
Abstract
Background:
Despite appropriate care, a subset of patients with ankle fractures has persistent pain. This condition may be associated with intra-articular pathology, which is present up to 65% of the time.
Purpose:
To quantify how much of the talus is visible through an open approach to a standard supination external rotation bimalleolar ankle fracture as a percentage of the entire weightbearing surface of the talus.
Study Design:
Descriptive laboratory study.
Methods:
Standard ankle approaches to lateral and medial malleolar fractures were performed in 4 cadaveric ankles from 2 cadavers. Osteotomies were made to simulate a supination external rotation bimalleolar ankle fracture based on the Lauge-Hansen classification. The visible segments of talar cartilage were removed. The tali were then exhumed, and the entire weightbearing superior portion of the talus was assessed and compared with the amount of cartilage removed by an open approach. The mean of the data points as well as the 95% confidence interval were calculated.
Results:
Four ankle specimens from 2 cadavers were used for these measurements. The mean surface area of the talus was 14.0 cm2 (95% CI, 13.3-14.7 cm2), while the mean area visible via an open approach was 2.1 cm2 (95% CI, 0.5-3.6 cm2). The mean proportion of the talus visualized via an open approach was 14.8% (95% CI, 3.6-26.1%).
Conclusion:
These findings indicate that the true area of weightbearing talar surface visible during an open exposure may be less than what many surgeons postulate.
Clinical Relevance:
Only a small fracture of the talus is visible via an open approach to the talus during fracture fixation. This could warrant arthroscopic evaluation of these injuries to evaluate and treat osteocondral lesions resulting from ankle fractures.
Ankle fractures remain a common orthopaedic injury requiring surgical repair. 23 Surgical management of displaced ankle fractures has been the standard of care secondary to tibiotalar incongruence or displacement predisposing to the development of early posttraumatic osteoarthritis. 2,5,18,26 However, despite appropriate treatment and restoration of alignment after ankle fracture surgical fixation, a certain subset of this population experiences poor long-term clinical outcomes. 1,9,12,29 Several studies 12,22,29 examining chronic ankle pain and osteoarthritis in patients have shown posttraumatic injury as a prevalent historical element. This subset of patients who experience poor clinical outcomes after repair of acute ankle fracture have often been described as containing occult intra-articular pathologies occurring at the time of acute ankle fracture. 4,16 Additionally, concomitant chondral lesions have been shown to be an independent predictor of the development of posttraumatic osteoarthritis and are common after an acute ankle fracture. 7,15,16,19,28 This pathology can be difficult to detect by conventional methods, including physical examination and imaging. 3,7,22
Ankle arthroscopy during the repair of acute ankle fractures has the potential to increase the detection of occult intra-articular pathologies, ligamentous damage, and syndesmotic disruptions. 1,3,7,11,16,19 However, arthroscopy after ankle fracture is not routinely performed, and there is a paucity of literature comparing outcomes of acute ankle fracture repair by arthroscopically assisted open reduction and internal fixation (ORIF) versus ORIF alone. 1,9,14 Various studies 14,16,19 suggest that arthroscopy may be valuable in improving outcomes after ankle fracture by reducing the rate of posttraumatic osteoarthritis development; however, long-term outcomes are still pending. The authors are not aware of any current literature comparing the degree of visualization arthroscopically versus open surgical visualization at the time of fixation. The purpose of this study was to quantify the degree of tibiotalar articular surface visible through a standard combined medial and lateral approach to an ankle fracture. We hypothesized that open visualization alone through the fracture fragments would be insufficient to rule out the presence of associated intra-articular pathology.
Methods
Ethics approval was obtained through our institution to utilize 2 fresh-frozen cadaveric specimens (Center for Procedural Innovation), allowing for the analysis of a total of 4 ankles. Cadavers were excluded if they contained any visible deformity through the lower extremity or surgical scars evidencing prior surgical intervention. Both specimens had minimal tibiotalar osteoarthritis. Dissection was carried out by a single researcher (K.A.P.), who made standard bimalleolar ankle fracture incisions both medially and laterally. For the lateral approach, the distal fibula was outlined and an incision was extended from 1 cm distal to the tip of the lateral malleolus to 11 cm proximal to the tip of the lateral malleolus midline along the fibula (Figure 1A). Dissection was carried to the bone, and the periosteal envelope was dissected anteriorly and posteriorly around the distal fibula and syndesmosis. For the medial approach, the medial malleolus was outlined and an incision was made contouring from 1 cm distal to the tip of the medial malleolus to 5 cm proximal along the border of the tibia (Figure 1B). Subperiosteal dissection was then carried out proximally while preserving the deltoid ligament distally.
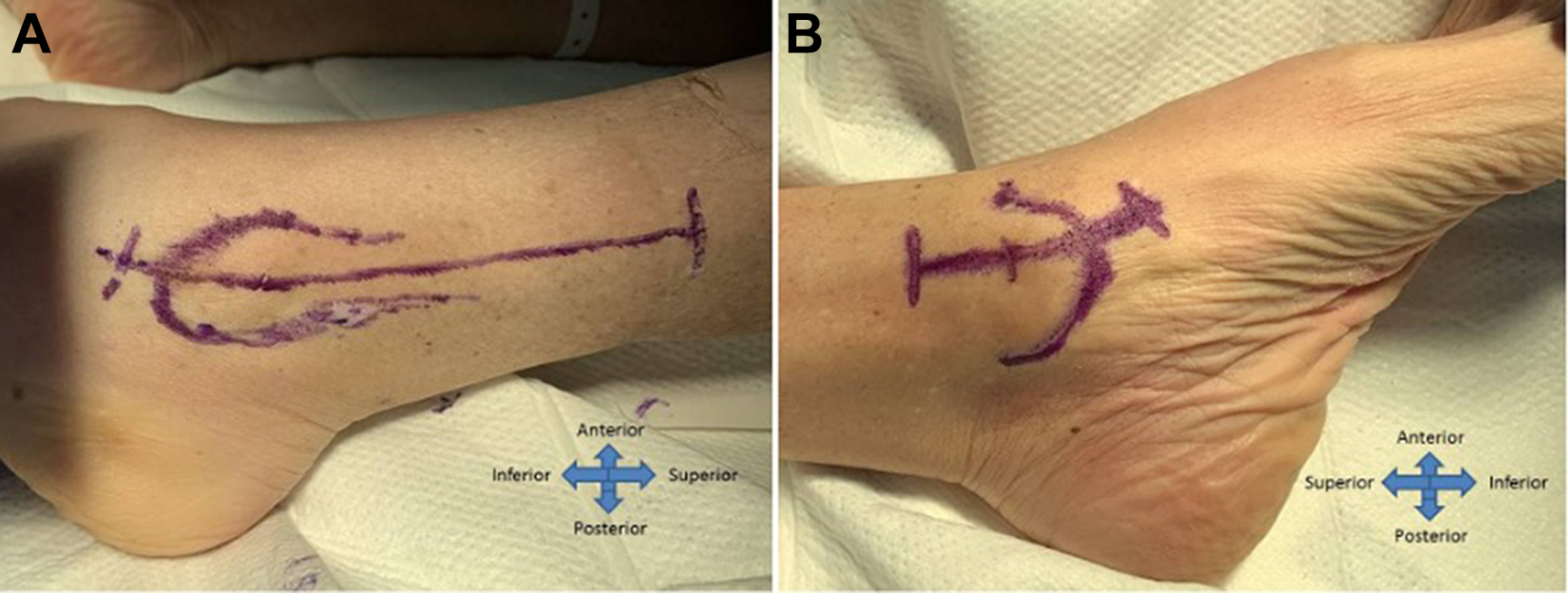
Surgical approaches to the left ankle: (A) lateral approach and (B) medial approach.
Osteotomies were made to simulate a supination external rotation bimalleolar ankle fracture based on the Lauge-Hansen classification. 24 A single researcher (K.A.P.) used an oscillating saw to initiate the cut through the use of a sharp osteotome and mallet to complete the osteotomy. Osteotomies were performed on the fibula from posterosuperior to anteroinferior, approximating a standard Weber B fibula fracture, while a transverse cut was made over the medial malleolus of the tibia (Figure 2A). The osteotomy site was cleaned with sharp dissection and a rongeur; next, a self-retaining retractor was placed to gain access to the articular surface. Sharp dissection utilizing a curette and narrow rongeur was performed on the visible segments of the talar cartilage. Complete removal of accessible and visible cartilage to the subchondral bone was performed in this manner through both medial and lateral osteotomies, ensuring that both osteotomies were complete before removal. Tibiotalar motion was utilized via ankle plantarflexion and dorsiflexion to obtain maximal visualization (Figure 2, B and C). The tali were then removed from the cadaveric specimens via amputation, and the debrided portion of the weightbearing surface was dyed with a blue surgical marker (Figure 3).

(A) Medial malleolar osteotomy by osteotome for the left ankle. (B) Exposed talar cartilage removal through lateral fibular osteotomy of the left ankle. (C) Surgical approach to medial malleolus of the right ankle, with exposed tibiotalar joint.
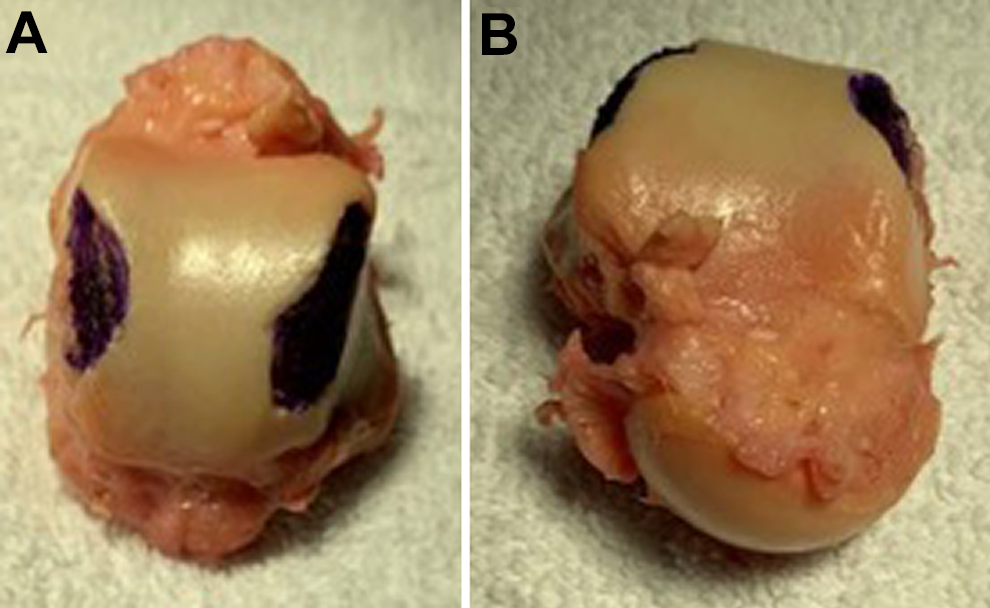
(A) Posterior and (B) anterior views of an exhumed right talus. Blue dye marking on the medial and lateral aspects of the talus represent the debrided portion of the weightbearing surface visible via surgical exposure.
To quantify the total surface of the talus, measurements were made around the contour of the weightbearing surface (Figure 4). This calculation approximated the talus to a central square (length of the posterior aspect of weightbearing cartilage × sagittal length of the weightbearing cartilage) with 2 peripheral triangles (0.5 × sagittal length of the weightbearing cartilage × [difference between coronal measurements anteriorly and posteriorly]/2). To calculate the visible portion of the talus, the length of the blue highlighted segment was multiplied by the largest width of the highlighted segment in the coronal plane. The highlighted surface area was then divided by the previously calculated total weightbearing surface to provide a percentage of talar visualization via the above-described standard bimalleolar open approach.

Measurement of medial defect on the right talus. The defect is identified by a blue surgical marker.
The primary outcome reported is the percentage of the weightbearing talar articular surface visible via an open approach. The mean of these data points and 95% confidence interval were calculated.
Results
The weightbearing portions of the 4 tali exhumed from the 2 specimens ranged from 13.5 to 14.4 cm2, with an average surface area of 14.0 cm2 (95% CI, 13.3-14.7 cm2). The smallest dimensions were routinely measured along the posterior margin of the weightbearing dome of the talus, averaging 2.3 cm in length compared with the longest dimension routinely measured, which was the lateral border of the weightbearing dome of the talus at 5.0 cm on average (Table 1).
Actual Talus Dimensions and Area Measurements

The cartilage that was removed, representing the visible portions of the weightbearing surface of the talus, created a defect (as described in the Methods section). This defect was larger on the medial side, averaging 1.2 cm2 compared with 0.9 cm2 for the lateral defect. The average total surface area of talus able to be visualized ranged from 1.1 to 2.9 cm2, with an average of 2.1 cm2 (95% CI, 0.5-3.6 cm2) (Table 2).
Actual Area of Visible Talus Through Medial and Lateral Approach With an Open Bimalleolar Fracture

The percentage of the total surface area of the weightbearing talus visible from the combined bimalleolar approach ranged from 7.6% to 20.5%. On average, 14.8% (95% CI, 3.6% -26.1%) was visualized, leaving 85.2% (95% CI, 73.9%-96.5%) of the weightbearing surface of the talus unexamined (Table 3).
Actual Area of the Talus Visible by an Open Approach as a Percentage of the Entire Weightbearing Portion of the Talus

Discussion
The current data show that the mean surface area of the weightbearing talus visible from a combined bimalleolar approach in a cadaveric specimen was 14.8% (95% CI, 3.6% -26.1%). The range of visible surface area was from 7.6% to 20.5%. This left a mean surface area of 85.2% (95% CI, 73.9%-96.5%) of the weightbearing surface of the talus unexamined.
A posttraumatic origin accounts for approximately 70% of patients with symptomatic ankle arthritis of the ankle. 7 The findings by Ramsey and Hamilton 20 in 1976 illustrate the importance of anatomic reduction, as only a 1-mm lateral shift in the talar surface will decrease contact area by 42% and drastically increase contact forces and asymmetric loading of the tibiotalar joint. The articular cartilage of the ankle surface varies from that of the hip and knee. The cartilage surface is both smaller and thinner, with greater tensile stiffness and fracture stress with aging. 13,25 These features allow a congruently maintained ankle surface to resist primary arthritis to a greater degree than would be seen in the hip and knee. 5,6,13
Our results suggest that, on average, surgeons can visualize 14.8% of the talus through an open bimalleolar approach. However, this leaves, an average, 80% to 93% of the weightbearing portion of the talus unrecognized. Additionally, visualization of the weightbearing portion of the talar dome is predominantly restricted to the lateral and medial aspects of the talus, while the greater central portion of the talar dome remains completely hidden or functionally inaccessible to the treating surgeon. Prior work has demonstrated the presence of intra-articular cartilage lesions as high as 65% of the time in association with traumatic ankle fractures. 16 Combined with our current understanding of posttraumatic arthritis and osteochondral defects of the talar surface, our data highlight the utility of concurrent ankle arthroscopy as an adjunct to ORIF of bimalleolar ankle fractures. Feiwell and Frey 10 performed a similar study in 1994 showing that the regions of the talus were accessible with curette via arthroscopic portals. When combining the anteromedial, anterolateral, and posterolateral portal sites, they noted that vast majority of the articular surfaces was accessible. The distal half of the anterior colliculus of the medial malleolus was not accessible with any portal combination at the time; however, modern 70° arthroscopes with adequate traction applied have made this region available for treatment of so-called shoulder lesions along the medial and lateral rim of the talus. 8
The majority of the traumatic chondral and osteochondral lesions that occur appear anterolaterally or medially on the talar shoulder, and therefore, these areas would be more readily accessible during an open approach for reduction of a bimalleolar ankle fracture. 15 Despite our finding that only a small portion of the talus is visualized during an open approach, there is significance to the highlighted locations allowing visualization and access to the most common areas for OCD lesions. If left untreated, these lesions may lead to impaired function, limited motion, stiffness, catching, locking, and swelling in the ankle joint. 6,18 Regier et al 21 found osteochondral lesions in 40.4% of patients who sustain displaced ankle fractures. There was a significant correlation between American Orthopaedic Foot and Ankle Society (AOFAS) scores and incidence of osteochondral lesions, and the risk of having an osteochondral lesion increased as much as 5.6% with as little as a single-point decrease in AOFAS score. 21
During exposure of the talar surface, dissection of the anterolateral capsule was avoided; this likely limited the amount of articular surface that could be exposed. In the setting of ORIF, we believe that most surgeons would not extensively dissect the anterolateral capsule because of the proximity of the anterior inferior tibiofibular ligament and anterior talofibular ligament. The capsule may obstruct a small portion of the talal weightbearing surface; however, inadvertent or overzealous release may destabilize the syndesmosis as well as generate chronic lateral ankle instability. 27 It should be noted that appropriate debridement of this area could help avoid posttraumatic impingement appearing as a Bassett ligament in later arthroscopy. 17
Limitations
There are several limitations to our study. Outside of the small sample size limiting generalizability, only 1 specific subset of fracture pattern was utilized for the assessment of visualization ability. This means that the application of these data to other fracture patterns may not be appropriate. Additionally, measurements of the talar surface and visible defects were performed by hand, bringing subjectivity of measurement into question. However, measurements were performed by several independent observers in an attempt to obfuscate any observation error. There was not an arthroscopic arm of the study to determine the percentage of the weightbearing surface of the talus visible by arthroscopic means with which to compare. Future studies should focus on comparison of arthroscopic visualization to open visualization and broaden to other common fracture patterns to determine the optimal candidate who could benefit from the addition of arthroscopy to ankle fracture fixation.
Conclusion
Although ankle arthroscopy is not routinely utilized to evaluate the joint surface during ankle fracture fixation, it may be a useful adjunct to completely visualize concurrent chondral pathology that affects a patient’s functional outcome. These data suggest that only a small fraction of the talus is visible/accessible via an open approach. This supports preexisting orthopaedic dogma; however, these findings highlight that the true area of weightbearing talar surface visible during an open exposure may be less than what many surgeons postulate.
Footnotes
Final revision submitted August 31, 2021; accepted September 27, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.D.H. has received educational support from Arthrex. D.G.D. has received educational support from Goode Surgical. T.A.K. has received consulting fees from Synthes USA, honoraria from Hologic, and hospitality payments from Medical Device Business Services and Wright Medical. M.C.D. has received grant support from NBA/GE Healthcare; educational support from Gotham Surgical; consulting fees from DePuy, Extremity Medical, Fast Form, and Pitusan 360; and royalties from Extremity Medical. K.A.P. has received educational support from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Mayo Clinic (protocol No. 20-002997).