
Abstract
Background:
With a hip abductor tendon tear, widening of the intergluteal space, or “fat stripe,” is a characteristic change seen in and around the gluteus medius and minimus.
Purpose:
To determine the relationship of the intergluteal fat stripe in hips with pathologic abductor tears compared with the contralateral side and to evaluate the association of fat stripe size with hip-specific patient-reported outcome measures.
Study Design:
Case series; Level of evidence, 4.
Methods:
Of the 43 patients (42 female, 1 male; mean age, 56.6 years; range, 38-85 years) who underwent endoscopic gluteus medius repair, 19 met inclusion criteria of preoperative bilateral hip magnetic resonance imaging (MRI) scans and 2-year follow up. A single board-certified fellowship-trained orthopaedic surgeon (J.F.), who was blinded to outcomes, evaluated the MRI scans to measure the intergluteal fat stripe on the operative and nonoperative sides. The 2-year postoperative International Hip Outcome Tool (iHOT-12) and modified Harris Hip Score (mHHS) values were analyzed to determine their relationship to the size of the fat stripe. Statistical analysis was performed using a paired t test, and associations were determined using Pearson product correlation as well as nonparametric measurements.
Results:
The size of the intergluteal fat stripe differed significantly between the operative and nonoperative sides. The area of the fat stripe on the operative side was 645.73 ± 513.09 mm2, and on the nonoperative side it was 313.47 ± 360.71 mm2, an average of 332.36 mm2 greater than the nonoperative side (P = .02). The width of the fat stripe was 9.10 ± 4.60 mm on the operative side and 5.15 ± 3.87 mm on the nonoperative side, 3.95 mm greater than the nonoperative side (P < .01). There was no correlation between the width or area of the fat stripe on the operative side and iHOT-12 or mHHS values at 2-year follow-up.
Conclusion:
The study findings indicated that the intergluteal fat stripe is significantly wider and has a significantly larger area in hips with abductor tears compared with unaffected hips. This did not correlate with 2-year patient-reported outcomes.
Initially recognized and described by Bunker et al 5 in 1997 while treating femoral neck fractures, hip abductor tendon tears have become increasingly recognized as a source of pain and disability. Since being coined “rotator cuff tears of the hip,” 5 this terminology has been used throughout the literature because of its clinical and morphological similarities to the shoulder pathology of the same name. Although the true prevalence is unknown, Howell et al 12 noticed chronic abductor tendon tears in 20% of patients undergoing total hip arthroplasty.
The true mechanism of injury for tears of the abductor tendons of the hip is unknown. In addition, the pain associated with abductor tendon tears does not always manifest the same, and because of this, the term “greater trochanteric pain syndrome” has been used to describe these vague symptoms and envelop a wide range of diagnoses in this anatomic region. 20 Many times, this pain is referred to as “trochanteric bursitis” because of its location and corresponding symptoms. Initial management usually involves a corticosteroid injection in and around the trochanteric bursa in order to distinguish simple bursitis from a true structural abnormality. 10 When pain does not resolve completely after injection, more advanced modalities are utilized to help identify an underlying cause.
Magnetic resonance imaging (MRI) has been shown to be the preferred diagnostic modality in identifying peritrochanteric pathology such as gluteal tendon tears, with a sensitivity and specificity of 73% and 95%, respectively. 7 The insertion of the gluteus medius tendon onto the greater trochanter has been studied extensively, and its footprint has been specifically mapped out. 18 As our knowledge of this pathology has increased, so has the evolution of endoscopic repair. Initially used to treat only partial-thickness and full-thickness tears without retraction, endoscopic management has advanced to treating a wide array of gluteal tendon tears, including those that are retracted. 16 The ability to preoperatively identify patients who may benefit from early endoscopic intervention could help decrease the delay in operative management that is very common among this population. 1 In addition, identification of patients who may not do as well with endoscopic intervention could help guide preoperative counseling as it pertains to prognosis and patient expectations.
Much like the rotator cuff of the shoulder, the hip abductor tendons and their associated muscle bellies display characteristic signal changes when torn. 7 Widening of the intergluteal space, or “fat stripe,” is a characteristic change seen in and around the muscle of the gluteus medius and minimus in the setting of a hip abductor tendon tear. The exact cause of the increased fat stripe in the intergluteal space is not known, but it is our opinion that this characteristic finding is related to 2 factors. One factor is that chronic tendon tears lead to muscle atrophy; as the muscle bellies decrease in size, fat occupies the space. In addition, as the tendon retracts, the normal tension of the muscle fibers is altered. This alteration may displace the muscle belly from its native anatomic position, creating a void in the intergluteal space.
The purpose of this study was to determine the relationship of the intergluteal fat stripe in hips with pathologic abductor tears compared with the contralateral side. In addition, we evaluated the association of the fat stripe area and width with hip-specific patient-reported outcome measures.
Methods
We retrospectively reviewed the records of 43 consecutive patients (42 female, 1 male) who underwent endoscopic repair of torn abductor tendons from the insertion on the greater trochanter between August 2011 and December 2012. Patients were included in this study if they had a documented preoperative bilateral coronal pelvic MRI, had at least 2 years of follow-up, and were able to be contacted for outcome measures. Of the initial 43 patients, 19 (all female) met the inclusion criteria and were included in this study. These patients had an average age of 56.6 years (range, 38-85 years), and all had undergone surgical repair after failure of nonoperative treatment, 15 for a partial tear of the gluteus medius and 4 for a full tear (Table 1).
Patient Characteristics (N = 19) a
a Data are presented as No. of patients unless otherwise indicated.
The nonoperative treatment consisted of up to 3 trochanteric corticosteroid injections coupled with 12 weeks of physical therapy focused on abductor strengthening. Most patients were reevaluated 4 to 6 weeks after initiation of this regimen. If pain had not improved by that time, advanced imaging was obtained. Continued pain in the trochanteric region, pain and weakness with abduction, and a Trendelenburg gait were used as clinical indications for operative treatment. Advanced imaging consistent with a high-grade partial- or full-thickness gluteal tear on MRI that correlated with physical examination findings and documented failure of conservative nonoperative treatment was used as an indication for surgical treatment.
Surgical Technique
The operative procedure consisted of an intra-articular diagnostic arthroscopic examination as described by Bond et al, 4 with the exception that a midanterolateral portal was used in lieu of a direct anterior portal. After the diagnostic arthroscopy was completed and all intra-articular pathology was identified and corrected, the camera was removed and a spinal needle was used to infiltrate normal saline into the potential space superficial to the iliotibial band. This created a space to insert a 30° arthroscope. The spinal needle was then used under fluoroscopy to locate the footprint of the gluteus medius tendon and was placed gently into the greater trochanter to mark this location. Portals were then established about 4 to 5 cm distal and proximal to the spinal needle, and a 30° arthroscope was inserted in the superior portal. The iliotibial band was visualized and split longitudinally with a cautery device. The peritrochanteric bursa was then excised with a mechanical shaver, and the abductor tendons were visualized.
Partial-thickness and full-thickness tears were repaired with a technique similar to rotator cuff tear of the shoulder, using anchors and nonabsorbable suture through small accessory portals as needed. Partial-thickness tears were repaired by entering underneath the already detached portion of the anterior oblique fibers of the gluteus medius or by taking down and undermining those fibers in order to enter the tear site for bone and soft tissue preparation. Both single- and double-row techniques were utilized, depending on the tear type and quality of the tendon; in this study, 13 single-row and 6 double-row methods were performed.
Postoperatively, patients were placed in an abduction brace for 6 weeks; no active abduction was allowed during that time. The brace allowed 90° of flexion the first 2 weeks and progression as tolerated. Progressive strengthening was initiated after 6 weeks. Physical therapy included flexion to 90° during the first 2 weeks and full extension, with progression as tolerated thereafter. Patients were allowed touch-down weightbearing for 6 weeks, with progression as tolerated.
MRI Review
All MRI scans of the study patients were reviewed by a board-certified orthopaedic surgeon (J.F.), fellowship-trained in sports medicine and hip arthroscopy, who was blinded to the patient-reported outcomes. The intergluteal fat stripe was identified on preoperative coronal MRI T1 imaging, measured, and compared with the contralateral side. Although T2-weighted images were used to specifically identify a gluteal tear, we found that T1-weighted images were better for visualizing the intergluteal fat stripe because of its signal enhancement specific to adipose tissue.
Measurements of the fat stripe were taken at the greatest length and greatest width. Figure 1 is a representative MRI of the fat stripe seen on the operative side of patients undergoing repair. Care was taken to ensure the same coronal plane was selected in each patient by using consistent bony landmarks easily identified on MRI. Each measurement was taken at the level where the greater and lesser trochanters were most prominent. For the comparison measurements, the representative image was taken from the bilateral coronal scans, preferably the T1-weighted images. The image selected was the slice halfway between the first image exhibiting the anterior superior iliac spine and the first image exhibiting the sacroiliac joint. For example, if the anterior superior iliac spine was first seen at slice 5 and the sacroiliac joint was first seen at slice 29, then the measurements were taken at slice 17. The transverse measurement was taken at the midportion of the visible stripe, and the longitudinal measurement was taken from the cranial-most to the caudal-most portion of the visible stripe. The 2 measurements were then multiplied to calculate the area of the fat stripe. Characteristic intergluteal fatty area (fat stripe) seen on the operative side (left hip). Arrow 1 indicates the intergluteal fatty area. Arrow 2 indicates the nonoperative image without the fat stripe.
Outcome Measures
All study patients were contacted and assessed using our routinely collected patient-reported outcomes, the International Hip Outcome Tool (iHOT-12), and the modified Harris Hip Score (mHHS). All assessments took place at least 2 years postoperatively.
Statistical Analysis
To assess intrarater reliability, the imaging data were extracted on 2 occasions more than 1 year apart. A 2-way, mixed-effects, consistent, single-rater measurement intraclass correlation coefficient (ICC[3,1]) was run to measure the consistency of association between the 2 extraction points. Cicchetti 6 proposed the following boundaries for interpretation of ICC values: poor, <0.40; fair, ≥0.40 and ≤0.59; good, ≥0.60 and ≤0.74; and excellent, ≥0.75 and ≤1.00.
Paired t tests were used to analyze differences in both the area and width of the fat stripe between the operative and nonoperative sides. Associations between stripe total area and width and patient-reported outcome measures were analyzed using the Pearson product correlation. Nonparametric analyses were conducted for the nonoperative assessments. All statistical analyses were performed using IBM SPSS Statistics for Windows version 26.0 (IBM Corp). P values <.05 were considered statistically significant.
Results
The ICC(3,1) was statistically significant and yielded a result of 0.98 (95% CI, 0.95-0.99), indicating excellent agreement for the single rater at the 2 given assessment points. A degree of objective tendinopathy with mild- to high-grade tears was seen approximately two-thirds of the time on the contralateral hips. There was a significant difference in the area of the intergluteal fat stripe between the operative and nonoperative sides of the study patients (P = .02), with the operative side tear being 332.36 mm2 larger than that of the nonoperative side (Table 2). Differences were also present when evaluated nonparametrically (P < .01). In addition, the width of the fat stripe, measured at the widest point on the coronal image, was 3.95 mm larger on the operative side than the nonoperative side (P < .01), a value reinforced through use of nonparametric testing (P < .01).
Average Intergluteal Fat Stripe Differences a

a Bolded P values indicate a statistically significant difference between the operative and nonoperative sides (P < .05).
The area of the fat stripe was not significantly associated with the mHHS or the iHOT, a finding that was verified using nonparametric measures. The width of the fat stripe was not significantly associated with the mHHS or the iHOT, a finding that was also verified using nonparametric measures (Table 3).
Correlation of Fat Stripe Measurements With Patient Outcomes a
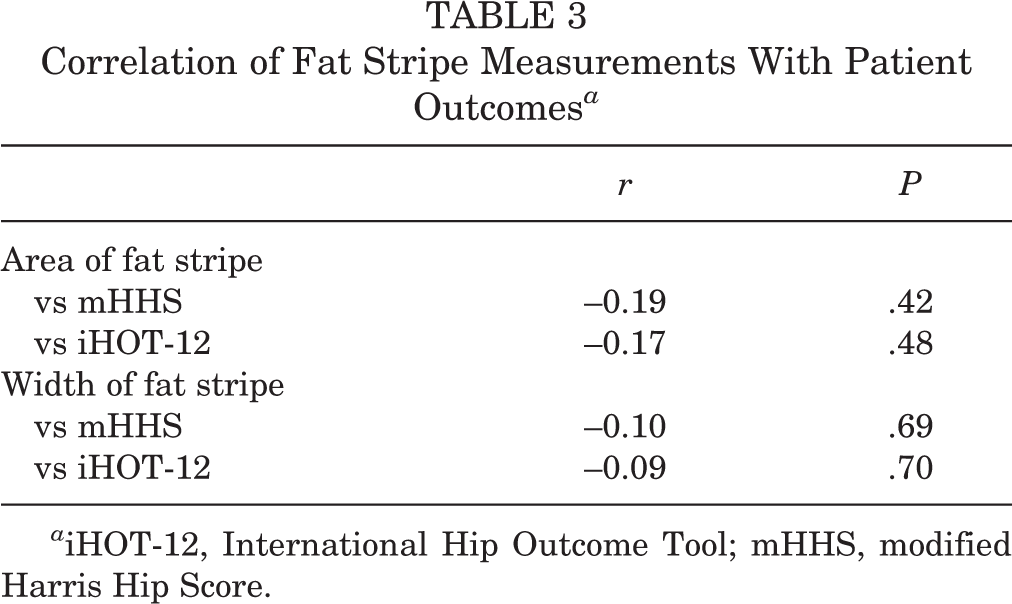
a iHOT-12, International Hip Outcome Tool; mHHS, modified Harris Hip Score.
Discussion
Overall, this study shows a statistically significant difference between the width and area of the fat stripe in the affected hip. Increased fat signal develops in between the gluteus medius and minimus after a chronic tendon tear to develop the characteristic intergluteal fat stripe. Outcomes of rotator cuff pathology in the shoulder are worse with muscle and tendon deterioration over time; these findings may be similar for hip abductor pathology. In 2009, Davies et al 8 reported 16 patients who underwent repair of the gluteus medius tendon. Although 4 patients experienced rerupture and 1 developed a postoperative infection, the remaining 11 patients had significant improvement in the visual analog scale as well as Oxford hip and SF-36 scores.
More recently, endoscopic repair of gluteal tears of the hip has become more common among orthopaedic surgeons. A recent systematic review by Alpaugh et al 2 identified 8 studies with patients undergoing repair and reported an overall retear rate of 9% among patients treated with open repair versus 0% for those treated endoscopically. However, specific evidence-based indications for repair are lacking. 14 Voos et al 21 originally reported outcomes in 10 patients undergoing endoscopic repair of torn abductor tendons. After an average of 25 months of follow-up, he reported complete resolution of pain and 5/5 abduction strength in all 10 patients. Domb et al 9 performed endoscopic repair of chronic abductor tears in 15 patients and followed them for 2 years. He noted statistically significant improvement in mHHS, Non-Arthritic Hip Score (NAHS), Hip Outcome Score–Activities of Daily Living (HOS-ADL), and Hip Outcome Score–Sport-Specific Subscale (HOS-SSS). Fourteen of 15 patients reported satisfaction levels of good to excellent. McCormick et al 16 performed endoscopic repair of both acute and chronic abductor tendon tears in 10 patients and followed them for 1 year postoperatively. He noted significant improvement in hip abductor strength and reported overall satisfaction ratings of good to excellent (defined as mHHS >80) in 6 patients and fair in 4 patients.
MRI has been established as a key diagnostic tool for identifying hip abductor tendon tears. 7 In addition, MRI may offer insight to the specific pathology of the patient’s condition, which would translate to a better understanding of the patient’s prognosis and potential outcome given a specific treatment plan. Sutter et al 19 retrospectively reviewed MRI scans in patients with abductor tendon tears and collected the size ratio of the tensor fascia lata between operative and nonoperative sides. He compared this ratio to MRI scans of patients without abductor tears and found that because of the hypertrophy of the tensor fascia lata muscle on the operative side, there was a significantly greater ratio among patients with abductor tears compared with normal controls.
Marcon et al 15 established normative values of fat content and volume based on MRI for healthy individuals, 20 to 62 years of age. Their work showed neither age dependency for hip abductor muscle volume nor a difference in muscle volume for the dominant versus nondominant hip. These findings further validate the notion that muscle atrophy and loss of volume are attributable to pathology as opposed to the normal aging process. Interestingly, Marcon’s normalized hip values correlated with Goutallier grade 1, no fatty infiltration apart from fatty streaks. According to multiple authors, fatty atrophy of gluteus minimus can be found in both symptomatic and asymptomatic patients, while fatty atrophy of the gluteus medius appears to be more suggestive of true pathology. 11,15,17 Thus, it is logical that if the Goutallier classification is used, it is best to evaluate the gluteus medius musculature as opposed to the gluteus minimus.
Bogunovic et al 3 analyzed hip abductor tears with the Goutallier/Fuchs classification, although they did not evaluate the gluteus medius muscle in isolation. They concluded that the Goutallier/Fuchs classification system can be applied to abductor tendon tears and that increasing preoperative muscle fatty atrophy is associated with worse subjective and objective patient outcomes. The previous studies differ from our study in that they are evaluating the abductor musculature fat content and volume, whereas we are simply identifying the “fat stripe” between the gluteus medius and minimus muscles. Identification of an enlarged fat stripe is an easily identifiable and reliable way to identify chronic tendon tear; this may prove to be less subjective than the Goutallier classification.
Signal changes found on MRI between the gluteal muscles and the relationship to patient outcomes are limited. Kirby et al 13 retrospectively followed 20 patients and found that patients with less fatty infiltration had better outcomes after endoscopic repair. This study establishes a relationship between amount of fatty infiltration and the impact on patient outcomes. This concept parallels the findings of rotator cuff pathology in the shoulder. Increased fatty atrophy of the rotator cuff musculature is associated with decreased outcomes and healing rates. Although we did not see a significant correlation between size of the intergluteal fat stripe and patient-reported outcomes, further investigation is warranted. One explanation for the findings in this paper could be due to the relatively small number of patients in this study, which may have decreased the ability to show a difference in outcomes compared with intergluteal fat stripe size. Nevertheless, previous studies 9,16,21 that have reported decreased outcomes from endoscopic repair of gluteal tendon tears have had similar sample sizes and, in many cases, have less than our current study. Thus, the fat stripe may be a reliable way to easily identify chronic hip abductor tears but may not correlate with clinical outcome.
Limitations
This study has several limitations. First, the study is limited by its retrospective design as well as its small sample size from a single surgeon. In addition to the small sample size, the study was mainly comprised of female patients with only 1 male participant, as this disease is most often seen in middle-aged females. Another limitation of this study, as a result of the small sample size, is that we were unable to perform subgroup analyses. These limitations may affect the generalizability of our findings. Another potential limitation of the study is that we calculated the area of the fat stripe based on a length and width measurement, which assumes a uniform shape of the stripe. There is software available that can give a more precise volumetric and area calculation. However, we believe it is important to note that our method makes these findings more generalizable and clinically useful. With this method, the clinician can simply look at a patient’s MRI scan and compare it to the contralateral side to determine if the fat stripe is larger, as opposed to having to run the imaging through special software to aid in the clinical decision. Although it was not the goal of this study, a potential limitation is that advanced imaging was not performed postoperatively, and thus a tendon repair healing rate cannot be determined from this study. We used outcome measures to determine the “success” of the procedure. Another weakness of the study as it relates to imaging is that we did not require bilateral hip MRI scans but also used pelvic MRI scans. This study included both full-thickness and partial-thickness tendon tears, as well as those fixed with a single-row and double-row technique. A larger study size would strengthen the results of this study. In addition, the patient-reported outcome measures we used to determine outcomes were hip specific, but not designed for hip abductor pathology.
Conclusion
The intergluteal fat stripe is a simple and quick method for evaluating patients with possible gluteal tendon pathology. We found that the fat stripe is larger in hips with abductor tears and can be reliably identified with coronal imaging. Our study did not find a correlation between outcomes and the size of the fat stripe. The fat stripe can be used in combination with the somewhat unreliable Goutallier classification to aid the clinician in determining operative indications and postoperative outcomes.
Footnotes
Final revision submitted September 6, 2021; accepted September 16, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: L.J.H. has received grant support from Arthrex and education payments from Smith & Nephew. C.R.B. has received grant support from Arthrex and DJO, education payments from Arthrex and Smith & Nephew, and hospitality payments from DePuy. J.M.T. has received education payments from Elite Orthopedics, Goode Surgical, and Peerless Surgical; consulting fees from Arthrex, DePuy Mitek, and Zimmer Biomet; nonconsulting fees from Arthrex and DePuy Mitek; and royalties from Arthrex. J.F. has received education payments from Arthrex, nonconsulting fees from Arthrex, and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Greenville Health System (ref No. Pro00041492).