
Abstract
Background:
There is a paucity of literature regarding injury incidence, mechanism, and return to play in National Football League (NFL) players who have sustained traumatic posterior hip instability.
Purpose:
To describe the incidence of traumatic posterior hip instability and the rate of return to play in NFL players across 18 seasons.
Study Design:
Descriptive epidemiology study.
Methods:
We retrospectively assessed all traumatic posterior hip dislocations/subluxations that occurred during football-related activities in the NFL seasons from 2000 through 2017. Player demographics and injury data (injury mechanism, season of injury, treatment, days missed, and return to play time) were collected from all 32 NFL teams prospectively through a leaguewide electronic health record system. Descriptive statistics are presented.
Results:
Across the 18 NFL seasons, 16 posterior hip instability injuries in 14 players were reported, with a maximum incidence of 4 (25%) in 2013. Posterior hip instability was predominantly sustained by offensive players (64.3%), with tight ends being the most affected (31.3%). Half of the injuries occurred during the regular season, 43.8% in the preseason, and 6.2% in the offseason. Of all injuries, 37.5% were noncontact, while 56.3% involved contact (direct or indirect), and 6.2% were of unknown mechanism. Among noncontact injuries, 66.7% occurred during cutting and change of direction while sprinting. The time of return to full participation was documented for 11 of the 16 reported injuries (68.8%); among them, the mean time loss was 136.7 ± 83.8 days—143.3 ± 99.6 days if the player underwent surgery (n = 4) and 116.7 ± 76.2 days missed by players without surgery (n = 6)—the treatment modality was unknown in 1 player.
Conclusion:
Although the incidence of traumatic posterior hip instability during the study period was low, all injured athletes missed time from football activities and competitions. Injuries that required surgery led to more missed time than those that did not. Ongoing research to understand risk factors and mechanisms of this injury, in conjunction with improvements to prevention and rehabilitation protocols, is necessary to ensure the safety of professional American football players.
Lower extremity injuries occur frequently in the National Football League (NFL), comprising 60% of all injuries and with a reported single-season risk of 41% per athlete, thus producing a substantial burden to players and teams. 9 During the 2015-2018 NFL seasons, a mean of 2006 lower extremity injuries resulting in missed playing time were sustained each season. Of these injuries, 148 (7.4%) affected the hip. 9
There are a variety of injuries that can occur about the hip in professional NFL players, including strains, sprains, contusions of the surrounding musculature, and intra-articular injuries, such as labral tears, fractures, and dislocations/subluxations. While intra-articular injuries represented only 5% of all hip injuries in the NFL between 1997 and 2006, they resulted in the most time loss with a mean of 94.2 days (median, 94 days; range, 3-283 days) missed. 6 Traumatic hip instability events, defined as hip dislocations or subluxations, can be particularly potentially devastating because they can result in osteonecrosis and chondrolysis, predisposing the joint to rapid progression of osteoarthritis that may eventually require total hip arthroplasty. 2,10,11 Philippon et al 11 reported that 100% of athletes who underwent hip arthroscopy after sustaining a traumatic hip dislocation presented with chondral defects and injury to the labrum.
Among the general public, traumatic posterior hip dislocations are usually sustained in motor vehicle accidents when the knee hits the dashboard while the hip is both flexed and adducted, thus resulting in a posteriorly directed force on the hip. 4 A similar injury mechanism and pattern has been found in American football players, most often with a flexed and adducted hip impacting either the ground or another player, resulting in the same posterior force. A 2003 study reported that athletes were primarily diagnosed with subluxations as opposed to dislocations, which reflects the lower energy nature of the trauma. 10
In order to keep athletes safe, there has been an increased focus on improving awareness, prevention, and diagnosis of injuries at all levels of competition. However, the current literature is lacking in the epidemiology and outcomes of posterior hip instability—a rare but potentially devastating injury—in professional American football players. Consequently, the purpose of this study was to investigate the incidence, mechanism, and time loss associated with posterior hip dislocations/subluxations sustained by NFL players across 18 seasons.
Methods
This was a descriptive epidemiology study of all posterior hip dislocation/subluxation injuries sustained by NFL players from 2000 through 2017. Per the NFL collective bargaining agreement, this research was approved through both the NFL Player Scientific and Medical Research Protocol 8 and our institutional review board. The NFL electronic health record (EHR) database was utilized for this study; its use has been previously described. 5 The NFL EHR consists of customized clinical impression codes specific to American football. The inclusion criteria for this study required the presence of a clinical impression code for either a posterior hip dislocation and/or a posterior hip subluxation, either alone or in conjunction with another contemporaneous injury. The available data regarding treatment were limited to surgical treatment via the presence of the Current Procedural Terminology codes. For consistency, posterior hip dislocation/subluxation injuries will be referred to as “posterior hip instability injuries” throughout the paper.
Guidelines for injury reporting into the NFL EHR changed during the study period. Before 2012, data collection focused on voluntary reporting of specific injuries and of any injury that resulted in medical intervention or time loss from a practice or a game. From 2012 to 2014, injuries that met a “reportable injury” definition were required to be entered into the EHR, with an emphasis on those that missed time. Beginning in 2015, all injuries sustained by NFL players were mandated to be entered into the EHR, regardless of missed time.
In this study, posterior hip instability events were evaluated based on treatment (operative vs nonoperative management), circumstances of injury onset (game vs practice, season, and team activity [eg, 11-on-11, 1-on-1, offense, and defense]), mechanism (contact vs noncontact), and laterality. Player-patient characteristics were described (age, body mass index [BMI], and years of NFL experience at the time of injury). The position was recorded as the position at the time the injury was sustained. The BMI was calculated from the height and the weight taken at the time a player signed with the team. Game injuries were described by the quarter of the game in which the injury occurred. Time loss for each injury was measured in days and calculated as the number of days that passed from the date of removal from participation because of the injury until the date the player returned to full participation in football activities. Football activities refer to any activity related to practice, conditioning, team workouts, or game competition with an NFL team. Full participation means that the athlete is recovered from his injury to the extent that he can fully participate in the team’s football-related activities and is cleared for such by the medical staff.
Statistical Analysis
Descriptive statistics were calculated to determine the player- and injury-specific characteristics. Means and standard deviations were calculated for continuous variables. Because of the small sample size, a detailed statistical analysis was not performed. All statistical analyses were performed in SPSS for Mac (Version 23.0; SPSS Inc).
Results
During the 2000-2017 NFL seasons, a total of 16 posterior hip instability injuries in 14 players were reported, with the incidence ranging from 0 to 4 per season (Figure 1). Of these, 9 (56.3%) were classified as posterior hip dislocations and 7 (43.7%) as posterior hip subluxations. On average, the injured athletes were aged 26 ± 3.2 years (range, 21-31 years), with a BMI of 29.1 ± 5.5 kg/m2 (range, 18.3-38.9 kg/m2). Posterior hip instability was predominantly suffered by offensive players (64.3%), with tight ends being the most frequently affected (31.3%). Whereas most injuries occurred during the regular season (50%), 43.8% of injuries were sustained during the preseason, while only 6.2% and 0% occurred in the offseason and the postseason, respectively. Eleven out of 16 injuries occurred in a game setting with varying incidence across each of the game quarters (first quarter: n = 1; second quarter: n = 4; third quarter: n = 2; and fourth quarter: n = 3), with 72.7% and 27.3% occurring in the regular season and preseason games, respectively. Four out of 5 (80%) practice injuries happened in the preseason, while only 1 (20%) was sustained during the offseason. Regarding the injury mechanism, 37.5% of injuries were noncontact, 37.5% were reported as being due to direct contact, 18.8% were classified as due to indirect contact (ie, contact not involving the injured extremity), and 6.2% were of unknown mechanism (Table 1). Cutting and change of direction was the predominant mechanism (66.7%) in noncontact injuries.
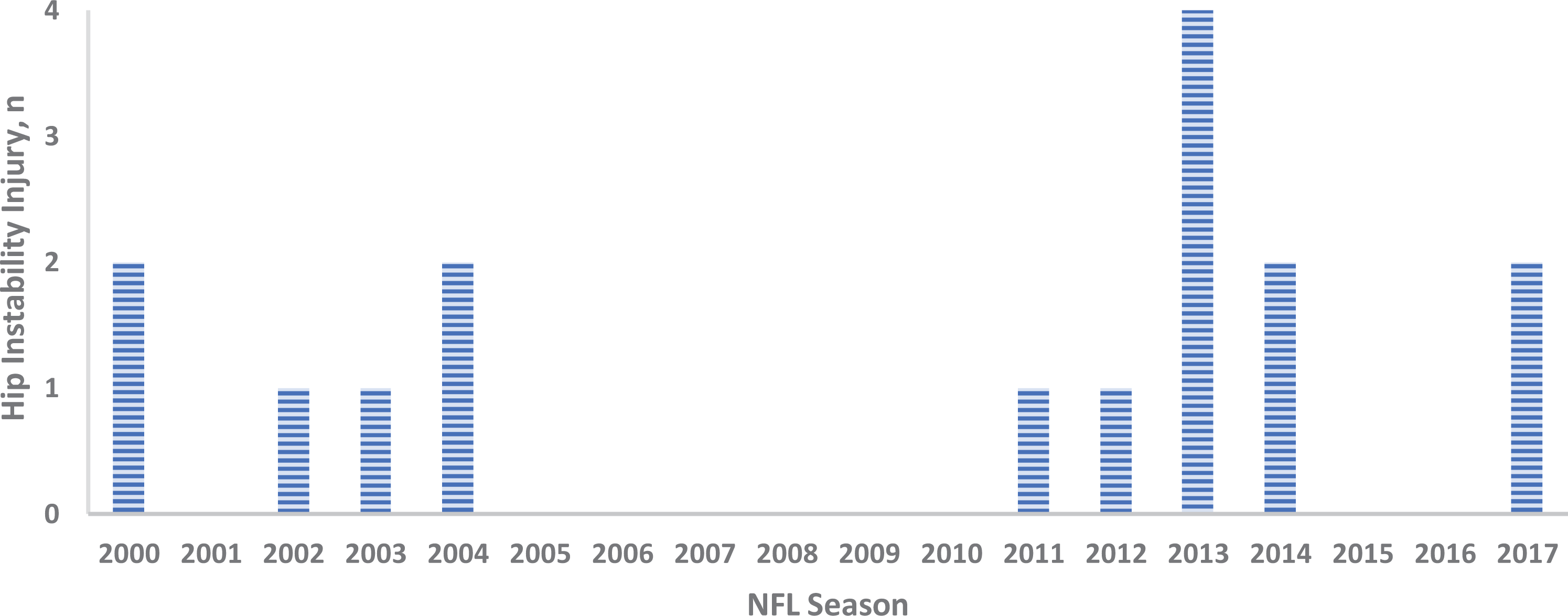
Incidence of posterior hip instability injuries in the National Football League: 2000-2017 seasons.
Player- and Injury-Specific Characteristics of Posterior Hip Instability Injuries in the NFL From 2000 to 2017, Stratified by Treatment Modalitya

a Data are reported as n (%) or mean ± SD. BMI, body mass index; NFL, National Football League.
b Information regarding operative vs nonoperative treatment was not available for 1 injured player.
c Information was available for 9 players (56.3%); 4 and 5 players underwent surgical and nonsurgical treatment, respectively.
Among players whose return to full participation date was known (n = 11/16), the mean number of days missed was 136.7 ± 83.8 days. Players who underwent surgery (n = 4) missed 143.3 ± 99.6 days, on average, compared with 116.7 ± 76.2 days missed by players whose injuries were managed nonoperatively (n = 6). One player returned after 231 days, but information on the treatment modality was not available.
Discussion
Study results indicated that the incidence of traumatic posterior hip instability in the NFL was low, with only 16 reported cases across 18 NFL seasons. This injury, however, leads to significant time loss among players, with a mean of 136.7 ± 83.8 days missed. Nearly 40% of injuries were sustained during a noncontact situation, of which the predominant mechanism was cutting and change of direction. Greater awareness among the medical and coaching staff can assist in the prevention, prompt recognition, and appropriate clinical management of this potentially serious injury in contact athletes.
In recent years, hip injuries have received considerably less attention in the media and among the scientific community than injuries to the shoulder, the knee, or the ankle, which are more common and can be more impactful in NFL prospects and active players. 1,9,13 A descriptive epidemiology study by Mack et al 9 analyzed all time loss from lower extremity injuries that occurred in the NFL during the 2015-2018 seasons. Of the 8024 lower extremity injuries sustained in the full NFL season, only 590 (7.4%) involved the hip compared with injuries to the knee (29.3%), the ankle (22.4%), the thigh (17.2%), and the foot (9.1%). In 2008, Feeley and colleagues 6 assessed the incidence and etiologic factors of intra- and extra-articular hip injuries in the NFL. Of the 738 hip injuries reported between 1997 and 2006, 59% were hip strains, and 33% were classified as contusions. In fact, only 5% of all included injuries were categorized as intra-articular (ie, fracture, labral tear, or dislocation/subluxation). However, with the current reporting mechanisms, it is certainly possible that hip subluxations may be underdiagnosed or misdiagnosed as “hip sprains” because of the transient nature of the pain and symptoms. 2,3,10 This might be even more relevant when considering that players with posterior hip instability often initially present with limited range of hip motion because of the significant pain but have a concentrically reduced hip joint and no concomitant injuries. 10
In a case series of 8 traumatic hip subluxations in American football players across a 9-year study period, Moorman et al 10 analyzed the injury mechanism and intra-articular injuries that were associated with the subluxation event. Six of the 8 players (75%) fell on a flexed knee with the hip adducted and flexed, which is the most frequently reported mechanism of injury for posterior hip instability in athletes. 2,6,7,10 As hips with traumatic posterior dislocation typically present with morphologic features of anterior femoroacetabular impingement, 11 Steppacher et al 12 theorized that with increasing flexion and internal rotation, the prominent femoral head-neck junction (cam type) and the prominent acetabular rim (pincer type) come into contact and act as a fulcrum, thus pushing the femoral head posteriorly. The finding in this study that nearly 40% of all traumatic posterior hip instability events in the NFL since 2000 occurred in a noncontact mechanism may support the hypothesis that some players may be prone to injury because of anatomical predisposition. Because the impingement position is sensitive to intra-articular injury, Feeley et al 6 suggest to routinely evaluate flexion, internal rotation, and adduction in NFL athletes, especially when considering the proposed influence of anterior femoroacetabular impingement on the risk of traumatic posterior hip instability. 12
In the absence of serious concomitant injuries, NFL players who sustained a traumatic posterior hip instability injury are initially treated nonoperatively with activity modification and toe-touch weightbearing using crutches for 6 weeks. 2,10 In the cohort reported by Moorman et al, 10 the 6 patients in whom osteonecrosis did not develop returned to full activity at a mean of 13 weeks after being instructed to use crutches and toe-touch weightbear for 6 weeks. This return to full participation is sooner than the mean 116.7 days of time loss experienced by the NFL players who were treated nonoperatively in our study. A previous study, analyzing hip injuries and labral tears in the NFL from 1997 to 2006, reported that the mean return to sport for 9 players with hip dislocation/subluxation was 126 days, with a range between 16 and 283 days. 6 This mirrors the results presented in our study, with an overall mean return to the full participation of 136.7 days (range, 20-283 days). Considering both studies covered a time of over 10 years, the return to sport after traumatic hip instability has not changed despite the more frequent utilization of sophisticated diagnostic tools, such as magnetic resonance imaging. As previously mentioned, this might stem from delayed medical attention because of the often subtle symptoms after a traumatic hip instability event. 2,3,10
The major strength of this study is the description of the mechanism and onset of this rare injury in the NFL over a course of almost 20 years utilizing the NFL’s injury database, including robust data from the electronic health record (EHR) that was implemented in 2014. The NFL EHR employs thorough data quality efforts, including regularly scheduled audits and queries for both completeness and accuracy. 5 Comprehensive and accurate reporting of injuries is essential to make reliable conclusions about the incidence, risk, burden, return to play estimates, and long-term sequelae. Consequently, studies based on public sources of injury data are likely to result in substantial levels of missing data and can thus reach invalid conclusions. 9
We acknowledge that there are limitations to this study. Although comprehensive and accurate data reporting is a strength of this study, some data were unavailable because of changes in reporting requirements of the NFL EHR over the course of the study period. This study was limited to the stratification of injury mechanism into contact and noncontact categories—the data that are reported by team athletic trainers based on in game observations and not centrally provided by video reviews. Variance and misclassification are possible. Future research could include very specific video reviews of injury onset, allowing for more detailed clinical assessment of the injury mechanism. Further, imaging data and treatment/rehabilitation progress were not included in this study. Because of the low incidence and the relatively small sample size, the current study focused on the epidemiologic description rather than the performance of the statistical testing. Last, the metrics presented here may underestimate the entire burden of posterior hip instability in the NFL because of the players leaving the NFL or the timing of the in-season injury. While the mean number of days missed due to posterior hip instability was 136.7 ± 83.8 days, this metric of days missed from NFL activities may not truly reflect the burden of this injury to individual players in terms of pain, long-term sequelae, subsequent surgeries, and potential reinjury. 10 However, the primary goal of this research is to describe injury incidence, mechanism, and return to play, which may inform injury prevention efforts and further research on the occurrence and management of these injuries.
Conclusion
Although the incidence of traumatic posterior hip instability during the study period was low, all athletes with this injury missed time from football activities and competitions. Injuries that required surgery led to more missed time than those that did not. Ongoing research to understand risk factors and circumstances surrounding the incidence of this injury, in conjunction with improvements in prevention and rehabilitation protocols, is necessary to ensure the safety of professional American football players.
Footnotes
Acknowledgment
The authors acknowledge the thoughtful editing suggestions by Dr Gary Solomon, senior advisor to the NFL Department of Health and Safety.
Final revision submitted August 31, 2021; accepted September 27, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: V.S. has received grant support from Arthrex; education payments from Liberty Surgical; and hospitality payments from Aesculap Biologics, DePuy, and Smith & Nephew. C.D.M., M.H., and J.R.P. are full-time employees of IQVIA, which is in a paid research consultancy with the National Football League for data collection, analytics, and research. M.D.P. has received education payments from Kairos Surgical, consulting fees from DePuy, and speaking fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Mount Sinai School of Medicine (ref No. Pro000601817).