proximally.
The positioning of the tenodesis screw allowed for corrections to the graft alignment over the humeral center of rotation of the LUCL origin. The CEO was repaired using a double-row technique, with either transosseous sutures (double-row equivalent) or double-row repair with a Pushlock anchor (Arthrex) placed at the anterolateral epicondyle to tension the free ends of the knotted sutures medially (suture bridge configuration). The fascia and skin were closed. The detailed surgical procedure was described by Dehlinger et al. 14
Postoperative Rehabilitation
In our setting, surgery was performed as an inpatient procedure for a duration of 2 days. Patients received an elbow brace for 6 weeks with flexion/extension limited to 90°-10°-0° for 4 weeks and without limitations in the final 2 weeks. Physiotherapy was provided immediately after surgery without range of motion restrictions. Heavy lifting and axial weightbearing were limited for 6 weeks. The sutures were removed 12 days after surgery. All patients received a continuous passive motion device to perform home exercises for 4 weeks. A clinical evaluation was requested after 6 weeks.
Validation and Statistics
Continuous variables are presented as means with ranges, and categorical variables are presented as frequencies and percentages. Data were analyzed using Xlstat statistics software (ADDINSOFT).
Results
Demographics
The mean age at revision surgery was 46.9 years (range, 21-74 years); 43% of the patients were aged between 46 and 55 years. Of the total patients, 39 (54%) were women and 33 (46%) were men. In total, 83.3% of the patients described a heavy workload for the elbow in their profession, and 77.7% of the operations were for the dominant arm. Surgery was performed on 52 right and 20 left elbows.
Prior Care (Including Infiltration Before Index Surgery)
A total of 77.7% of the patients received at other institutions a mean of 3.6 injections in the lateral elbow at the CEO (n = 54 injections with corticosteroids; n = 1 with Botox) before the Hohmann procedure. Generally, patients presented at our institution with ongoing pain. Our care for those patients included a course of nonoperative treatment for approximately 6 months after the Hohmann procedure to wait for time-delayed improvements. During this time, conservative measurements were carried out, including physiotherapy, electrotherapy, brace wearing, autonomous eccentric exercises following specific guidelines, shock wave therapy, and oral application of nonsteroidal anti-inflammatory drugs (NSAIDs). We recommended physiotherapy and autonomous eccentric exercises, following specific guidelines. Nonoperative orthopaedists initiated all other measurements (such as shock wave therapy, etc.). A specific protocol for conservative treatment did not exist.
Surgery and Intra-articular Findings
The mean surgical time was 54 minutes (range, 35-151 minutes) from incision to wound closure. Patients were evaluated arthroscopically before LUCL reconstruction. PLRI was confirmed in all 72 patients using stability testing, similar to protocols described previously. 2,19 Loose bodies were detected in 4 patients (5.5%). Small focal cartilage lesions were found in 23.6% (n = 17) but did not affect the main stress-bearing area of the joint. Outerbridge grade 4 defects were found mostly at the posterior part of the radial head. Triceps tendon grafts were used in all 72 patients. In total, 38.9% (n = 28) of the patients showed a radial-sided capsular lesion with an arthroscopic view from the anteroulnar portal. Another 19.4% (n = 14) had a detachment of LCLC, with the joint being visible after arthroscopy while exposing the CEO during the open part of the surgery. Thus, 58.3% of the patients exhibited a defect in the CEO during revision surgery. In addition, 3 patients had local scarring, and 2 patients presented with apparent thinning of the CEO at the insertion point.
Postoperative Findings
Patients returned to work after a mean of 18.9 weeks after surgery (range, 0-52 weeks). One patient who was self-employed returned to work 3 days after surgery. Five patients received a pension, 3 patients were unemployed, and 3 patients could not return to work at the time of the follow-up appointment. Pain-related NSAID intake lasted a mean of 5.4 weeks (range, 1-52 weeks). Four patients still took NSAIDs for elbow pain, if required. The average number of physiotherapy sessions was 29 (range, 3-150 sessions), with 4 patients still undergoing physiotherapy at follow-up. None of the patients with ongoing oral pain medication or physiotherapy needed additional surgery. When asked, from the patients’ point of view, the final clinical result was reached at a mean of 24 weeks after revision surgery (range, 4-96 weeks) (Figure 3).

Mean duration of time before patients returned to work, for nonsteroidal anti-inflammatory drug (NSAID) intake, and for achievement of final clinical results as well as the average number of physiotherapy sessions.
Functional Outcomes
The SEV was 78.9% (range, 20% to 100%) (Figure 4). The patients’ average evaluation of their current condition at the final follow-up was good, with 75% rating it either good or excellent (Figure 5). A total of 43.1% rated the clinical results and status of their elbow as excellent. From among the 49 patients who underwent clinical examinations, 1 elbow joint (2%) was evaluated as unstable, with positive findings in the posterolateral rotatory drawer test, chair push-up test, and tabletop relocation test. However, the instability did not bother the patient, and he was satisfied with the results of the surgery. The other 48 patients did not show any signs of PLRI during clinical examination at the final follow-up.

Subjective elbow value (SEV) (%). Each patient is represented by a dot. The thick gray line represents the mean, and the error bars represent SD.
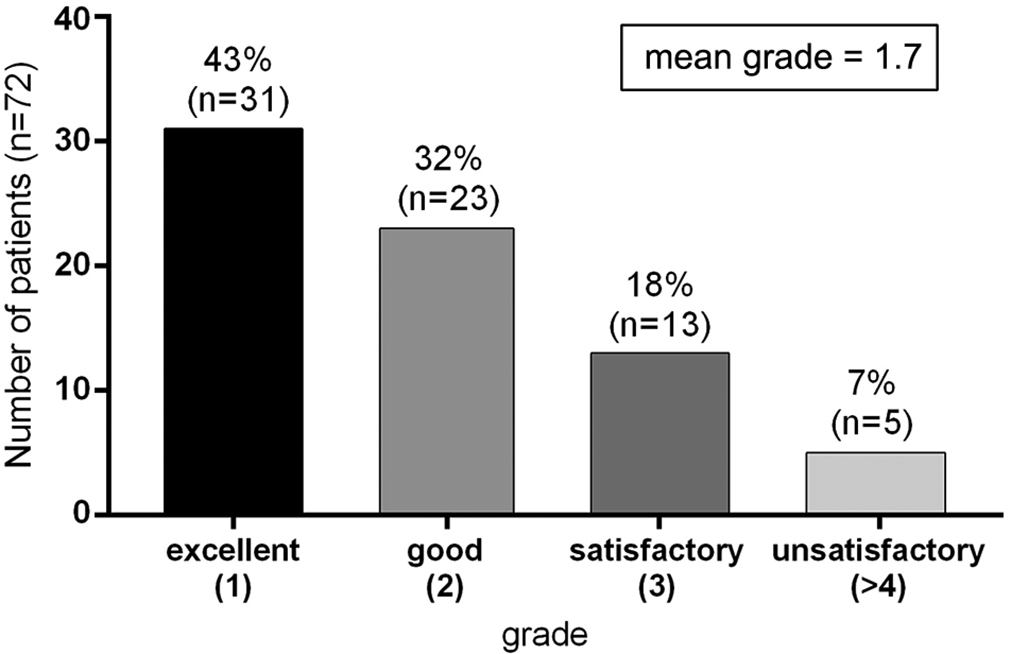
Patient satisfaction concerning postoperative outcomes. Grades 4-6 were rated as unsatisfactory.
The mean maximal grip strength was 33.9 kg (range, 8-76 kg) on the operated side and 36.7 kg (range, 20-65 kg) on the nonoperated side. A total of 65% (n = 32) of the patients reached their maximal strength without pain; 15 patients (31%) complained of mild pain, and 2 felt pain before reaching maximal strength. A deficit in elbow extension was detected in 8 patients (16%).
The mean MEPS score was 78.6 (range, 45-100). The PRTEE reached an average of 21.5 (range, 0-66.5). The mean Placek score was 2.2. The average QuickDASH score was 20.4 (range, 0-81.8). There were no significant differences in scores between patients with or without cartilage damage (MEPS, 77 vs 80.2 [P = .456]; PRTEE, 22 vs 20.9 [P = .536]; QuickDASH, 21.8 vs 19 [P = .589], respectively).
Complications
In total, 13.9% of the patients underwent revision surgery after LUCL reconstruction. The complications were divided into major and minor revisions. Major revisions were performed for 9 patients. One patient underwent arthroscopic arthrolysis. In 1 patient, a compromising suture anchor inserted during LUCL reconstruction had to be retrieved; 2 patients had open reinsertion of the CEO because of insufficient healing, and 5 patients underwent a second LUCL reconstruction with an autologous gracilis tendon graft owing to insufficiency of the triceps tendon graft. Their scores at 2 years were similar to those of patients without complications (MEPS, 79.3 vs 78 [P = .563] and QuickDASH, 22.3 vs 18.4 [P = .498], respectively). One patient needed a minor revision to excise a suture granuloma.
Discussion
In patients suffering from prolonged pain after open release of the CEO without subsequent reconstruction procedures, PLRI should be expected. Revision surgery with LUCL leads to a decline in pain and functional improvements, including high patient satisfaction.
We evaluated 72 patients with PLRI of the elbow joint after exclusive open CEO release. The LCLC has immediate proximity to the attachment site of the CEO, specifically the extensor carpi radialis brevis (ECRB), and is therefore prone to injury during either local injection or surgical release. 11,21 In our study, all patients were externally treated by open release without subsequent reconstruction of the CEO as primary surgery. To our knowledge, our study is the largest case series of patients with PLRI who underwent open release of the CEO via the Hohmann procedure.
Morrey was the first to describe PLRI as a major complication after open release of the CEO in 1992. 24 In that study, 13 patients underwent surgical revision after unsuccessful operations for LE. The 4 patients diagnosed with some type of lateral instability underwent either LCLC plication (3 patients) or LCLC reconstruction (1 patient), with 3 of the 4 patients achieving satisfactory results. However, the outcome of the patient who underwent LCLC reconstruction was unsatisfactory. In our study, 75% of the patients achieved good-to-excellent results.
Although Oki et al 28 found that patients benefited from arthroscopic debridement of the ECRB up to 24 months after surgery, revision surgery should be advocated when clinical examination reveals PLRI. Since clinical evaluation of subtle elbow instability is often difficult in patients who are awake, because of their apprehension, 2 clinical examination under anesthesia and diagnostic arthroscopy can help determine PLRI and rule out concomitant injuries, such as cartilage defects, arthrosis, plica syndrome, or medial instability, which may mimic PLRI. Although presumably not relevant for the development of PLRI, we found multiple pathologies that were not addressed during the index surgery. Organ et al 30 described 34 patients with continuous pain after surgery for LE. In 27 of the 34 patients who underwent salvage surgery after failed surgical interventions for LE, no scarring of the ECRB was detected, leading to the assumption that initial surgery may have been flawed. Their findings match our experience that surgeons should be suspicious for surgical inaccuracy and PLRI in patients presenting after surgical release of the CEO without reconstruction (Hohmann procedure), without clinical improvement after surgery and persistent pain.
In our series, along with the findings of Shim et al, 43 multiple local corticosteroid injections were observed as a risk factor for the development of chronic lateral elbow instability. The role of CEO degeneration in the development of LCLC insufficiency and subsequent PLRI remains unclear, although Bredella et al 6 suggested a coherence of LCLC insufficiency in patients with chronic LE.
For 93% of the patients, the use of an autologous triceps tendon led to the restoration of elbow stability. In our opinion, the triceps tendon has several advantages. First, we were able to connect the posterolateral and soft spot portals and lengthen the incision. Second, we did not observe any complications related to either the approach or the graft. We believe that it is important to stay far enough away from the olecranon tip when harvesting the tendon. From our experience, lateral harvesting may cause persistent pain. In addition, the side-to-side suture of the triceps seems to be important to fully regain strength.
Many authors have suggested primary LUCL reconstruction as a feasible procedure that produces excellent results for traumatic PLRI. 18,29,41 In our study, the results of LUCL reconstruction as revision surgery were evaluated as good, and the SEV reached a mean of 78.9%. The mean MEPS score was 78.6. In a systematic review of surgical treatment for patients suffering mainly from traumatic PLRI, the mean MEPS score was 91, with excellent results in 61% of the patients. 3 Chanlalit and Dilokhuttakarn 9 performed LUCL reconstruction in 6 patients with atraumatic PLRI without prior surgery and found an average postoperative MEPS of 97.5%.
Chanlalit and Dilokhuttakarn 9 described a postoperative QuickDASH score of 9, while our patients reached a score of 20.4. However, neither Anakwenze et al 3 nor Chanlalit and Dilokhuttakarn characterized the patients’ workloads. In our study, 83.3% of the patients stated that their elbows had a heavy workload. This circumstance might contribute to the fact that, in our series, LUCL reconstruction for iatrogenic PLRI produced good but inferior results compared with traumatic as well as noniatrogenic reconstructions described in the literature. 19,42 Nevertheless, even with slightly worse functional outcomes compared with noniatrogenic reconstructions in the literature, 97.2% of the 72 patients (n = 70) available for follow-up in our study would undergo LUCL reconstruction as revision surgery after failed open release of the CEO again.
We experienced a complication rate of 14%. Anakwenze et al 3 stated an overall complication rate of 11% in their systematic review, with most patients suffering from traumatic PLRI. Since our patients had previous surgery and some patients suffered from focal cartilage defects, LUCL reconstruction in patients with prior surgery did not lead to a higher risk for postoperative complications. In addition, a second reconstruction of the LUCL with an autologous gracilis tendon graft helped to achieve acceptable results in patients suffering from triceps graft insufficiency. We believe that the high reoperation rate in our series is associated with prior surgery, older age, and the number of corticosteroid injections. The focal cartilage defects found in 24% of the patients might have also influenced clinical outcomes. Smith et al 45 hypothesized that inflammatory changes, such as early osteoarthritis, lead to the production of proinflammatory cytokines. This theory may explain the impaired healing of the CEO and insufficiency of the triceps tendon graft in patients with cartilage changes, although we did not find any significant differences in the postoperative outcomes of patients with or without cartilage defects. However, 3 of 5 patients undergoing rerevision surgery due to graft insufficiency showed Outerbridge grade 4 cartilage lesions.
Typically, patients suffering from traumatic PLRI are younger than those suffering from atraumatic PLRI. 3,19 Therefore, age and degenerative changes may be associated with inferior clinical outcomes.
Limitations
Our study has several limitations. First, this was a retrospective evaluation. The patients did not provide any functional scores before LUCL reconstruction; therefore, changes in elbow status could not be measured. Second, this study did not include a detailed assessment of the MRI conducted prior to revision surgery. The accuracy and reliability of MRI in this cohort are therefore missing. In addition, only 49 patients were available for clinical examinations, and an additional 23 patients were interviewed by telephone. The patients followed up by telephone could not be evaluated for ongoing instability of the elbow, which represents a significant limitation. However, we believe that good patient-related outcome measures (eg, QuickDASH and PRTEE scores), high satisfaction with LUCL reconstruction, and subsequent rehabilitation suggest that these patients did not suffer from ongoing problems such as instability. If ongoing pain was present, we believe that these patients would have made follow-up appointments to express their complaints.
In addition, we did not ask the patients whether the initial pain leading to open release of the CEO differed from the pain after surgery, as suggested by Morrey. 24 Unfortunately, the study’s retrospective design did not allow for a detailed description of the clinical evaluations or provide indications prior to primary surgery. Therefore, we cannot conclude whether PLRI occurred during surgery or was present beforehand, but we believe that the latter was less common. Another limitation is the inclusion of patients with focal cartilage damage, which might have contributed to the revision rate of 12.5% and the inferior clinical outcomes. However, the MEPS of patients who underwent a second revision with a gracilis tendon graft did not differ significantly from that of patients without complications after LUCL reconstruction, justifying a second reconstruction of the LUCL with a gracilis tendon graft in this subgroup of patients.
Conclusion
Persistent pain caused by PLRI after open release without subsequent reconstruction of the CEO is not uncommon. Revision surgery with ligamentous reconstruction leads to pain relief and functional improvements. However, chronic changes might increase the risk of complications such as graft insufficiency. Previous open release of the CEO without reconstruction, independent of the underlying pathology, is a risk factor for worse clinical outcomes after open LUCL reconstruction using a triceps tendon graft compared with traumatic or primary LUCL reconstructions.
Footnotes
Acknowledgment
The authors thank Dr Ellermann, head of the Arcus Sportklinik, for his support and the ability to perform clinical research.
Final revision submitted September 25, 2021; accepted October 3, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Ethics Committee Landesärztekammer Baden-Württemberg, Stuttgart, Germany (reference No. F-2014-061).