
Abstract
Background:
The cleft sign (CS) and bone marrow edema (BME) are considered magnetic resonance imaging (MRI) findings signifying a pubic pathology, which is associated with groin pain; however, their relationship with bony morphology related to femoroacetabular impingement (FAI) has not been established.
Purpose:
To investigate the prevalence of CS and BME in symptomatic patients with acetabular labral tears and assess their possible association with bone morphology and sport-specific activities.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
This study enrolled 418 patients (469 hips) undergoing hip arthroscopic surgery for labral tears. Also included were patients with labral tears in the setting of either hip dysplasia or borderline hip dysplasia who were undergoing endoscopic shelf acetabuloplasty combined with hip arthroscopic labral repair, cam osteoplasty, and capsular plication. All patients were screened for superior CS (SCS), inferior CS (ICS), and BME of the ipsilateral side of the pubis using 3-T MRI. We measured the following angles: lateral center edge (LCE), Sharp, Tönnis, vertical-central-anterior, and alpha. Then, we evaluated the relationship between patient characteristics and abnormal findings on MRI scans (preoperatively vs 1 year postoperatively).
Results:
An overall 397 hips were included: 200 in men and 197 in women (mean ± SD age, 35.3 ± 16.0 years). There were hips in 214 athletes (53.9%) and hips in 183 nonathletes (46.1%). MRI findings revealed SCS, ICS, and BME in 18 (4.5%), 13 (3.3%), and 34 hips (8.6%), respectively. Abnormal MRI findings at the pubis were seen more often in athletes than nonathletes (23.8% vs 3.3%), and contact sports athletes had the most frequent abnormalities. There was no SCS in patients with an LCE angle <22°. SCS was more frequently seen in those who had an alpha angle ≥71°. More than 60% of abnormal findings at the pubis diminished after arthroscopic surgery that included FAI correction and labral repair.
Conclusion:
In patients with labral tears, CS and BME were seen more frequently in athletes versus nonathletes, especially contact athletes with FAI-related bony abnormalities. More than 60% of abnormal MRI pubis findings resolved after arthroscopic treatment of FAI.
The Doha agreement states that groin pain includes adductor-, iliopsoas-, pubic-, and hip-related groin pain. 30 Pubic-related groin pain particularly affects the long-term playing abilities of soccer players. While 21% of other groin pain causes time loss <28 days, 18 50% of pubic-related groin pain results in time loss >28 days, making it a difficult issue for athletes to overcome.
Patients with pubic-related groin pain often show a cleft sign (CS) on magnetic resonance imaging (MRI) scans, specifically in the pubic symphysis, which comprises the superior CS (SCS) and the inferior CS (ICS). An SCS indicates a tear in the rectus abdominis/adductor longus, and an ICS indicates a tear from the short adductors to the margin of the pubic ramus. 6,19 CS and bone marrow edema (BME) of the pubis are strongly associated with hip and groin pain in athletes. 11,24
Several studies have investigated the relationship between femoroacetabular impingement (FAI) and osteitis pubis. It has been reported that repetitive loading of the symphysis secondary to cam morphology and impingement was likely a precursor to groin pain and athletic pubalgia via increased motion at the symphysis pubis. 4,25 Despite these findings, there is a lack of clear understanding regarding the relationship between CS/BME and (1) bone morphology and (2) sport-specific activities.
In this study, we aimed to investigate the prevalence of CS and BME in symptomatic patients with acetabular labral tears and assess whether the presence of CS and BME is associated with bone morphology and sport-specific activities. We hypothesized that abnormal pubic findings would be more frequently observed in contact sports athletes and those with FAI bony morphology.
Methods
Patient Recruitment
The protocol for this study received institutional review board approval. Between January 2015 and March 2019, 418 patients (469 hips) undergoing hip arthroscopic surgery for acetabular labral injury were enrolled in this study. Patients with synovial chondromatosis and osteoarthritis (19 hips from 19 patients), no preoperative MRI scan (9 hips from 9 patients), and a Tönnis grade >1 (44 hips from 43 patients) were excluded. Several studies 1,3,10,13,21 have shown that patients with hip dysplasia, such as borderline developmental dysplasia of the hip (BDDH) and developmental dysplasia of the hip (DDH), frequently have cam deformities. As such, we included patients with BDDH and DDH as well as FAI in this study, although the recent literature has not provided clarity on the frequency and relevance of osteitis pubis in patients with dysplastic hips. Ultimately, 397 hips in 350 patients were included in the study. Informed consent was given by all participants.
We defined athletes as patients with University of California–Los Angeles activity score ≥8. 28,32 The athlete group consisted of 214 hips, and the nonathlete group consisted of 183 hips. The athlete group was divided into 2 groups according to its contact sports activity. For the purpose of this study, contact sports were defined using the American Academy of Pediatrics Committee on Sports Medicine criteria. 2,17 There were 96 athletes (96 hips) who played contact sports. Figure 1 summarizes the study enrollment process.

Flowchart showing the recruitment of patients undergoing hip arthroscopy. MRI, magnetic resonance imaging.
Imaging Assessments
Two orthopaedic surgeons (K.N. and S.T.), who were blinded to the clinical data, performed all imaging assessments.
Radiographic Assessment
The radiographic parameters were measured at the time of initial presentation using a picture archiving and communication system. All patients were subjected to 3 plain radiographic projections: an anteroposterior pelvic view to check the lateral center-edge (LCE), 31 Sharp, alpha, and Tönnis angles; 2 modified Dunn views to measure the alpha angle (hip flexion at 45° and external rotation at 20°; hip flexion at 45° and external rotation at 45°); and a false-profile view to measure the vertical-central-anterior (VCA) angle. 9 The anteroposterior pelvic view was obtained with the patient in the supine position on the radiographic table and both lower extremities internally rotated at 15°. 9 The modified Dunn views were obtained with the patient in the supine position at an angle of 45° of hip flexion and 20° of abduction with neutral rotation. The false-profile view was obtained with the patient standing at an angle of 65° between the pelvis and the film, as described previously. 8
We used the LCE angle to define the lateral coverage of the acetabulum. 31 The femoral neck-shaft angle was calculated by imagining a line through the center of the neck and head and a line parallel to the femoral shaft that was determined via the direction of the shaft below the lesser trochanter. 1 We used the Tönnis angle to measure acetabular inclination 27 and the Sharp angle to measure the acetabular index. 26 The VCA angle helped to measure the anterior coverage of the acetabulum, 16 and the alpha angle was used to identify any cam-type impingement.
The presence of a cam deformity was indicated by an alpha angle >55° on plain radiographs. The largest angle among the anteroposterior pelvic and 2 modified Dunn view alpha angles was used. 20,22
MRI Assessment
Supine MRI scans with the lower extremities positioned at 15° of internal rotation were obtained preoperatively and at 1 year postoperatively for all patients. All images were acquired using 3.0-T MRI (MAGNETOM Skyra; SIEMENS Healthcare). The standardized MRI evaluation protocol was as follows:
Coronal (T2-weighted fat saturation [T2 FS]; repetition time/echo time [TR/TE], 4140/91 milliseconds; field of view [FOV], 360 × 360 mm; slice thickness, 4.0 mm; matrix, 358 × 448) and proton density (PD; TR/TE, 1100/30 milliseconds; FOV, 200 × 200 mm; slice thickness, 1.5 mm; matrix, 256 × 320)
Axial oblique (T2 FS; TR/TE, 23/14 milliseconds; FOV, 200 × 200 mm; slice thickness, 0.5 mm; matrix, 307 × 384)] and PD (TR/TE, 1100/27 milliseconds; FOV, 160 × 160 mm; slice thickness, 1.5 mm; matrix, 256 × 320)
Sagittal oblique (T2 FS; TR/TE, 23/14 milliseconds; FOV, 200 × 200 mm; slice thickness, 0.5 mm; matrix, 307 × 384 and PD TR/TE, 1100/27 milliseconds; FOV, 160 × 160 mm; slice thickness, 1.5 mm; matrix, 256 × 320)
The axial oblique slice was parallel to the femoral neck axis, and the sagittal oblique slice was inclined at an angle of 10°.
The SCS was used to describe the hyperintense linear signal from the symphyseal cleft parallel to the inferior margin of the superior pubic ramus 19 ; similarly, the ICS was used to describe the hyperintense linear signal from the symphyseal cleft parallel to the inferior margin of the inferior pubic ramus on T2 FS images. 23 We checked the presence of pubic BME and measured its extent using the coronal sequences on T2 FS at the intersection of the line where the longest distance of increased signal intensity was visible and the pubic symphyseal bony joint surface. 5 A positive BME finding was defined as an involved region ≥1 cm on the coronal sequences (Figure 2). 25

MRI findings: (A, B) superior and inferior cleft signs and (C) bone marrow edema. Preoperative supine MRI scans were obtained for all patients, with the lower extremities internally rotated at 15°. BME, bone marrow edema; ICS, inferior cleft sign; MRI, magnetic resonance imaging; SCS, superior cleft sign.
Statistical Analysis
A power analysis was performed a priori using G*Power (Version 3.1; Universitat Dusseldorf). Branci et al 5 reported that CS was positive in 13.7% of soccer players and 2.5% of other sports athletes. Based on the assumption that the soccer players and the other athletes were compared using the chi-square test with alpha level set as .05, the effect size was calculated as a d of 0.32, and 128 hips were needed to reach to a power of 0.80. We decided to include >200 hips from athletes in this cohort; thus, the actual power was 0.95.
The inter- and intraobserver reproducibility of the imaging parameters was evaluated. For intraobserver reliability, 1 of the 2 reviewers (K.N.) measured each radiograph or MRI scan 3 times, with an interval of at least 1 week between the measurements.
We calculated the intraclass correlation coefficients and corresponding 95% CIs to quantify inter- and intraobserver reliability for continuous variables. The weighted kappa value was used to determine positive or negative CS and BME. Using the Landis and Koch 15 standards for the kappa statistic, we interpreted the strength of agreement per the following intraclass correlation coefficient values: 0.81 to 1.0, almost perfect; 0.61 to 0.80, substantial; 0.41 to 0.60, moderate; and 0.21 to 0.40, fair.
The relationship between CS or BME and patient characteristics (including sports activity and radiographic measurements) was analyzed using the Student t test, Mann-Whitney U test, chi-square test, or Fisher exact test, as appropriate, and the Kolmogorov-Smirnov test to assess the assumption of normal data distribution between the groups. A receiver operating characteristic curve analysis was performed to decide the cutoff value; this was defined as the value with the highest Youden index. A P value <.05 was considered statistically significant. SPSS (Version 21; IBM Corp) was used for the analyses.
Results
Of the 350 study patients, 177 were male (200 hips) and 173 were female (197 hips). The mean ± SD age was 35.3 ± 16.0 years (range, 14-77 years), and the mean LCE angle was 28.1° ± 9.0° (range, 0°-58°).
Inter- and Intraobserver Reliability
The inter- and intraobserver reliability of the imaging measurements is shown in Table 1.With the exception of VCA angle (moderate reliability), the reliability of the measurements was indicated as substantial to almost perfect. For our analysis, we adopted the measurements by 1 of the reviewers (K.N.), who had >12 years of experience as an orthopaedic surgeon.
Inter- and Intraobserver Reliability of the Imaging Measurements a

a ICC, intraclass correlation coefficient; LCE, lateral center edge; MRI, magnetic resonance imaging; VCA, vertical-center-anterior.
b All ICC values: P < .001.
c All kappa values: P < .001.
Presence of CS and BME in the MRI Analysis
We observed SCS, ICS, and BME of the pubis in 18 (4.5%), 13 (3.3%), and 34 hips (8.6%), respectively. Among these, 1 hip showed all 3 parameters. BME and ICS were found together in 3 hips, and BME and SCS were found together in 3 hips. Overall, 58 hips (14.6%) showed at least 1 of these findings.
Sports Activity
The athlete group (23.8%) showed more frequent abnormal MRI findings at the pubis than did the nonathlete group (3.3%; P < .001; odds ratio, 9.5 [95% CI, 3.9-22.6]). Within the athlete group, there were more frequent abnormal MRI findings among contact sports athletes than noncontact athletes (41.7% vs 9.3%; P < .001; odds ratio, 6.9 [95% CI, 3.3-14.6]) (Table 2). The sports activity of all patients is shown in Appendix Table A1.
Prevalence of Abnormal MRI Findings at Pubis in Contact vs Noncontact Athletes a
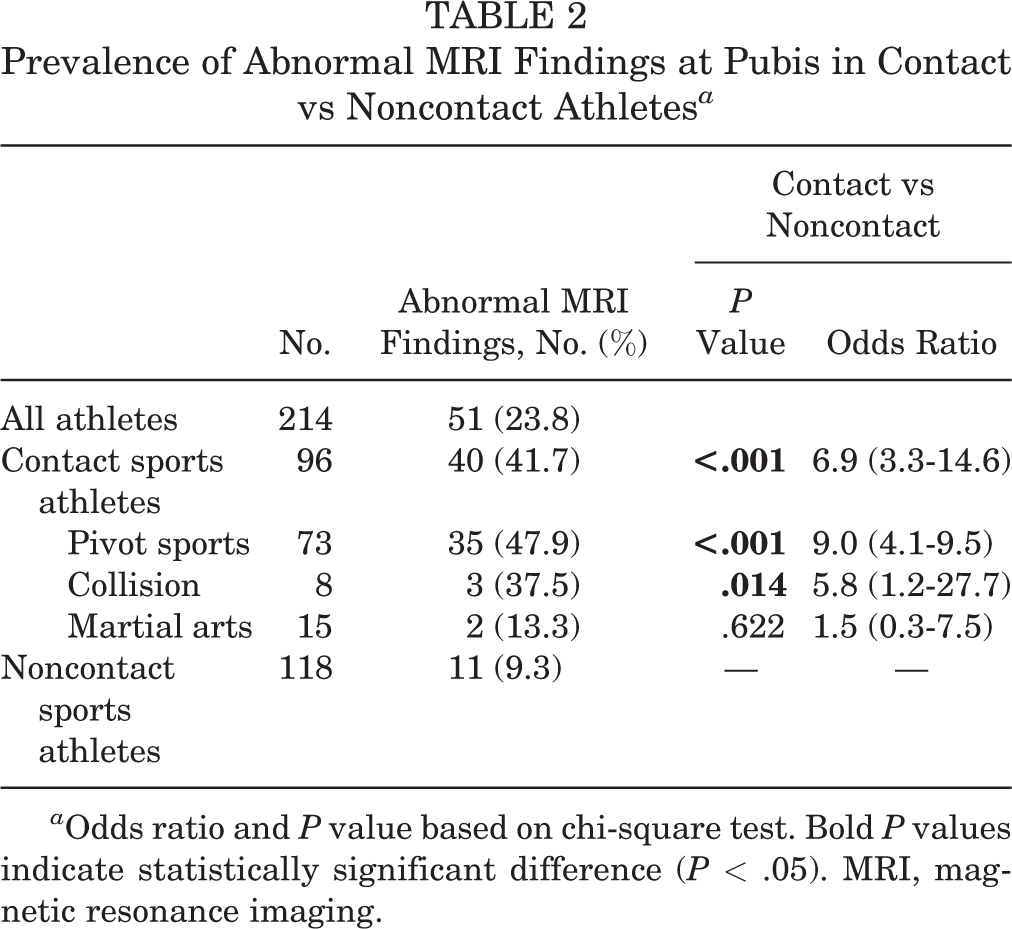
a Odds ratio and P value based on chi-square test. Bold P values indicate statistically significant difference (P < .05). MRI, magnetic resonance imaging.
Radiographic Parameters
We observed that patients with a positive SCS had a significantly smaller Sharp angle and larger VCA angle than did patients with a negative SCS. There was no significant relationship between the radiographic measurements and ICS or BME (Table 3).
Radiographic Parameters of the Superior Cleft Sign, Inferior Cleft Sign, and Bone Marrow Edema a
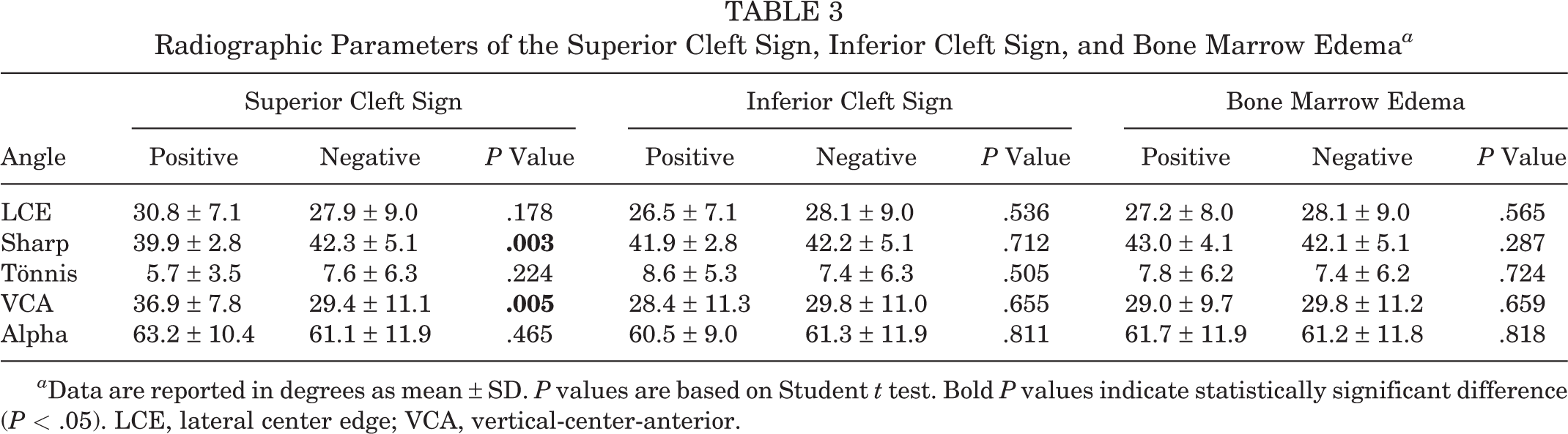
a Data are reported in degrees as mean ± SD. P values are based on Student t test. Bold P values indicate statistically significant difference (P < .05). LCE, lateral center edge; VCA, vertical-center-anterior.
Table 4 shows the cutoff values of the radiographic parameters between positive and negative SCS. There was no SCS in patients with an LCE angle <22° (0%; P = .018), and it was rarely seen in patients with a VCA angle <37° (2.3%; P = .001). SCS was more frequently seen in those who had an alpha angle ≥71°, but this did not reach statistical significance (P = .06) (Table 5).
Cutoff Values of Each Parameter in Superior Cleft Sign a

a AUC, area under receiver operating characteristic curve; LCE, lateral center edge; VCA, vertical-center-anterior.
Contribution of FAI on Superior Cleft Sign a

a Bold P values indicate statistically significant differences (P < .05). FAI, femoroacetabular impingement; LCE, lateral center edge; VCA, vertical-center-anterior.
b Chi-square test.
Since SCS was not recognized at an LCE angle <22°, we investigated the SCS incidence in patients with DDH (LCE angle <20°; n = 75), BDDH (20° ≤ LCE angle < 25°; n = 49), and FAI (LCE angle ≥25°; n = 273). We found some statistically significant tendencies: SCS occurred in BDDH (10.2%) and FAI (4.8%) but not in DDH (0%) (Table 6). Moreover, we found significant differences between some of the groups: FAI vs BDDH (P = .16), FAI vs DDH (P < .01), and DDH vs BDDH (P < .01).
Frequency of MRI Abnormal Findings in DDH, BDDH, and FAI a

a BDDH, borderline developmental dysplasia of the hip; DDH, developmental dysplasia of the hip; FAI, femoroacetabular impingement; LCE, lateral center edge; MRI, magnetic resonance imaging.
b DDH was defined as an LCE angle <20°; BDDH, as 20° ≤ LCE angle < 25°; and FAI, as LCE angle ≥25°.
c Chi-square test. Bold P values indicate statistically significant difference (P < .05).
Postoperative Change on MRI Scans of CS and BME
Among the patients who showed abnormal findings on preoperative MRI scans (57 hips), we examined the postoperative MRI scans of 44 hips (follow-up, 77.2%) at a mean 9.0 ± 3.0 months after surgery. MRI findings of SCS, ICS, and BME were reduced in more than 60% of the hips, which was statistically significant (P < .001, P = .026, and P < .001, respectively). There were no statistical differences between the patients with postoperative positive and negative CS in terms of their radiographic parameters. There were no cases with postoperative intensity changing from negative to positive.
Discussion
There were 4 major findings in this study. First, pubis MRI abnormalities were seen in 23.8% of patients undergoing hip arthroscopy for labral tears. Of these patients, pubis MRI abnormalities occurred in 41.7% of the contact sports group and 9.3% of the noncontact sports group. Second, SCS was more frequent in patients with a VCA angle >37°, a Sharp angle <43°, and a Tönnis angle <8°, suggesting that SCS may be associated with deeper acetabular coverage. Third, patients with an alpha angle ≥71° were likely to show a positive SCS more frequently. Fourth, >60% of CS and BME findings were reduced on the postoperative MRI scans obtained after hip arthroscopic surgery, which involved labral repair and FAI correction. Based on these observations, CS and BME appear to be significantly associated with contact sports activity and FAI-related bone morphology.
CS and BME have frequently been observed in soccer players. In a series on 100 consecutive soccer players, Cunningham et al 11 reported ICS in 88% of the players and BME in 91% of the players. This suggests that the entities are mechanically related and that osteitis pubis and adductor dysfunction frequently coexist. Murphy et al 19 investigated 25 patients with a clinically suspected sports hernia and found SCS in 19, ICS in 9, and BME in 12 patients; notably, all 25 had groin crease and lower abdominal pain, and their sports activities were not known. Byrne et al 7 reported isolated SCS in 42% of the patients, isolated ICS in 7%, and osteitis pubis in 11% from a sample of 45 patients with chronic groin pain as a result of field-based kicking sports. These findings suggest that microtearing of the attachment of the rectus abdominis–adductor longus is the most common primary injury and the resultant instability causes propagation and short adductor microtearing. Our findings support this evidence; among 53 hips of 53 soccer players in our study, 10 (18.9%) were SCS positive, 7 (13.2%) were ICS positive, and 18 were BME positive. Also, there were 96 hips from contact sports players, of which 16 (16.7%) showed a positive SCS; 8 (8.3%), a positive ICS; and 23 (24.0%), a positive BME. These observations support the claim that SCS and ICS are more prevalent in contact sports players than noncontact sports players.
Krishnamoorthy et al 14 reported a low prevalence (1.8%-2.6%) of pubis joint symphysis abnormalities on imaging in patients with FAI syndrome. These patients may demonstrate significantly inferior clinical outcomes and persistent postoperative pain after primary hip arthroscopy for FAI syndrome. However, Saito et al 25 stated that the prevalence of osteitis pubis was 67% and that of BME was 36% in 25 symptomatic soccer players undergoing hip arthroscopic surgery for FAI correction. Saito et al also noted that BME was reduced on the final postoperative follow-up MRI scan in all patients who were preoperatively BME positive. Moreover, in a recent series of 1091 athletes with groin pain, multiple MRI findings, including CS and pubic BME, were found in 56.5% of athletes. 24 The authors noted that body mass index and CS were independently associated with a delayed return to play. Our findings support the claim that contact sports players (including soccer players) show more frequent BME: specifically, contact sports players with FAI had a higher prevalence of SCS, ICS, and BME than did noncontact sports players. Therefore, we considered that vigorous, sudden, and violent kicking, pivoting, and twisting motions during pivot and collision sports likely contribute to the increased transfer stress surrounding pubic symphysis in contact sports players.
It has not yet been established whether the abnormal bony morphology of the hip is associated with CS and BME. In a cadaveric study, Birmingham et al 4 demonstrated that simulated cam impingement increased the motion of the pubic symphysis, supporting the hypothesis that impingement with a constrained range of motion of the hip might contribute to osteitis pubis as a subset to the initial impingement. Furthermore, Saito et al 25 reported that alpha angle was significantly larger among patients with pubic BME as compared with those with no BME. Varada et al 29 evaluated patients with FAI and found that male sex, history of sports participation, and morphology of the femoral cam with an alpha angle ≥60° were significant predictors of damage patterns of athletic pubalgia on MRI scans. Notably, in our study, we did not observe SCS in patients with an LCE angle <22°, and we determined that SCS was more frequent in patients having cam impingement and excess acetabular coverage of the socket. These findings support the association between FAI and CS or BME.
Saito et al 25 showed that pubic BME was reduced postoperatively among all the soccer players in their study. Similarly, our findings revealed that >60% of CS and BME findings had diminished after surgery. These observations suggest that abnormal pubic change is associated with pincer- and cam-type impingement of the hip and can be treated via arthroscopic surgery by resolving FAI, which is associated with pubic CS and BME. However, it may be affected by the period of rest and core rehabilitation as well, rather than FAI surgery.
Our findings are clinically relevant. Pubic-related groin pain is a known cause of long-term time and functional loss for soccer players. 12 This study added to this evidence by revealing that CS and BME are associated with FAI-related bony abnormalities. FAI is associated with the motion of the pubic symphysis and BME of the pubis 21 ; therefore, it is possible that FAI is a significant contributory factor of pubic-related groin pain in contact sports players. FAI correction surgery may be one of the suitable options for contact sports players who experience long-term pubic-related groin pain if nonoperative treatment fails. Further studies, such as large-scale and prospective studies, are required to confirm the mechanism, pathology, and epidemiology of FAI in pubic-related groin pain. However, it is still inconclusive whether FAI correction surgery actually treats the groin pathology, as some patients with groin strain may simply benefit from the forced rest or postoperative rehabilitation. Therefore, investigation regarding the role of surgery on groin pathology is still required.
Our study suggests that sports activity is likely a greater risk factor for pubic changes. Branci et al 5 reported that sprinting, kicking, and change of direction induce considerable stress at the adductor musculotendinous complex and seem to play an important role in relation to groin injury mechanisms. In addition, there are a few articles describing that soccer players or National Football League players had much osteitis pubis. 25 From these facts, the reason why sports activity is likely to be a greater risk factor for groin changes may be the strong stress on the pubis when athletes (especially those in contact sports) are exercising. As there is no literature about this as far as we know, further biomechanical cadaver study is needed.
Limitations
This study had several limitations. First, we retrospectively analyzed data that were collected prospectively. Although we conducted 100% preoperative MRI screening using a single 3-T scanner, a retrospective study may inherently have selection bias. Second, we focused on patients with symptomatic FAI and did not include a matched control group of healthy individuals. As healthy hips are heterogeneous, it was difficult to analyze the radiographic correlation between FAI and SCS, ICS, and BME. Note also that this was a retrospective study that investigated symptomatic patients with labral tears undergoing hip arthroscopic surgery. However, some patients may have a symptomatic groin strain resulting in incidental findings of FAI on MRI scans, while some may have symptomatic FAI but with asymptomatic MRI findings at the adductor/rectus insertion. Nonetheless, there might be some degree of bias in the previous studies conducted so far, and the strength of our study is that it comprised the largest number of patients with systematic screening using 3-T MRI pre- and postoperatively. Third, even though the interobserver reliability was “moderate,” we used the recordings of only 1 observer because he was more experienced. Fourth, we did not record how many people actually experienced groin pain or had tenderness over the symphysis.
Conclusion
The study findings indicated that in patients with labral tears, CS and BME are seen more frequently in athletes versus nonathletes and especially in contact athletes with FAI-related bony abnormalities. Results also showed that more than 60% of abnormal MRI pubis findings resolve after arthroscopic treatment of FAI.
Footnotes
Acknowledgment
The authors thank Editage for editing and reviewing this manuscript for the English language.
Final revision submitted August 20, 2021; accepted September 16, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.U. is a consultant for Smith & Nephew and ConMed. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Occupational and Environmental Health (H29-220).
APPENDIX
Prevalence of SCS, ICS, BME, and Abnormal MRI Findings at the Pubis During Each Sports Activity a

| Patients, No. (%) | |||||
|---|---|---|---|---|---|
| Total | SCS | ICS | BME | Abnormal MRI Findings | |
| Nonathletes | 183 | 2 (0.7) | 3 (1.6) | 1 (0.5) | 6 (3.3) |
| Athletes | |||||
| Contact sports | 96 | 16 (16.7) | 8 (8.3) | 23 (24.0) | 40 (41.7) |
| Pivot sports | 73 | 14 (19.2) | 7 (9.6) | 21 (28.8) | 35 (47.9) |
| Soccer | 53 | 10 (18.9) | 7 (13.2) | 18 (34.0) | 28 (52.8) |
| Basketball | 15 | 3 (20.0) | 3 (20.0) | 6 (40.0) | |
| Lacrosse | 2 | 1 (50.0) | 1 (50.0) | ||
| Futsal | 2 | 0 (0) | |||
| Hockey | 1 | 0 (0) | |||
| Collision sports | 8 | 1 (8.3) | 0 (0) | 2 (25.0) | 3 (37.5) |
| Rugby | 5 | 1 (20.0) | 1 (20.0) | ||
| American football | 3 | 1 (33.3) | 1 (33.3) | 2 (66.7) | |
| Martial arts | 15 | 1 (6.7) | 1 (6.7) | 0 (0) | 2 (13.3) |
| Karate | 1 | 0 (0) | |||
| Kick boxing | 4 | 1 (20.0) | 1 (20.0) | ||
| Judo | 3 | 1 (33.3) | 1 (33.3) | ||
| Boxing | 1 | 0 (0) | |||
| Sumo | 1 | 0 (0) | |||
| Kendo | 2 | 0 (0) | |||
| Martial arts | 1 | 0 (0) | |||
| Taekwondo | 1 | 0 (0) | |||
| Riot police | 1 | 0 (0) | |||
| Noncontact sports | 118 | 0 (0) | 2 (1.7) | 9 (7.6) | 11 (9.3) |
| Artistic and gymnastics | 29 | 0 (0) | 1 (3.4) | 5 (17.2) | 6 (20.7) |
| Classic ballet | 10 | 2 (20.0) | 2 (20.0) | ||
| Rhythmic gymnastics | 6 | 2 (33.3) | 2 (33.3) | ||
| Dance | 5 | 1 (20.0) | 1 (20.0) | 2 (40.0) | |
| Ballet | 5 | 0 (0) | |||
| Awa dance | 1 | 0 (0) | |||
| Flamenco | 2 | 0 (0) | |||
| Bat-and-ball games | |||||
| Baseball | 10 | 0 (0) | 0 (0) | 1 (10.0) | 1 (10.0) |
| Ball-over-net games | 25 | 0 (0) | 0 (0) | 2 (8.0) | 2 (8.0) |
| Badminton | 9 | 2 (22.2) | 2 (22.2) | ||
| Volleyball | 8 | 0 (0) | |||
| Tennis | 7 | 0 (0) | |||
| Table tennis | 1 | 0 (0) | |||
| Others | 54 | 0 (0) | 1 (1.9) | 1 (1.9) | 2 (3.7) |
| Board sports | |||||
| Surfing | 4 | 0 (0) | |||
| Skiing | 1 | 0 (0) | |||
| Mountaineering | 2 | 0 (0) | |||
| Cycling | |||||
| Road bicycle | 2 | 0 (0) | |||
| Bicycle race | 2 | 0 (0) | |||
| Golf | 12 | 0 (0) | |||
| Running | |||||
| Jogging | 1 | 0 (0) | |||
| Triathlon | 2 | 0 (0) | |||
| Marathon | 4 | 0 (0) | |||
| Athletics | 5 | 0 (0) | |||
| Walking | 2 | 0 (0) | |||
| Weight lifting | |||||
| Weight lifting | 2 | 1 (50.0) | 1 (50.0) | ||
| Gymnasium | 2 | 0 (0) | |||
| Miscellaneous | |||||
| Japanese drums | 3 | 1 (33.3) | 1 (33.3) | ||
| Yoga | 4 | 0 (0) | |||
| Boat racing | 2 | 0 (0) | |||
| Indiaca | 1 | 0 (0) | |||
| Archery | 1 | 0 (0) | |||
| Swimming | 1 | 0 (0) | |||
| Speed skating | 1 | 0 (0) | |||
a BME, bone marrow edema; ICS, inferior cleft sign; MRI, magnetic resonance imaging; SCS, superior cleft sign. Blank cells indicate 0.