
Abstract
Background:
The benefits of the interval slide (IS) procedure in retracted rotator cuff tears remain controversial.
Purpose:
The purpose was to evaluate the effect of the IS procedure on repair tension (RT). It was hypothesized that the IS procedure (anterior IS [AIS], posterior IS [PIS], and intra-articular capsular release [CR]) would reduce the RT of a supraspinatus tendon.
Study Design:
Controlled laboratory study.
Methods:
A total of 31 Thiel-embalmed human cadaveric shoulders (mean age, 74 years; range, 68-84 years) were tested. Full-thickness supraspinatus tendon tears were created, and 1 cm of tendon was resected to simulate a retracted defect. Shoulders were randomized into intervention (n = 16) and control (n = 15) groups. In all shoulders, the load during tendon reduction to footprint was measured, an endpoint was defined as maximum tendon lateralization before 50 N was reached, and the RT (load during lateralization to endpoint) of the native tendon (t1) was evaluated. In the intervention group, AIS (t2), PIS (t3), and CR (t4) were performed in order, with RT measurement after each step. In the control group, RT was assessed at the same time points without the intervention.
Results:
A complete reduction of the tendon was not achieved in any of the shoulders. Mean maximum lateralization was 6.7 ± 1.30 mm, with no significant differences between groups. In the intervention group, the overall IS procedure reduced RT about 47.0% (t1 vs t4: 38.7 ± 3.9 vs 20.5 ± 12.3 N; P < .001). AIS reduced RT significantly (t1 vs t2: 38.7 ± 3.9 vs 27.4 ± 10.5 N; P < .001), whereas subsequent PIS (t2 vs t3: 27.4 ± 10.5 vs 23.2 ± 12.4 N; P = .27) and CR (t3 vs t4: 23.2 ± 12.4 vs 20.5 ± 12.3 N; P = .655) did not additionally reduce tension. Comparison between groups at t4 revealed a reduction of RT of about 47.8% (control vs intervention: 39.3 ± 4.0 vs 20.5 ± 12.3 N; P < .001).
Conclusion:
The IS procedure reduces RT of the supraspinatus tendon in human cadaveric shoulders. However, performing PIS and CR subsequent to AIS does not reduce tension additionally.
Clinical Relevance:
These findings provide surgeons with a biomechanical rationale regarding the efficacy of the IS procedure.
Massive, retracted rotator cuff tears are challenging to treat. Despite significant improvement in surgical techniques, considerable retear rates remain. 13,26 In this regard, several risk factors like fatty infiltration and atrophy of the rotator cuff muscle have been reported. 10 In addition to the surgical reconstruction technique, repair tension (RT) is important for clinical outcome and tendon integrity. 4,12,24 Because of the natural course of tendon retraction, remodeling of tendon and muscle, and adhesions to the surrounding tissue, the mobility of a torn tendon decreases with time. 6,7 The arthroscopic interval slide (IS) procedure was introduced for severely retracted rotator cuff tears to improve tendon mobility.
Initial clinical studies 28,29 evaluating the anterior IS (AIS), where an incision is made in the anterior rotator interval between the subscapularis and supraspinatus, combined with an intra-articular capsular release (CR) reported promising results. Subsequently, Lo and Burkhart 23 advanced this procedure by adding the posterior IS (PIS), an incision between the supra- and infraspinatus tendons, and reported satisfying clinical outcomes. Furthermore, the authors postulated improved tendon mobility at 3 to 4 cm after performing the IS procedure, without providing details regarding objective assessment or statistical analysis
On the other hand, more recent investigations have shown limitations regarding clinical outcome of the IS procedure. 3,11,15 In particular, performing the PIS in addition to AIS led to remarkably higher retear rates and insufficient clinical benefit compared with partial repair without PIS. 11,15
So far, the reasons for the inferior results remain unclear. Objective biomechanical data regarding the effect of the IS procedure on RT are lacking. The aim of this study was to evaluate the effect of the IS procedure on RT in human cadaveric shoulders. We hypothesized that the IS procedure (fixed sequence of AIS, PIS, and intra-articular CR) reduces RT of the supraspinatus tendon.
Methods
Specimen Preparation
A total of 40 Thiel-embalmed 30 shoulders (donated to the Department of Anatomy of the Medical University of Graz [Graz, Austria] under the approval of the Anatomical Donation Program of the university) were used. Preparation and testing setup have previously been described by Porschke et al. 25 Briefly, the scapula was fixed in a custom-made testing station using 3 bicortical screws and avoiding damage of rotator cuff or deltoid muscles. The supinated forearm was fixed at 30° of glenohumeral abduction (determined by using a goniometer) and neutral rotation (bicipital grove pointing anteriorly, perpendicular to the scapular plane) by another bicortical screw. The humerus, elbow, forearm, and hand were left intact (Figure 1). The humeral supraspinatus insertion was exposed by performing a deltoid split approach and careful resection of the overlying subacromial bursa. The remaining bursa that did not cover the supraspinatus footprint was preserved.
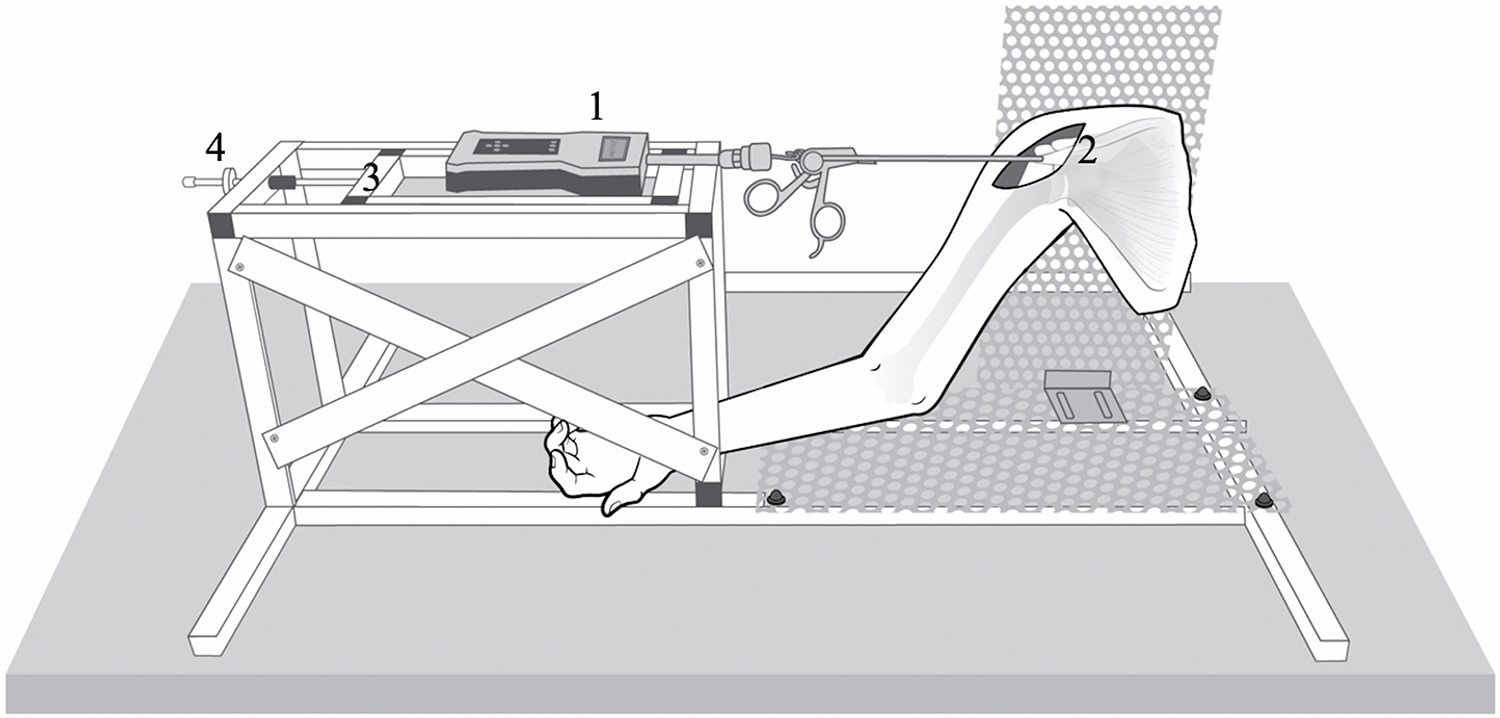
Schematic illustration of the test setup (right shoulder, anterior view). The shoulder was fixed at 30° of glenohumeral abduction. The sensor-enhanced arthroscopic grasper (1) lies aligned with the supraspinatus muscle (2), grasping the distal tendon stump of the supraspinatus. The sensor-enhanced arthroscopic grasper was lateralized in 1-mm steps via a slide (3) by using an isometric screw (4), thus reducing the tendon to the footprint. Load on the tendon was measured in real time.
At this time, shoulders were evaluated for exclusion criteria, which comprised full-thickness defects of subscapularis, supraspinatus, or infraspinatus tendons or any previous surgical procedure at the included shoulder. From 40 included shoulders, 9 were excluded owing to preexisting supraspinatus defects (n = 6) or previous surgical interventions (n = 3), leaving a total of 31 shoulders (mean age, 74 years; range, 68-84 years; 20 left and 11 right shoulders) for biomechanical analysis.
A full-thickness supraspinatus tendon tear was then created in all 31 specimens. Sharp detachment of the supraspinatus tendon insertion site was performed using a No. 15 blade starting from the anterior border and continuing 15 mm posteriorly. The supraspinatus tendon was then shortened to simulate a retracted tear by removing the distal 10 mm of the tendon. Tendon dimensions were measured using a digital caliper (myotendinous length [medial border of supraspinatus muscle insertion – lateral border of supraspinatus tendon] and the most distal tendon width after detachment and shortening of tendon). The specimens were then randomly assigned to an intervention group (n = 16) and a control group (n = 15).
Surgical Procedure (Intervention Group)
Figure 2 provides a schematic illustration of the IS procedure. For the AIS, an incision was created within the rotator cuff interval between the supraspinatus and subscapularis from lateral to medial past the articular surface of the glenoid, as described by Tauro. 28 For the PIS, an incision between the supraspinatus and infraspinatus from lateral to medial up to the glenoid rim using the scapular spine as landmark was performed, as described by Lo and Burkhart. 23 For the superior CR, a semicircular capsule incision was made between the rotator cuff and the glenoid from the AIS to the scapular spine. 23,29

Schematic illustration of the surgical procedures (right shoulder, axial view): (1) anterior interval slide: incision between the subscapularis and supraspinatus; (2) posterior interval slide: incision between the supraspinatus and infraspinatus; (3) intra-articular capsular release: juxta-glenoidal capsular incision from 2- to 10-o’clock (dashed gray line). *Supraspinatus footprint. **Sensor-enhanced arthroscopic grasper.
Assessment of RT
RT was assessed by measuring the force that was needed to advance the supraspinatus tendon stump laterally. This was performed using a sensor-enhanced arthroscopic grasper, which has been used in previous research and has demonstrated validity. 25 The sensor-enhanced arthroscopic grasper was visually adjusted to align with the tendon and muscle fibers of the supraspinatus. The device was then used to firmly grasp and hold the distal tendon stump, and stepwise lateralization (ie, reduction to the supraspinatus footprint) in 1-mm increments was performed. Load on the tendon was measured in real time (Figure 1).
To reduce the tension lost because of viscoelastic relaxation, the tendon was preconditioned by 20 cycles of lateralization to a maximum of 50 N (1 mm/5 s) 8 before definitive measurements. Then, the starting point was set after preloading to 0.5 N. The endpoint was defined for each shoulder as the point at which maximum tendon lateralization (in millimeters) before 50 N was reached, as preliminary testing had shown a high risk of tendon slippage at loads greater than 50 N. Next, the tendon was lateralized in 1-mm increments (0.1 mm/s) beginning at the starting point, with measurement of the loading force preceded by a 5-second equilibrium period. One test cycle was considered completed when the individually defined endpoint was reached. All specimens were tested 3 times, allowing a pause of 5 minutes between cycles. RT was defined as the mean load of the 3 test cycles at the endpoint.
Testing Protocol
In the intervention group, after RT evaluation of the native (retracted supraspinatus tendon tear) tendon (t1), the AIS (t2), PIS (t3), and superior CR (t4) were performed subsequently with RT testing after each procedure. The percentage change of RT was defined as changes in load relative to t1. In the control group, the measurement of RT was performed at the same time points, without any interventions.
Statistical Analysis
For quantitative variables, mean and standard deviation were calculated. RT was compared using analysis of variance (ANOVA) for repeated measurements with post hoc testing according to Tukey-Kramer using the SAS procedure, proc mixed. Test results were considered statistically significant if the corresponding P value was less than .05. For assessment of the test-retest reliability, the intraclass correlation coefficient (ICC) was calculated for every lateralization step (3 repeated test cycles), each based on a 2-way ANOVA. Agreement strength was inferred from the ICC in accordance with the recommendations of Landis and Koch. 20 ICC values were defined as follows: <0.20, poor; 0.21 to 0.40, fair; 0.41 to 0.60, moderate; 0.61 to 0.80, substantial; and >0.81, nearly perfect agreement. All statistical analyses were performed by a biostatistician of the Medical Faculty Mannheim at Heidelberg University, using the statistical software SAS (version 9.4; SAS Institute).
Results
A complete reduction of the tendon (ie, 10-mm lateralization) was not achieved in any of the shoulders. The mean maximum lateralization was 6.7 ± 1.30 mm, with no significant difference between groups. There was also no difference between the groups regarding the tendon parameters (Table 1). The ICC for test-retest reliability was 0.98, indicating nearly perfect agreement.
Tendon Parameters a

a Data are reported as mean ± SD unless otherwise indicated.
The results of the RT measurements are shown in Table 2. Within the first measurement (t1), no significant difference regarding RT was found between the groups (P = .187). In the intervention group, the overall IS procedure reduced RT about 47.0% (t1 vs t4: 38.7 ± 3.9 vs 20.5 ± 12.3 N; P < .001). In the control group, tension decreased only 3.3% within the measurement period (t1 vs t4: 40.7 ± 4.1 vs 39.3 ± 4.0 N; P < .001). Compared with the control group, RT after the IS procedure (t4) was significantly lower (47.8%) (intervention vs control: 20.5 ± 12.3 vs 39.3 ± 4.0 N; P < .001).
Results of Repair Tension Measurements a

a Data are reported as mean ± SD. Dashes indicate areas not applicable. t1, tension of the native tendon; t2, tension after anterior interval slide; t3, tension after posterior interval slide; t4, tension after superior capsular release.
b Statistically significant difference compared with previous measurement point (P < .05).
c Statistically significant difference between groups (P < .05).
In post hoc analyses, the AIS significantly reduced RT (t1 vs t2: 38.7 ± 3.9 N vs 27.4 ± 10.5 N; P < .001), whereas there were no significant differences in tension after the PIS (t2 vs t3: P = .273) or after superior capsule release (t3 vs t4: P = .655) (Table 2).
Discussion
The most important finding of this study was that the IS procedure significantly reduced RT of the supraspinatus tendon in a biomechanical model simulating retracted full-thickness supraspinatus tears. The tension was about 47% lower after performing IS compared with tendons that did not receive IS. When evaluating the sequential procedures in post hoc analyses (AIS-PIS-CR), RT after AIS decreased significantly (29.3%), whereas PIS (15.3%) and superior CR (11.5%) did not significantly add to mobility when performed after AIS.
Several factors have been identified predicting the risk of retear after tendon repair. In addition to size and configuration of the defect, 26 atrophy and fatty infiltration of the muscles have been described as risk factors. 10 Interestingly, advanced fatty infiltration correlates with an inability to achieve complete rotator cuff repair. If the infraspinatus muscle was involved, even a moderate fatty infiltration led to lower rates of repairability. 14,19 However, whether this was actually because of the fatty infiltration or rather an indicator of the advanced degenerative changes and remodeling processes with impaired biomechanical properties was not answered by these studies.
Mobility of the torn tendon is increasingly in focus in clinical practice and science as well. Because of remodeling processes, the torn tendon retracts over time. 6 In addition, biomechanical properties of the tendon deteriorate at the expense of mobility. 7 Numerous studies 16,24,27 have demonstrated that tendon retraction results in impaired clinical outcome and higher retear rates after rotator cuff repair when compared with nonretracted tendons.
In massive, retracted rotator cuff tears, direct tendon-to-bone repair without excessive tension is often difficult, and in some cases impossible to achieve. In those cases, extra-anatomic salvage procedures such as partial repair of the rotator cuff, 18 medialization of the footprint, 17,21 and superior capsule reconstruction 1 have shown satisfactory results. However, if surgeons aim to anatomically reconstruct rotator cuff tears, tendon mobility has to be adequate, which is not always the case, specifically in chronic, retracted tears. Here, extensive subacromial and intra-articular CR is often necessary. In approximately 10% of patients, however, the aforementioned procedures are not sufficient to improve tendon mobility to achieve tendon-to-bone fixation. 23 For these patients the IS procedure was implemented. Tauro 29 reported promising clinical results for the arthroscopic AIS procedure in a retrospective study. Subsequently, Lo and Burkhart 23 found significantly better active range of motion, strength, and patient-reported outcomes after the addition of a PIS procedure as well. Both authors reported a substantial improvement of tendon mobility through the IS procedure based on their subjective impression.
In contrast to prior findings, Kim et al 15 reported a lack of benefit regarding clinical outcomes in patients with additive PIS compared with patients who underwent partial repair of the supraspinatus only. In patients who underwent PIS, a retear rate of 91% in magnetic resonance imaging follow-up was reported. These high retear rates were then confirmed by Berdusco et al 3 2 years after the PIS procedure as well. The rationale for the high rerupture rates after PIS remains unclear. Limitations of all discussed studies included their retrospective designs, small patient numbers, considerable variance of tear types, and subjective assessment of tendon mobility. In summary, clinical benefits of the IS procedure remain debated.
Our findings confirm that the IS procedure can effectively reduce RT within supraspinatus tendon reduction to the footprint. With a fixed sequence of procedures (AIS-PIS-CR), we found that RT significantly decreased after the AIS alone, whereas PIS and CR had a lower effect and did not significantly add to AIS. Jeong et al 11 found inferior clinical results after the PIS, with substantially larger retear sizes in patients who underwent an additional PIS compared with patients without this rather aggressive release. The authors suggested there is a potential risk of devascularization by separating the supraspinatus and infraspinatus. One explanation for the inferior clinical results may be that the PIS does not provide a sufficient increase of mobility when performed after AIS, and therefore may not outweigh the potential risks of devascularization and overtensioning. However, our results comprise a significant confounder. The PIS has been introduced as an additional procedure to increase tendon mobility after an AIS has been performed. Therefore, in this study, a fixed sequence beginning with AIS followed by PIS and CR was used. It remains unclear whether the lower effect of PIS and CR was due to the fixed sequence or the procedures itself. This is in addition to the fact that in this study, Thiel-embalmed shoulders were tested, in which the alterations of viscoelastic properties are not well known. A subsequent study performing AIS and PIS independently would be valuable in this regard.
Limitations
Besides the lack of randomization regarding the order of procedures, further considerable limitations must be considered. Thiel-embalmed specimens were used in this investigation. The comparability of biomechanical properties of Thiel-embalmed specimens to that of native tissue was evaluated in few studies reporting heterogenic results. Some studies 9,22 found altered elastic moduli of tendons compared with fresh-frozen cadavers, while one 2 reported similar mechanical properties. The control group showed significantly lower changes in RT throughout the testing; therefore, the potential bias through altered biomechanical properties should at least be mitigated. The specimen had a high mean age of 74 years, and degenerative changes in tendon and muscle can be assumed. On the other hand, this also represents an age group in which rotator cuff tears are common. 5,31 For this investigation, artificial tears of otherwise intact tendons were analyzed, which cannot fully simulate chronic rotator cuff tears, as it is known that biomechanical capacities change in chronic rotator cuff disease. 6,7 This investigation is a point zero experiment that cannot take into account healing processes.
Conclusion
The study findings indicated that the IS procedure reduces RT of the supraspinatus tendon in human cadaveric shoulders. However, performing PIS or superior CR after AIS does not reduce tension further.
Footnotes
Final revision submitted August 14, 2021; accepted September 20, 2021.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics committee of the Rheinland-Pfalz Medical Association (837.297.17 [11131]).