
Abstract
Background:
Various methods exist for managing the joint capsule during the Latarjet procedure. Repairing the capsule to the native glenoid rim results in an extra-articular bone block, while repairing it to the remnant coracoacromial ligament stump of the coracoid graft renders it intra-articular. The technique that optimizes patient outcomes is not well defined.
Purpose:
To compare the outcomes of intra-articular and extra-articular bone block techniques for the Latarjet procedure.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
Using PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analyses) guidelines, we queried the PubMed, EMBASE, and the Cochrane Library for all studies reporting outcomes of the Latarjet procedure with a clearly defined method of capsular repair that rendered the coracoid graft intra-articular or extra-articular. The included levels of evidence and degree of heterogeneity in this study precluded meta-analysis. Outcomes of interest included preoperative variables, surgical technique, rehabilitation protocols, functional outcome assessments, recurrent instability, range of motion, and radiographic findings.
Results:
A total of 16 studies including 816 patients were included. A total of 8 studies employed an intra-articular bone block in 338 patients, while the other 8 employed an extra-articular technique in 478 patients. There was variation among studies in reference to baseline patient characteristics, surgical techniques, rehabilitation, methods for assessing patient outcomes, and follow-up times. Rates of postoperative instability were reported in 8 intra-articular (0%, 0%, 2.1%, 2.7%, 3.2%, 5%, 5.4%, 5.9%) and 7 extra-articular (0%, 0%, 1.2%, 2%, 3.9%, 6.3%, 14%) bone block studies. Postoperative osteoarthritis or progression of preoperative osteoarthritis was reported in 5 intra-articular bone block studies (0%, 5.6%, 23.5%, 23.5%, 25%) and 4 extra-articular bone block studies (0%, 1.9%, 5.2%, 8.6%).
Conclusion:
Varying capsular repair methods appeared to provide similar outcomes regarding stability. There was an apparent trend toward higher rates of post-traumatic arthritis among studies in which an intra-articular bone block technique was employed; however, it is possible that this was influenced by substantially different follow-up times between groups and other various sources of heterogeneity among the included studies. There were no studies in the literature directly comparing intra-articular and extra-articular bone block techniques. Large-scale randomized controlled trials or comparative studies are needed to draw stronger conclusions comparing the 2 techniques.
Anterior shoulder instability is a commonly encountered shoulder problem affecting an estimated 1.7% of the general population. 20 In young athletes who sustain a traumatic injury resulting in shoulder instability, the rate of recurrent instability after nonoperative management is as high as 75% to 92%. 6,41,43 Arthroscopic capsulolabral repair has been shown to decrease the recurrence rate to approximately 4% to 51%. 6,21,34,35,40,41 However, glenoid bone loss is encountered in a large proportion of patients with recurrent shoulder instability, and almost 30% of these patients have clinically significant bone loss. 15,39 Bony defects >20% to 25% of the glenoid surface are known to contribute to an unstable glenohumeral joint and are considered “critical glenoid bone loss.” 26 In these cases, soft tissue stabilization alone is often insufficient to restore and sustain shoulder stability over time, and thus a glenoid bone reconstruction procedure may be more appropriate in providing better long-term outcomes.
Bone grafting procedures for shoulder instability with critical glenoid bone loss have increased in frequency over the past 2 decades, especially outside the United States. 11,12,36 Among these, the Latarjet procedure is often considered the gold standard. 12,36 It is thought to provide shoulder stability via the bone block effect produced by the transferred coracoid graft offering increased articulating arc and the sling effect produced by the tensioning of the inferior subscapularis muscle and the transferred conjoint tendon. 18,44 After coracoid fixation, shoulder stability may be further augmented by repair of the anterior-inferior capsule. 44 Capsular repair techniques generally include (1) suturing the medial aspect of the capsule to the remnant coracoacromial ligament (CAL) stump of the transferred coracoid, resulting in an intra-articular bone block, and (2) fixing the medial portion of the anterior capsule to the native glenoid, rendering the bone block extra-articular.
When the capsule is repaired to the CAL, it is effectively elongated by the thickness of the bone block and the length of the CAL stump. However, repairing the capsule to the glenoid tightens the anterior soft tissues, with more tension when there is greater bone loss because of the fixation point on the glenoid, which may affect external rotation. Because capsular repair technique dictates the position of the coracoid graft in relation to the glenohumeral joint, it may influence the risk of postoperative osteoarthritis. Methods that leave the coracoid graft in an extra-articular position prevent it from making direct contact with the articular surface of the humeral head if the capsular repair remains intact and the bone block is placed at or below the level of the native glenoid articular surface. Repairing the capsule to the native glenoid, thereby establishing an extra-articular location of the transferred coracoid bone, has been associated with a decrease in the rate of arthritis at long-term follow-up, compared with historical controls. 7
There is a paucity of literature that has directly compared capsular repair technique outcomes in the setting of a Latarjet procedure. To this end, the purpose of this systematic review was to compare the clinical outcomes after the Latarjet procedure with an intra-articular versus extra-articular bone block position. We hypothesized that intra-articular bone grafting techniques would be associated with less external rotation loss after the Latarjet procedure while extra-articular bone grafts would be correlated with a decrease in the rate of postoperative arthritis.
Methods
A systematic review was performed according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. In February 2019, 2 independent reviewers (H.S.S. and A.L.V.) searched PubMed, EMBASE, and the Cochrane Library using the term “Latarjet.” We sought all studies reporting outcomes of the Latarjet procedure with a clearly defined method of capsular repair. Studies with a capsular repair technique that rendered the coracoid graft intra-articular or extra-articular were included. Articles not published in the English language as well as technique reports and biomechanical studies were excluded. The included levels of evidence and degree of heterogeneity in this study precluded meta-analysis.
After duplicate studies were removed across the 3 databases, titles and/or abstracts were reviewed, and full-text articles were further assessed for eligibility. Data were extracted and cross-checked for accuracy. Outcomes of interest included patient characteristics, preoperative details, surgical technique, rehabilitation protocol, recurrent instability, clinical evaluation, and radiographic findings. Due to heterogeneity among studies in patient populations, surgical techniques, and outcome assessments, quantitative assessment via meta-analysis was not appropriate.
Results
The literature search returned a total of 1201 records. After applying our criteria, 16 studies were included (Figure 1). # The capsular repair technique rendered the coracoid graft intra-articular in 8 studies 2,5,28,30,32,33,38,48 and extra-articular in the other 8 studies. 1,4,7,8,16,31,46,47
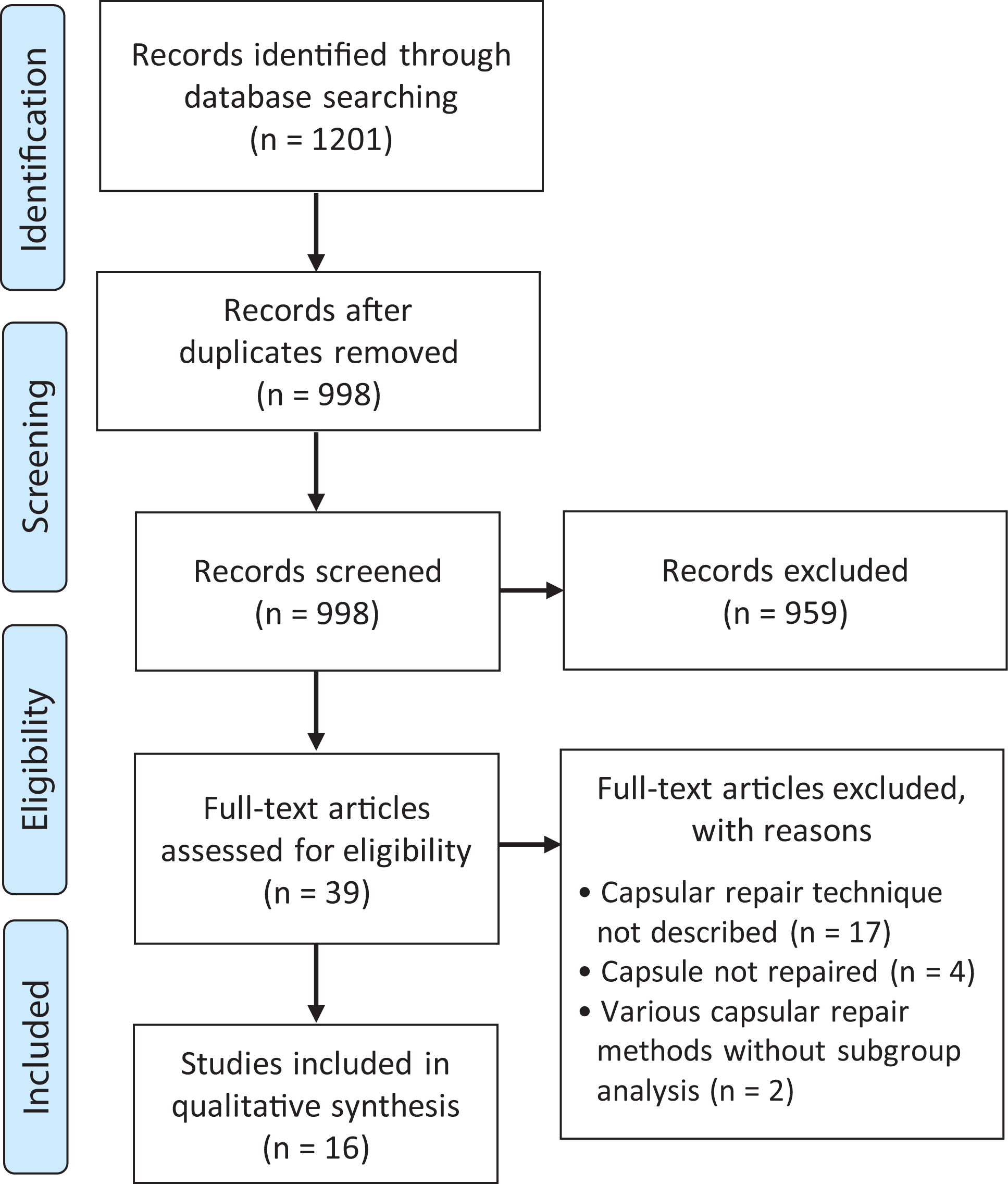
PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analyses) flowchart describing the process for selecting studies included in the review.
Details of the Included Studies
Table 1 provides details of the included studies. Among the studies reporting on an intra-articular coracoid graft position, 2 compared the results of open Latarjet with those of arthroscopic Bankart repair. 38,48 Results from these studies were extracted only for patients who underwent Latarjet. Marion et al 30 compared results after the arthroscopic and mini-open Latarjet; however, they did not explicitly describe the capsular management technique or the position of the bone block in the arthroscopic group. Thus, data were only extracted for patients in the mini-open group. Bonnevialle et al 5 compared 2 surgical revision techniques for recurrent anterior shoulder instability after failed selective capsular repair (SCR): repeat SCR and Latarjet. Similarly, our review only included data from patients with a coracoid transfer procedure. Kee et al 28 compared the clinical outcomes of collision and noncollision athletes who had undergone Latarjet with a uniform capsular management technique. The remaining 3 studies conducted retrospective case series with no comparison groups. 2,32,33 Among studies reporting on the Latarjet procedure with an extra-articular graft position, 2 compared the outcomes of an open versus arthroscopic approach. 31,46 The remaining 6 studies performed retrospective case series with no comparative study groups. 1,4,7,8,16,47
Characteristics of the Included Studies a

a F, female; LOE, level of evidence; M, male; MCSM: Modified Coleman Methodology Score; NR, not reported.
b Values represent the number of patients in whom the capsular management technique was reported and thus included in our analysis.
c Including patients who underwent a surgery other than Latarjet.
Preoperative Evaluation
All included studies comprised patients who underwent Latarjet for recurrent anterior shoulder instability; however, there were differences in their respective patient populations (Table 2). A total of 8 studies reported the number of patients who had undergone a prior ipsilateral shoulder instability surgery, 1,5,7,16,28,30,31,38 and 2 studies excluded such patients. 4,32 The remaining 6 studies 2,8,33,46 –48 did not report these values. A total of 12 studies provided details regarding glenoid bone loss, ** and 4 studies did not. 1,2,31,48
Preoperative Evaluation a

a Data are reported as number of shoulders (%) or mean ± SD (range) unless noted otherwise. A, arthroscopic; ASI, anterior shoulder instability; C, collision; Excl, excluded; GBL, glenoid bone loss; ISIS, Instability Severity Index Score; NC, noncollision; NR, not reported; O, open; SCR, selective capsular reconstruction.
b Reported as mean % GBL ± SD (range), or number of patients with GBL (%).
c Value for entire study population while only 1 cohort was included in our analysis.
d Banana glenoid described by authors as a glenoid so eroded that it assumes the shape of a banana.
Surgical Technique
In accordance with our inclusion criteria, all studies described the technique used to manage the joint capsule. Eight studies that employed an intra-articular bone block position described repair of the joint capsule to the remnant CAL stump (Figure 2). 2,5,28,30,32,33,38,48 Among these, 2 studies specified the capsular repair being performed with the arm in external rotation, 32,33 and 1 study mentioned the capsule being repaired without inducing retightening. 5 There was minor variation among these studies in the management of the subscapularis. The authors of 6 studies employed a horizontal split between the upper two-thirds and lower one-third of the subscapularis. 2,28,32,33,38,48 Kee et al 28 described repairing the subscapular split, while Beranger et al 2 mentioned its not being repaired. The remaining 4 studies did not report whether or not the subscapularis split had been repaired. 32,33,38,48 Marion et al 30 reported the subscapularis tendon’s being closed via 1 X-suture but did not describe the method by which it was incised. Bonnevialle et al 5 employed an L-shaped tenotomy that was subsequently sutured in the anatomic position using separate stitches and nonabsorbable braided sutures.

Illustration demonstrating the intra-articular bone block technique with the medial capsule sutured to the remnant coracoacromial ligament stump of the bone graft. (Reprinted with permission from Mizuno N, Denard PJ, Raiss P, Melis B, Walch G. Long-term results of the Latarjet procedure for anterior instability of the shoulder. J Shoulder Elbow Surg. 2014;23(11):1691-1699. 32 )
Eight studies described an extra-articular bone block technique. 1,4,7,8,16,31,46,47 In 7 of these studies, this was achieved using 1 to 3 suture anchors to secure the capsule to the anterior rim of the native glenoid (Table 3). 1,4,8,16,31,46,47 In contrast, Bouju et al 7 described a method in which three 1.5-mm holes were drilled on the lateral side of the bone block to form 2 transosseous U-suture formations for capsular repair (Figure 3). The approach was arthroscopic in 4 studies, 1,4,31,46 open in 3 studies, 7,8,16 and a comparison of arthroscopic versus open surgery in 1 study. 46 The method by which the subscapularis, labrum, and capsule were managed in each study, as well as details regarding bone block fixation, are outlined in Table 3.
Surgical Technique a

a Arthrosc, arthroscopic; CAL, coracoacromial ligament; ER, external rotation; IGHL, inferior glenohumeral ligament; NR, not reported; SLAP, superior labrum anterior to posterior.
b In patients who had hyperlaxity, the split was made at the junction of upper and lower halves to maximize the sling effect.

(A) Bone block preparation showing (B) 2 transosseous U-suture formations for capsular fixation. Unlike other capsular-coracoid repair techniques, (C) the method employed by Bouju et al 7 yields (D) an extra-articular bone block. The dotted line refers to the articular surface of the glenoid. (Reprinted with permission from Bouju Y, Gadea F, Stanovici J, Moubarak H, Favard L. Shoulder stabilization by modified Latarjet-Patte procedure: results at a minimum 10 years’ follow-up, and role in the prevention of osteoarthritis. Orthop Traumatol Surg Res. 2014;100(4)(suppl):S213-218. 7 )
Rehabilitation
Fifteen studies described their respective rehabilitation protocols. †† In 11 studies, a 1- to 6-week period of immobilization with a sling was reported. ‡‡ In 4 studies, passive range of motion exercises were permitted in the immediate postoperative period. 1,2,4,30 Figure 4 provides a visual representation of the progression of rehabilitation among the studies in which it was reported.
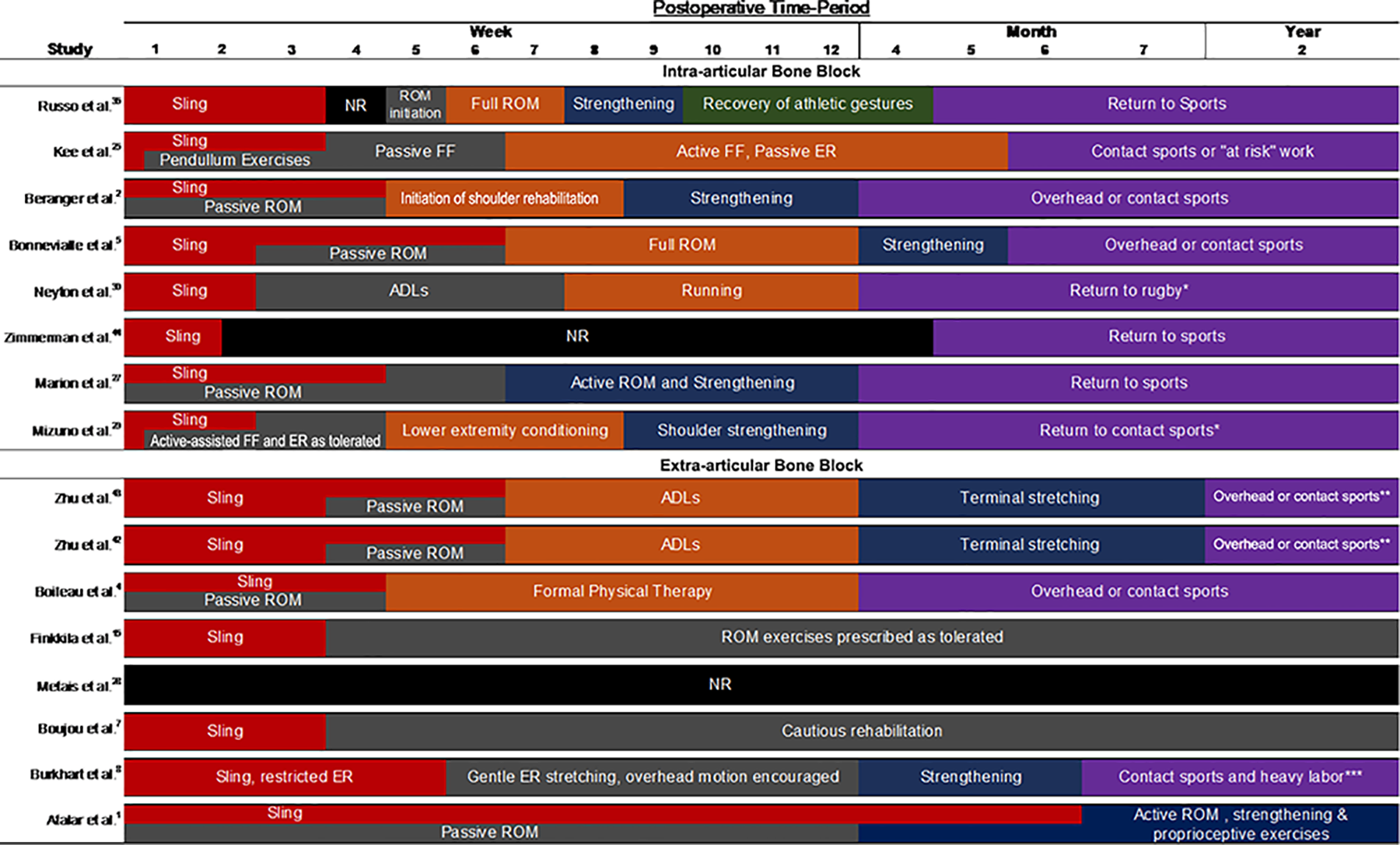
Postoperative rehabilitation. *After clinical and radiographic evaluation showed satisfactory healing of the coracoid graft. **When full ROM was restored and no apprehension detected. ***Delayed until 1 year postoperatively if bone graft did not show radiographic consolidation at 6 months. ADL, activities of daily living; ER, external rotation; FF, forward flexion; NR, not reported; ROM, range of motion.
Functional Outcomes
Intra-articular Bone Blocks
Five of the 8 studies that employed an intra-articular bone block technique reported postoperative Rowe scores (Table 4). 5,28,32,33,38 Among these, preoperative Rowe scores were reported in 3 studies, all of which demonstrated significant improvements at final follow-up. 28,32,38 The only intra-articular bone block study that reported Constant-Murley scores found a significant improvement from preoperative values at final follow-up. 38 Other functional outcome scores reported among the intra-articular bone block studies included Walch-Duplay scores in 2 studies 5,33 and University of California Los Angeles scores in 1 study. 28
Functional Outcome Scores a

a Data reported as mean ± SD (range). Values in bold represent statistically significant difference between groups (P < .05). A, arthroscopic; C, collision; NC, noncollision; NR, not reported; O, open; postop, postoperatively; preop, preoperatively; UCLA, University of California Los Angeles.
b Mean (95% CI).
Extra-articular Bone Blocks
Five of the 8 studies that employed an extra-articular bone block technique reported postoperative Rowe scores. 1,4,31,46,47 Among these, preoperative Rowe scores were reported in 3 studies, all of which demonstrated significant improvements at final follow-up. 1,46,47 Three extra-articular bone block studies reported Constant-Murley Scores. 8,46,47 Among these, 2 studies included preoperative values, 46,47 and both reported no significant improvements from preoperative scores in patients who underwent arthroscopic Latarjet. However, mean preoperative Constant-Murley scores in these studies were 91.5 in 1 study 47 and 93.1 in the other. 46 Other functional outcome scores reported among the intra-articular bone block studies included Walch-Duplay scores in 4 studies. 4,7,8,31
Recurrent Instability
Intra-articular Bone Blocks
Among the intra-articular bone block studies, 6 reported the incidence of recurrent dislocations 2,5,28,32,33,48 and 5 reported recurrent subluxations, 5,28,32,33,48 with rates ranging from 0% to 2.8% and 0% to 3.6%, respectively. Three intra-articular bone block studies performed the apprehension test clinically. 5,33,48 In these studies, a positive test was elicited in 2 of 6 patients (33.3%), 5 5 of 34 patients (14.7%), 33 and 10 of 93 patients (10.8%). 48 Beranger et al 2 noted that the mean patient-reported level of apprehension quantified on a numerical scale from 0 (none) to 10 (extreme) was 1.7 at final follow-up.
Extra-articular Bone Blocks
Among the 8 extra-articular bone block studies, 7 reported the incidence of recurrent dislocations. 1,4,7,8,16,46,47 Of these 7 studies, 3 reported no postoperative dislocation episodes, 1,46,47 and 3 reported 1 patient with recurrent dislocation (range, 1.4%-1.9%). 4,7,16 Burkhart et al 8 reported that 4 of 102 patients (3.9%) had a recurrent dislocation in the early postoperative period, 1 of which was due to a grand mal seizure and 3 of which were due to premature return to high-risk activity against medical advice. Recurrent subluxation was reported in 0% of patients among 4 studies 7,8,46,47 and 6 of 52 patients (11.5%) in 1 study. 16 Clinical assessment of persistent apprehension was performed in 5 studies. 4,8,31,46,47 A positive result was reported in 0% of patients in 2 studies, 46,47 while Boileau et al 4 found that 13 of 70 patients (18.6%) had persistent apprehension. The remaining 2 studies reported persistent apprehension in 2.1% 8 and 31.6%, 31 but these studies had low clinical follow-up rates of 46% and 30%, respectively (Table 5).
Recurrent Instability a
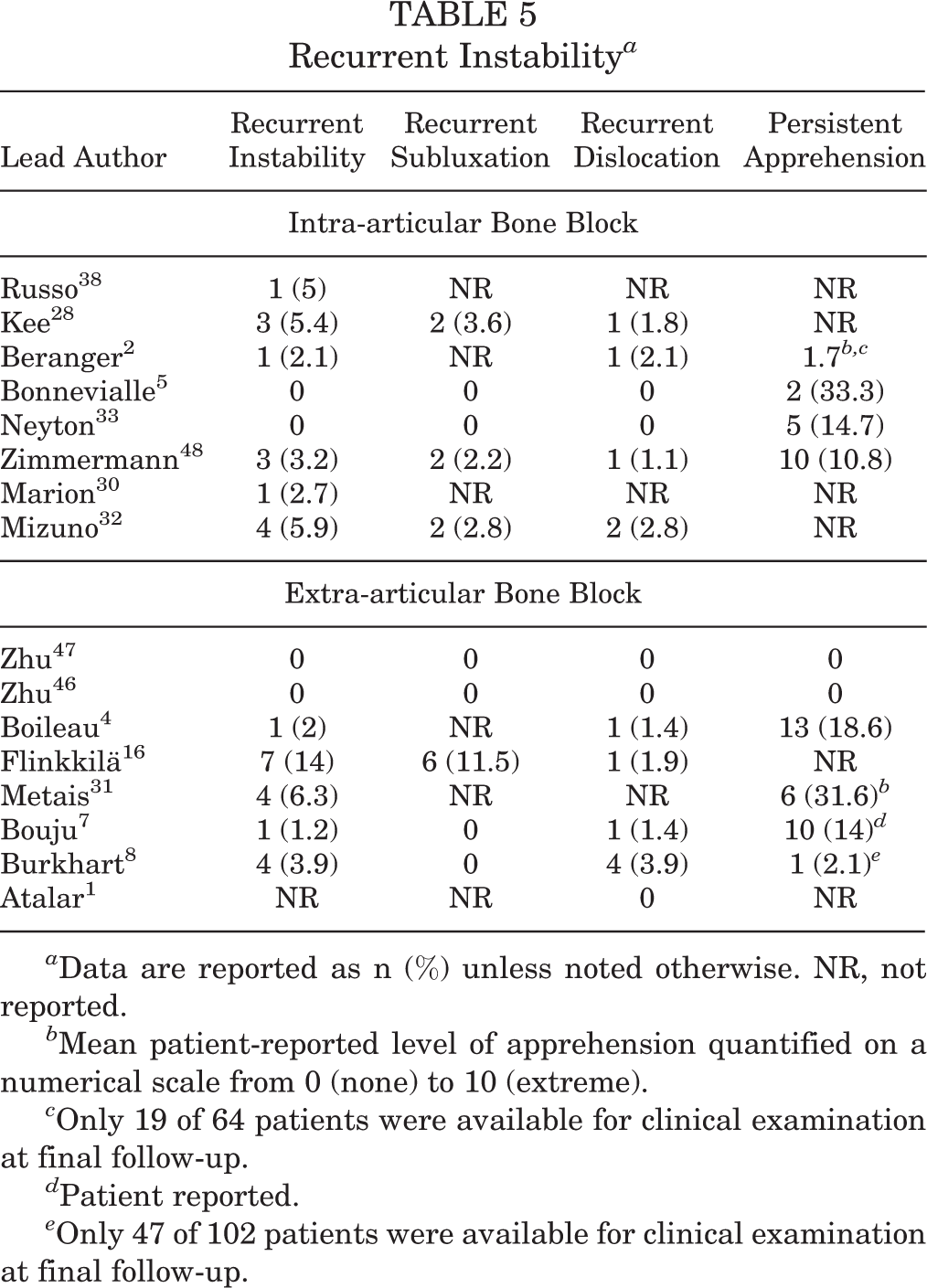
a Data are reported as n (%) unless noted otherwise. NR, not reported.
b Mean patient-reported level of apprehension quantified on a numerical scale from 0 (none) to 10 (extreme).
c Only 19 of 64 patients were available for clinical examination at final follow-up.
d Patient reported.
e Only 47 of 102 patients were available for clinical examination at final follow-up.
Range of Motion
Intra-articular Bone Blocks
Among the 8 intra-articular bone block studies, only 1 study reported preoperative and postoperative range of motion values. 5 In this study, mean external rotation decreased from 76.7° to 54.2° at 0° of abduction and 99.2° to 74.2° at 90° of abduction after a mean follow-up period of 40 months (range, 24-65 months). It is important to note, however, that data from this study represented 6 patients who underwent Latarjet after failed SCR. Russo et al 38 reported that limited external rotation was found in 12 of 20 patients (60%), with a mean loss of 9° with the arm in a neutral position and 5° at 90° of abduction after a mean postoperative period of 21 months (range, 20-39 months). However, mean preoperative and postoperative range of motion values of the entire cohort were not reported. Kee et al 28 reported that the mean external rotation after a mean 67-month follow-up was 47° and that the average discrepancy from the contralateral shoulder was 4.5°. However, preoperative range of motion values were not reported in this study. The reported range of motion values for internal rotation and forward flexion among these studies are detailed in Table 6.
Range of Motion a

a NR, not reported; Postop, postoperative; Preop, preoperative.
b Among 12 of the 20 patients in whom limited external rotation was noted.
c Measured as discrepancy from contralateral shoulder.
Extra-articular Bone Blocks
Among the 8 extra-articular bone block studies, 4 reported preoperative and postoperative range of motion values. 8,31,46,47 Zhu et al 47 reported mean external rotation decreasing from 54.6° preoperatively to 52.4° after a mean 28.4-month follow-up (range, 24.0-41.7 months). In the study by Zhu et al, 46 mean losses of 4.5° and 6.3° of external rotation were observed in the open and arthroscopic groups, respectively, after a mean postoperative period of 37.1 months (range, 24.2-62.3 months). Metais et al 31 found that mean external rotation decreased from 70.4° to 61.1° at 0° of abduction and 90.0° to 88.9° at 90° of abduction after a mean 22.7-month follow-up (range, 13-32 months). Burkhart et al 8 reported a mean 5.1° loss in external rotation at 59-month follow-up (range, 32-108 months), with reported values decreasing from a mean of 55.3° preoperatively to 50.2° postoperatively. Boileau et al 4 reported that after a mean 35-month follow-up (range, 24-60 months), the mean external rotation was 57° (range, 20°-90°), and a 9° discrepancy in external rotation from the contralateral shoulder was noted. However, the authors of this study did not report preoperative range of motion values. Atalar et al 1 reported that mean external rotation was 59° at 24-month follow-up (range, 12-74 months) but did not provide preoperative values. Interestingly, among the extra-articular bone bock studies, a mean overall gain in forward flexion was reported in cohorts in which an open technique was employed, 8,46 while a mean overall loss in forward flexion was found in those with an arthroscopic technique. 31,46,47 In 1 study comparing open and arthroscopic techniques utilizing the same method for capsular repair, mean forward flexion increased by 10° in the open group and decreased by 2.6° in the arthroscopic group. 46
Radiologic Outcomes
Intra-articular Bone Blocks
Six of the 8 intra-articular bone block studies reported radiologic outcomes. 5,28,30,32,33,38 The postoperative graft position on the horizontal plane was reported in 5 studies. 5,28,30,32,33 Among these, the bone block was found to be flush with the glenoid articular surface in 12.5% to 100% of cases, too lateral in 0% to 13%, and too medial in 0% to 87.5%. Russo et al 38 did not report the horizontal bone block position. Among the 3 studies reporting vertical bone block position, it was found appropriately placed in 50%, 30 89%, 33 and 100% 5 of cases. Three studies did not report the vertical bone block position. 28,32,38
Five intra-articular bone block studies reported the incidence of glenohumeral osteoarthritis. 5,28,32,33,38 Russo et al 38 reported that 5 of 20 patients (25%) had grade 1 or 2 osteoarthritis after a mean 21-month follow-up (range, 20-39 months). Kee et al 28 reported that at minimum 12-month follow-up, 3 of 56 patients (5.4%) had progression of preoperative osteoarthritis or previously unidentified arthritic changes. Neyton et al 33 reported postoperative osteoarthritis or progression of preoperative osteoarthritis in 8 of 37 shoulders (21.6%) at 144-month mean follow-up (range, 68-237 months). After a mean follow-up period of 20 years (range, 18-22 years), Mizuno et al 32 reported postoperative osteoarthritis or progression of preoperative osteoarthritis in 16 of 68 patients (23.5%).
Extra-articular Bone Blocks
Five of the 8 extra-articular bone block studies reported radiologic outcomes. 1,4,7,46,47 The postoperative graft position on the horizontal plane was reported in 4 studies. 4,7,46,47 Among these, the bone block was found to be flush with the glenoid articular surface in 100% of cases at 1-year follow-up in 2 studies. 46,47 Boileau et al 4 found that the coracoid graft was flush in 92.9% of shoulders, too medial in 2.9%, and too lateral in 4.3% of cases. Bouju et al 7 reported lateral overhang of the bone block in 7 of 58 shoulders (12.1%). Among the 4 studies that reported vertical bone block position, it was found appropriately placed in 78.8% to 98.3% of cases. 4,7,46,47 Interestingly, in the study by Zhu et al 46 comparing arthroscopic and open Latarjet techniques, a significantly increased rate of vertically correct graft placement was found in the open (100%) versus arthroscopic (91.3%) groups (P < .001).
Four extra-articular bone block studies reported the incidence of osteoarthritis. 1,4,7,47 The follow-up period was short in the study by Atalar et al, 1 which reported no radiographic evidence in any patients at mean 8-month follow-up. Zhu et al 47 reported 1 case (1.9%) of rapidly progressing osteoarthritis on 1-year computed tomography scan. Boileau et al 4 reported 6 cases (9%) of Samilson grade 1 (5 cases) or grade 2 (1 case) osteoarthritis at mean 35-month follow-up. Lastly, Bouju et al 7 reported 3 cases (5.2%) of Samilson grade 1 osteoarthritis after a mean follow-up of 13 years. Table 7 outlines the radiologic outcomes reported among included studies.
Radiologic Outcomes a

a Data are reported as n (%) or n (range), the value for Bouju study is mean ± standard deviation. CT, computed tomography; NR, not reported; XR, radiograph.
b Postoperative osteoarthritis or progression of preoperative osteoarthritis.
c Only patients who had complete follow-up were included.
d At final follow-up. All patients had CT scans immediately after surgery. Thus, “bone block position” results were available for all 90 patients.
e Rate of vertically correct graft placement was found in the open (100%) versus arthroscopic (91.3%) groups (P < .001).
f Arthroscopic group showed significantly less bone resorption than open group (P = .044).
g 100% follow-up or study only included patients who were available for follow-up.
Discussion
The principle finding of this review on the Latarjet procedure is that capsular repair methods that yield an extra-articular coracoid graft are associated with a decreased risk of postoperative osteoarthritis. However, in the current literature, there are no studies comparing Latarjet outcomes with intra-articular versus extra-articular graft positions while controlling for other variables. Thus, this observation is based on comparison of heterogeneous studies. In addition, heterogeneity among studies precluded our ability to draw strong conclusions regarding our other outcomes of interest, including the effect of amount of preoperative bone loss, the medial-lateral position of the coracoid bone on the glenoid neck, and the comparison of preoperative and postoperative external rotation. These factors may also contribute to the risk of developing posttraumatic arthritis.
The Latarjet procedure is a well-studied treatment modality for patients who have anterior shoulder instability with critical glenoid bone loss. While it has been shown to result in good outcomes for most patients, it carries a risk of potential complications including recurrent instability, loss of range of motion, neurologic injury, and postoperative osteoarthritis. Some studies have suggested that the risk of these complications may be influenced by the capsular repair technique employed after coracoid graft fixation. 27,29 However, surgeons are left to make this decision based on laboratory data and low level of evidence clinical studies. 7,27 The results of our review further implicate the method of capsular repair as a potential risk factor, but the reader is cautioned that our observations were based on a group of heterogeneous level 3 and 4 studies that happened to report this component of their surgical technique and were not specifically designed to assess differences in these techniques.
The rate of osteoarthritis after Latarjet is estimated to be 42% at 5-year follow-up. 37 Repairing the capsule in a manner that results in an extra-articular bone block may decrease this risk. Two distinct methods of achieving an extra-articular bone block were employed in the studies included in our review: (1) suture anchor fixation of the capsule to the native glenoid rim and (2) transosseous suture fixation to the coracoid bone block at the edge of the glenoid cavity. Bouju et al 7 employed the latter variant of capsular repair in 78 shoulders and reported an overall osteoarthritis rate of 8.6% after a mean 13-year follow-up. Among the 5 shoulders that demonstrated radiographic evidence of osteoarthritis at final follow-up, 2 had preoperative arthritic changes that remained stable after Latarjet. Thus, the incidence of postoperative osteoarthritis or progression of preoperative osteoarthritis was 5.2% at 13-year follow-up. Capsular fixation to the native glenoid rim was performed in all remaining extra-articular bone block studies. 1,4,8,16,31,46,47 Among the other 4 that reported the incidence of osteoarthritis, 1,4,46,47 the follow-up time was no longer than 1 year in 3 studies. 1,46,47 Boileau et al 4 employed this variant of capsular repair in 70 shoulders and reported a 9% rate of osteoarthritis after 33-month mean follow-up. The suture anchor capsular repair to the glenoid offers the advantage of minimal tension on the coracoid bone graft during external rotation and a structurally stronger fragment by minimizing drill holes in a small coracoid graft. However, there was no statistically significant difference in graft nonunion or fracture between the 2 described techniques.
Due to the differences among studies included in our review, quantifying the results by way of meta-analysis was not appropriate. However, there appeared to be a trend toward higher rates of osteoarthritis for shoulders in which a capsular-CAL repair technique left the bone block in an intra-articular position. Russo et al 38 reported that 25% of patients had signs of articular cartilage alteration a 21-month mean follow-up. However, it was specified that that these lesions involved the glenoid surfaces without mention of the humeral head articular cartilage. This obviates the possibility that humeral head to coracoid graft contact led to cartilage degeneration in these patients. After a mean 40-month follow-up, Bonnevialle et al 5 reported that all 6 patients in this very small-scale study were free of osteoarthritis, while Mizuno et al 32 reported a 23.5% rate of glenohumeral osteoarthritis after a mean 20-year follow-up. Similarly, Neyton et al 33 reported the incidence of glenohumeral osteoarthritis exceeding 20% after a mean 12-year follow-up. While these rates are higher than those in any studies in which an extra-articular bone block technique was employed, heterogeneity among our reviewed studies makes it difficult to implicate capsular repair position as the sole culpable risk factor for osteoarthritis.
Risk factors for postoperative osteoarthritis after Latarjet include both patient-specific factors such as older age at the onset of shoulder instability, preoperative fracture of the anterior glenoid rim, and participation in high-demand sport activities, as well as technical factors, including a laterally overhanging bone block or excessive screw obliquity. 3,9,13,19,45,47 In the 2 intra-articular bone block studies with the longest follow-up times and the highest reported rates of osteoarthritis, glenoid rim fractures were identified in 48.6% 33 and 35.3% 32 of patients preoperatively. Nevertheless, the landmark study by Bouju et al 7 reported glenoid fractures in 44% of patients and observed low long-term rates of osteoarthritis that were attributed to the capsular repair position. Two intra-articular bone block studies evaluated lateral overhang of the coracoid graft as a risk factor for postoperative osteoarthritis. 28,32 In 1 study, 4 of 56 grafts (7%) were projecting laterally on postoperative images. Among these patients, no differences were reported in the rate of osteoarthritis preoperatively and at final follow-up, 28 but this result is highly prone to type 2 error. Mizuno et al 32 found that 9 of 68 grafts (13.2%) were projecting laterally, a finding they reported to be a significant risk factor for osteoarthritis at final follow-up. Bouju et al reported a similar rate of laterally projecting bone blocks (7 of 58; 12.1%) and observed no significant association of this finding with the occurrence of osteoarthritis. These results may indicate that positioning the graft so that it is flush with the glenoid articular surface is especially important in the setting of capsular-CAL repairs and, perhaps, that repairing the capsule to the native glenoid may be protective in the setting of laterally projecting grafts. Finally, biomechanical studies have demonstrated that both the congruent arc of the bone block and its flush position in the correct inferior location can all increase contact pressure in the glenohumeral joint. 14,17
Another important implication of capsular repair position is postoperative range of motion. When the capsule is repaired to the CAL, depending on the amount of bone loss, the length of the capsule-CAL repair may be elongated by the thickness of the bone block. However, repairing the capsule directly to the native glenoid when there is bone loss will definitely reduce the arc of motion from the preinjury status. If the extra-articular capsular repair tissue remains intact, it is likely to reduce external rotation as demonstrated by Itoigawa et al 27 in a biomechanical comparison of the 2 capsular repair positions. However, rather than suturing the capsule to the CAL for the intra-articular bone block position, a transosseous suture technique was employed to repair the capsule directly to the coracoid graft. Capsular repair to the glenoid rim was found to restrict external rotation to a significantly greater degree compared with capsular-CAL repair, but it also provided significantly greater stability with the arm in neutral rotation. Based on their investigation, the authors recommended repairing the capsule to the coracoid to preserve range of motion in external rotation. As mentioned previously, it is uncertain if there is an increased risk of graft nonunion or fracture when this technique is employed clinically.
Translating these findings to the clinical setting was difficult based on the studies included in this review. Postoperative range of motion values were only reported in 3 of the 8 intra-articular bone block studies, 5,28,38 compared with 6 of 8 extra-articular bone block studies. 1,4,8,31,46,47 In contrast to the findings of Itoigawa et al, 27 the largest observed loss in external rotation (mean, 22.5°) was reported after capsular-CAL repair in the study by Bonnevialle et al. 5 However, these results were the average of only 6 patients who had a history of SCR, 2 of whom had external rotation deficits of 30° and 40° compared with preoperative values. Bonnevialle et al attributed these large limitations to subscapularis tendon fibrosis after repeat tenotomy and prolonged protection against external rotation during the rehabilitation period. It may be important to note this is 1 of 3 studies that employed an L-shaped subscapularis tenotomy technique compared with the horizontal subscapularis split used in all other studies. 1,5,8 Interestingly, the lowest reported postoperative range of external rotation (47°) was in a study that employed a capsular-CAL repair technique. 28 Among studies that reported postoperative range of motion values, this was the only study that also reported repair of the subscapularis split. Due to heterogeneity in surgical technique beyond the method of capsular repair among studies that reported postoperative range of motion, the findings by Itoigawa et al could neither be corroborated nor refuted by the current review.
A recent systematic review and meta-analysis performed by Hurley et al 25 compared the outcomes of open versus arthroscopic Latarjet procedures. Those authors reported no significant differences between approaches in outcome measures, recurrent instability, postoperative external rotation, or complications. However, it was found that the rate of persistent apprehension was significantly higher with the arthroscopic Latarjet procedure (35.7%) compared with the open technique (10.2%; P < .01). This finding gives merit to our decision to forgo a meta-analysis comparing capsular repair techniques. The extra-articular bone block cohorts in our review comprised both open and arthroscopic techniques, while all the intra-articular bone block studies utilized an open approach. Among the extra-articular bone block studies in our review, a mean overall gain in forward flexion was reported in cohorts in which an open technique was employed, 8,46 while a mean overall loss in forward flexion was found in those with an arthroscopic technique. 31,46,47 In 1 study comparing open and arthroscopic techniques utilizing the same method for capsular repair, mean forward flexion increased by 10° in the open group and decreased by 2.6° in the arthroscopic group. 46 Forward flexion was not evaluated in the study by Hurley et al, precluding our ability to confirm our observation that arthroscopic Latarjet may lead to decreased forward flexion compared with its open counterpart. While the mechanism for this finding is not clearly understood, it may be due to the position of the subscapularis split in open versus arthroscopic approaches.
The influence of capsular repair position on the occurrence of postoperative instability or persistent apprehension could not be assessed by evaluating the studies included in this review. The rates of these complications varied widely among studies that employed each capsular repair technique, with no apparent trend differentiating intra-articular and extra-articular bone block techniques. Proper healing of the coracoid graft to the glenoid neck has been shown to be a risk factor for persistent apprehension in patients who undergo the Latarjet procedure. 10,22,24,42 Due to inconsistency among studies in reporting the rates of graft healing, as well as those of postoperative instability, this association could not be analyzed adequately by this review. Boileau et al 4 reported a relatively low rate of bone block healing (73%) and one of the highest rates of persistent apprehension (18.6%). In the study by Bouju et al, 7 14% of patients reported persistent apprehension postoperatively. The authors reported that this finding correlated with the presence of preoperative hyperlaxity (P = .049). It has been shown that reducing the joint volume by performing a horizontal capsular shift at the time of Latarjet in patients who have increased shoulder laxity could effectively improve subjective stability. 23 Repairing the capsule to the native glenoid may function in a similar manner to a horizontal capsular shift. However, the heterogeneity among studies reporting preoperative hyperlaxity precluded our ability to determine its effect on postoperative stability.
This review has several strengths. To our knowledge, it is the first attempt to compare capsular repair techniques among studies reporting outcomes of the Latarjet procedure. Due to the multitude of factors besides capsular repair position that could influence our outcomes of interest, we extracted a plethora of preoperative data to aid the reader in appropriately evaluating the included studies. To capture all studies that met our criteria and ensure accurate data mining, 2 independent reviewers conducted the literature search and extracted data.
Limitations
This review also has its limitations. Our outcomes of interest could be influenced by several factors other than capsular repair position. This precluded our ability to determine whether the postoperative outcomes we collected demonstrated a causal relationship of capsular repair technique and the incidence of posttraumatic arthritis. While our study does provide evidence of a relationship between extra-articular capsular repair and a decreased incidence of posttraumatic arthritis, we cannot determine the effect of other known risk factors such as patient-specific differences (ie, amount of glenoid bone loss, existing glenohumeral arthritis, preoperative dislocations, etc) or variations in other aspects of the surgical technique. For this review, we did not include comparison of coracoid fixation position regarding the congruent arc technique for coracoid rotation during fixation. In addition, meta-analysis was not conducted because of heterogeneity among our included studies. The follow-up times were substantially different among our included studies. When evaluating osteoarthritis as a postoperative outcome, long-term follow-up is essential, and similar follow-up times between groups of comparison are necessary to draw reliable conclusions. Last, we only included studies in which the method of capsular management was explicitly stated. Thus, it is probable that some of the studies we excluded from review employed one method or the other without reporting it, thereby introducing selection bias to our review.
Conclusion
This review exposed a gap in the current literature regarding an important surgical variable in the Latarjet procedure, namely, the position of the coracoid bone block in relation to the capsule. High-quality clinical evidence indicating the optimal capsular repair position does not exist. Securing the capsule to the native glenoid rim resulting in an extra-articular coracoid graft may be associated with a lower risk of postoperative osteoarthritis, but this observation was based on comparison of heterogeneous studies. On the basis of our review, we encourage future researchers evaluating the Latarjet procedure to (1) describe with detail the method used to manage the subscapularis tendon, labrum, coracoid position, and joint capsule; (2) adequately report preoperative details including hyperlaxity, glenoid morphology, range of motion, and radiographic evidence of osteoarthritis; and (3) report pertinent postoperative data including recurrent instability, range of motion, radiographic coracoid position, and osteoarthritis at long-term follow-up. A large-scale randomized controlled trial or further comparative studies comparing the 2 techniques are required to draw stronger conclusions.
Footnotes
Final revision submitted August 17, 2021; accepted September 20, 2021
One or more of the authors has declared the following potential conflict of interest or source of funding: K.C.D. has received education payments from Gemini Mountain. M.T.P. has received research support from Arthrex, consulting fees from Arthrex and JRF (Allosource), nonconsulting fees from Arthrex and Flexion, and royalties from Arthrex and Arthrosurface. A.A.R. has received research support, consulting fees, nonconsulting fees, and royalties from Arthrex. K.B.F. has received education payments from Liberty Surgical, consulting fees from DePuy/Medical Device Business Services and Vericel, and nonconsulting fees from Aastrom Biosciences and Vericel. R.M.F. has received research support from Arthrex, education payments from Gemini Mountain and Smith & Nephew, consulting fees from Arthrex and JRF (Allosource), and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.