
Abstract
Background:
Depression and anxiety symptoms can occur in patients following an anterior cruciate ligament (ACL) injury, and the presence of these symptoms has been associated with poorer self-reported knee function in this type of injury.
Purpose:
To investigate the prevalence and severity of self-reported symptoms of depression and anxiety following an ACL injury.
Study Design
Systematic review; Level of evidence, 4.
Methods:
PubMed, Cochrane Library, Embase, PsycINFO, AMED, and PEDro databases were searched using a combination of keywords relating to ACL, depression, anxiety, and their synonyms. Inclusion criteria were clinical studies written in English that reported on patients with an injured and/or reconstructed ACL and assessed symptoms of depression and/or anxiety. Data extraction was performed independently by 2 authors. Data synthesis was performed using an emergent synthesis approach. The quality of the included studies was assessed using the methodological index for non-randomized studies or the Mixed-Methods Appraisal Tool. Certainty of evidence was determined using the Grading of Recommendations Assessment, Development and Evaluation.
Results:
After abstract screening, 37 studies were assessed in full text, of which 16 were included. The studies comprised 682 patients (417 male [61%]). The depression symptoms appeared to be more severe in elite athletes compared with recreational athletes. Symptoms decreased over time from moment of ACL reconstruction to up to 2 years postoperatively. The prevalence of self-reported symptoms of anxiety after an ACL injury was reported in 1 study (2%). There were no differences in anxiety symptoms between professional and amateur athletes or between adolescents and adults. The overall quality of the studies was low or very low.
Conclusion:
Patients who sustain an ACL injury can suffer from symptoms of depression, especially during the first 6 weeks after ACL reconstruction. Depressive symptoms are more common among professional versus nonprofessional athletes. Levels of anxiety symptoms were not above the cutoffs for a diagnosis of anxiety after an ACL injury.
An injury to the anterior cruciate ligament (ACL) is a common, severe, sports-related injury, treated with rehabilitation and optional surgery. 20 Regardless of whether patients undergo surgical treatment, the rehabilitation is demanding and usually takes at least 1 year. 10 During rehabilitation after an ACL injury, patients can develop negative psychological reactions, 16,28,51 such as an increase in anger, negative emotions, and lower self-esteem. 14 Symptoms of depression and anxiety are also examples of psychological reactions that can follow an ACL injury or other acute orthopaedic trauma.
There are 9 symptoms of depression: (1) depressed mood that may be characterized by sadness, emptiness, or hopelessness; (2) markedly diminished interest or pleasure in all or almost all activities; (3) significant unexpected weight loss; (4) inability to sleep or oversleeping; (5) psychomotor agitation or retardation; (6) fatigue or loss of energy; (7) feelings of worthlessness or inappropriate guilt; (8) diminished ability to think, concentrate, or make decisions; and (9) recurrent thoughts of death, suicidal ideation without a specific plan, or a specific suicide attempt or specific plan for committing suicide. 52 Depression has been reported in up to 34% of ACL injuries, while, after a musculoskeletal injury, the incidence of depression is reported to be as high as 45%, 16 which is higher than in the general population. 16,35
When negative psychological reactions are not correctly addressed, they can negatively affect rehabilitation and treatment outcome, as an inferior psychological outcome has been associated with poorer rehabilitation outcomes after ACL reconstruction. 23,39,42 Negative psychological reactions to an ACL injury can persist for many years. 7 Furthermore, patients who return to their preinjury level of sport and do not perform as well as before the ACL injury report fear of reinjury or lack of self-confidence as reasons. 39 Specifically, depression and anxiety have been associated with poorer self-reported knee function after an ACL injury. 21 This is in agreement with preoperative symptoms of depression and anxiety being associated with a poorer outcome after surgery following many orthopaedic procedures. 1,2
As symptoms of depression and anxiety can occur in patients after an ACL injury and negatively affect the treatment outcome, there is a need for knowledge regarding the prevalence and severity of symptoms of depression and anxiety in patients with an ACL injury. The aim of this systematic review was to investigate the prevalence and severity of self-reported symptoms of depression and anxiety after an ACL injury.
Methods
This systematic review was performed in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 47 We prospectively registered this systematic review in the international prospective register of systematic reviews (PROSPERO No. CRD42020181678).
Literature Search Strategy
An electronic search was performed by a librarian with expertise in medical electronic searches at Sahlgrenska University Hospital Library, Gothenburg (Sweden) on May 25, 2020. In the search strategy, we used a combination of Medical Subject Headings relating to ACL, depression, anxiety, and their synonyms, from inception to May 25, 2020. The search terms and search results are described in Table 1.
Search Terms and Search Results a

AMED, Allied and Complementary Medicine Database; PEDro, Physiotherapy Evidence Database.
a Search terms used: Depression OR Depressive Disorder OR Anxiety OR Anxiety disorders OR Psychology OR depression OR depressive OR depressed OR antidepress OR anti-depress OR anxiety OR trepidation OR angst OR psychology OR psychologi OR psychosocial AND Anterior Cruciate Ligament Reconstruction OR Anterior Cruciate Ligament Injuries OR anterior AND cruciate AND ligament OR ACL.
Study Selection Process
Two authors (R.P. and T.B.) separately screened abstracts for inclusion and exclusion. In the event that an abstract did not contain information that could inform decision-making, that study was included in the full-text assessment. The full text of eligible studies were then read. When necessary (eg, inclusion of patients <16 years or studies that did not report answers to the patient-reported outcomes [PROs] used), the authors of the original study were contacted for additional data. Any disagreement on eligibility was resolved in consensus and by discussion with the senior author (E.H.S.). The Cohen kappa coefficient showed moderate agreement between the reviewers on study eligibility (κ = 0.57). 31
Eligibility Criteria
The eligibility criteria were randomized controlled trials, longitudinal studies, cohort studies, case-control studies, cross-sectional studies, and qualitative studies that were written in English and published in peer-reviewed journals, included patients aged 16 to 65 years with an injured and/or reconstructed ACL, and assessed symptoms of depression and/or anxiety with PROs. Studies published as opinion pieces and/or editorials, other review studies, and studies assessing symptoms of depression and/or anxiety without using PROs tested for psychometric properties were excluded.
Outcomes
In the present systematic review, the outcome of interest was the presence and severity of self-reported symptoms of depression or anxiety given on psychometric-tested PROs. The type of outcome measurement used, the time of administration (from baseline injury/reconstruction), and the eventual effect on a treatment outcome were used as additional outcomes.
Data Extraction and Synthesis
Two authors (R.P. and T.B.) extracted data independently using an Excel spreadsheet (Version 16; Microsoft Corp). Extracted data consisted of author, journal, purpose, publishing year, study quality, statistical analysis, sample size, time of follow-up, study population, outcomes, results, and conclusion.
Data synthesis was performed using an emergent synthesis approach, which provides a systematic approach to synthesizing varied literature in a topic area that includes diverse data types. 44 The results were summarized in narrative expression and summary and in tables, according to the proposed method. 44 The results were structured with subheadings, including appraisal of evidence, depression, and anxiety. Owing to heterogeneity in the collected data regarding outcome measurements, a percentage was calculated by dividing the mean score from the outcome used in a study by the highest possible score of the used outcome's measurement to summarize findings relating to the severity of depression and anxiety. Results were presented as percentages (0%-100%) of the PRO used to assess the outcome of interest.
When the emergent synthesis approach allowed and after the data had been summarized, the certainty of evidence was determined using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) Working Group methodology (www.gradeworkinggroup.org). 4 The evidence was defined as of high, moderate, low, or very low certainty by considering potential limitations due to risk of bias, inconsistency, indirectness of results, imprecision, and publication bias. 4 The included studies received an initial GRADE evaluation (low or high) depending on the study design, then each evaluation was successively downgraded, maintained, or upgraded depending on the study's execution.
Quality Assessment of Individual Studies
The included studies were assessed using the methodological index for non-randomized studies (MINORS). 45 The studies were independently graded by 2 authors (R.P. and T.B.), and any disagreements were resolved by consensus. The MINORS consists of 8 items for noncomparative studies and 12 items (4 additional items) for comparative studies. Each item is graded from 0 to 2 points, with 0 representing an item not reported, 1 representing an item reported inadequately, and 2 representing an item reported adequately; thus, the maximum score is 16 for noncomparative and 24 for comparative studies. The quality scores can be interpreted as follows: for noncomparative studies, 0 to 4 = very low, 5 to 8 = low, 9 to 12 = fair, and 13 to 16 = high; for comparative studies, 0 to 6 = very low, 7 to 12 = low, 13 to 18 = fair, and 19 to 24 = high. 45
A critical appraisal of the included qualitative studies was performed using the Mixed-Methods Appraisal Tool (MMAT). 26 The MMAT includes 2 screening questions and assesses studies according to category based on the study methods.
Results
The search resulted in 838 studies, of which 388 were duplicates. The 450 unique studies were uploaded in the Rayyan QCRI 40 web application for systematic reviews for the screening and selection process (Figure 1). A total of 37 studies were eligible and assessed in full text. Of these, 8 studies were excluded for the following reasons: 4 were doctoral dissertations, 2 were conference papers, 1 study was a trial registration only, and 1 did not report any measurement of anxiety or depression. Of the remaining 29 studies, 3 were excluded because no validated outcome measurement was used. For the remaining 26 studies, we contacted the corresponding authors of 15 by email, because 11 studies included patients 21 younger than 16 years and 4 studies did not report answers to the outcome measurements used. We received responses from the authors of 5 studies, of which 2 were based on the same cohort. 7,8 We therefore extracted data from 16 studies # comprising 682 patients (417 male [61%]). A summary of the included studies is shown in Table 2.

Flowchart of the study inclusion process. *Other sources: gray literature and reference lists of included studies.
Summary of the Included Studies (N = 16) a
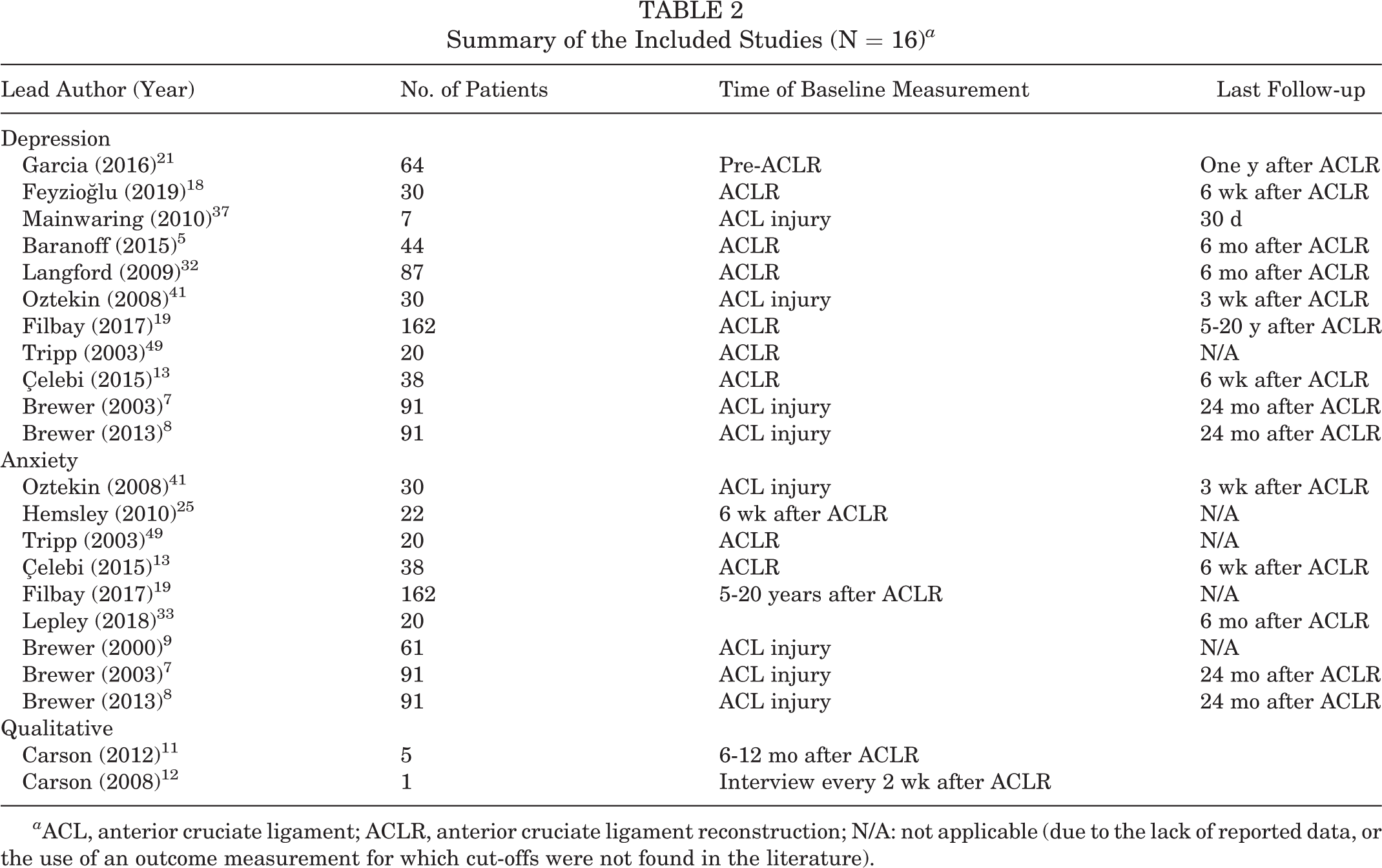
a ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; N/A: not applicable (due to the lack of reported data, or the use of an outcome measurement for which cut-offs were not found in the literature).
Quality Appraisal
When grading the quality of the evidence using GRADE, all but 2 studies 37,41 (which were graded very low quality) were assessed as having low quality. The 2 studies with very low quality were downgraded owing to risk of bias, imprecision, and indirectness of results (Table 3).
Quality of Evidence Using the GRADE a

a GRADE, Grading of Recommendations Assessment, Development and Evaluation.
b Assessment based on study design (high or low).
c Assessment after rating the evidence using GRADE (high, moderate, low, very low).
d Downgraded owing to risk of bias, imprecision, and indirectness of results.
e Downgraded owing to risk of bias.
There were 7 noncomparative studies 5,7 –9,13,19,33 and 7 comparative studies 18,21,25,32,37,41,49 assessed with the MINORS. The noncomparative studies had a median score of 9 of 16 (range, 5-11), indicating that they were of fair quality. The comparative studies had a median score of 16 of 24 (range, 10-18), and all but 1 study 25 scored between 13 and 18, thereby indicating fair quality (Table 4). The most frequent methodological weakness was the lack of a prospective calculation of study size and an unbiased assessment of the study endpoint. The methodological strengths were the clearly stated aims and the prospective collection of data.
Quality Assessment Using the MINORS a

a MINORS, methodological index for non-randomized studies; N/A, not applicable (noncomparative studies).
b MINORS items: (1) clearly stated aim; (2) inclusion of consecutive patients; (3) prospective collection of data; (4) endpoints appropriate to the aim of the study; (5) unbiased assessment of the study endpoint; (6) follow-up period appropriate to the aim of the study; (7) loss to follow-up <5%; (8) prospective calculation of the study size. Additional criteria for comparative studies: (9) adequate control group; (10) contemporary groups; (11) baseline equivalence of groups; (12) adequate statistical analyses.
The 2 qualitative studies 11,12 were assessed using the MMAT. One study 12 used a mixed method and was assessed with the 5 questions on qualitative methods and the 5 questions on mixed methods. The qualitative part of the mixed-methods study was of good quality; however, the questions about the quantitative method could not be answered due to the way the authors had reported quantitative data. 12 The other study 11 was assessed with the 5 MMAT questions about qualitative methods. 27 The total scores are reported in Table 5.
Quality Appraisal Using the MMAT a
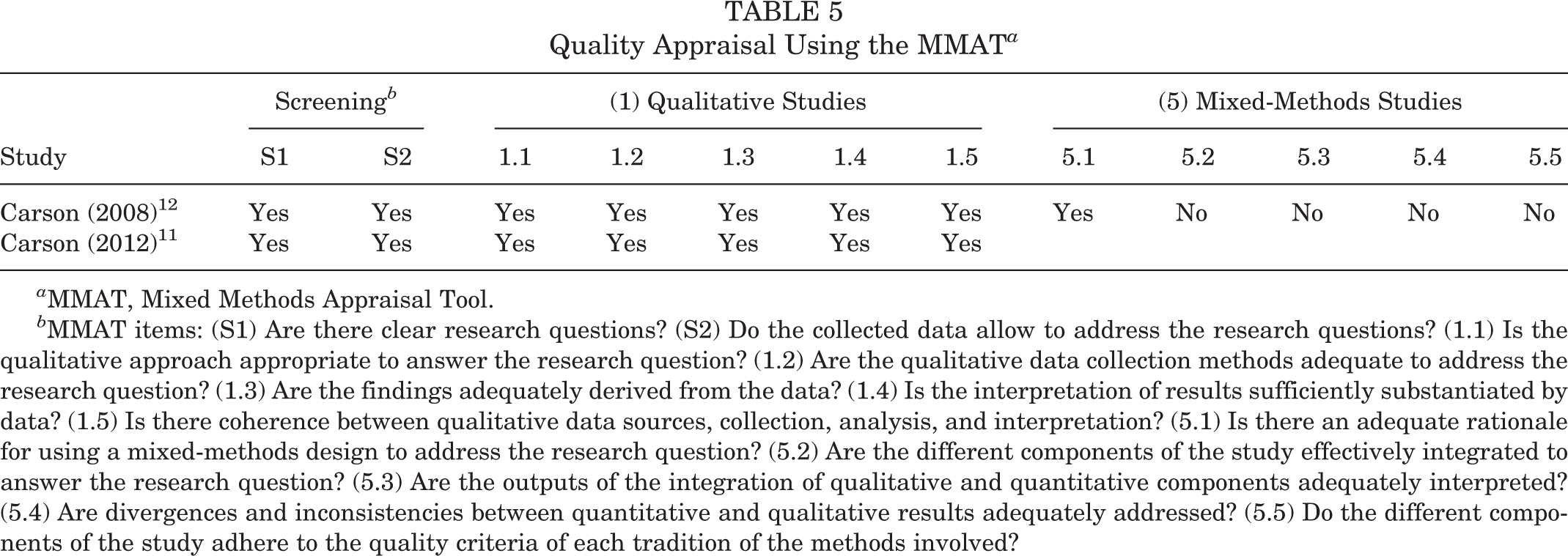
a MMAT, Mixed Methods Appraisal Tool.
b MMAT items: (S1) Are there clear research questions? (S2) Do the collected data allow to address the research questions? (1.1) Is the qualitative approach appropriate to answer the research question? (1.2) Are the qualitative data collection methods adequate to address the research question? (1.3) Are the findings adequately derived from the data? (1.4) Is the interpretation of results sufficiently substantiated by data? (1.5) Is there coherence between qualitative data sources, collection, analysis, and interpretation? (5.1) Is there an adequate rationale for using a mixed-methods design to address the research question? (5.2) Are the different components of the study effectively integrated to answer the research question? (5.3) Are the outputs of the integration of qualitative and quantitative components adequately interpreted? (5.4) Are divergences and inconsistencies between quantitative and qualitative results adequately addressed? (5.5) Do the different components of the study adhere to the quality criteria of each tradition of the methods involved?
Depression
Measurement of depression symptoms
Of the 16 included studies, 11 were studies ** that measured symptoms of depression using various outcome measurements. Three studies 18,41,49 used the Beck Depression Inventory, 6 2 studies 13,19 used the Hospital Anxiety and Depression Scale 53 (HADS), and 2 studies 8,37 used the Profile of Mood States 22 (POMS). The remaining measures used were the Quick Inventory of Depressive Symptomatology, 43 Depression Anxiety and Stress Scale, 36 Emotional Response of Athletes to Injury Scale, and Brief Symptom Inventory 17 (BSI), which were used in 1 study each. 5,7,21,32 In addition, 1 qualitative study 12 reported depression as a theme. Comprehensive extraction results, including outcomes for measurements of depression and depressive symptoms in the included studies, are summarized in Appendix Table A1.
Severity of depression symptoms
The severity of symptoms of depression was reported according to the published cutoffs for the outcome measurement used (Appendix Table A1). Three studies 13,18,41 compared the severity of symptoms of depression between professional and recreational athletes, showing a higher rate of severity for symptoms of depression both before and after ACL reconstruction and before and after accelerated rehabilitation in professional athletes when compared with recreational athletes. In addition, higher levels of symptoms of depression were reported in athletes who suffered an ACL injury compared with athletes who suffered a concussion or with healthy controls. 37
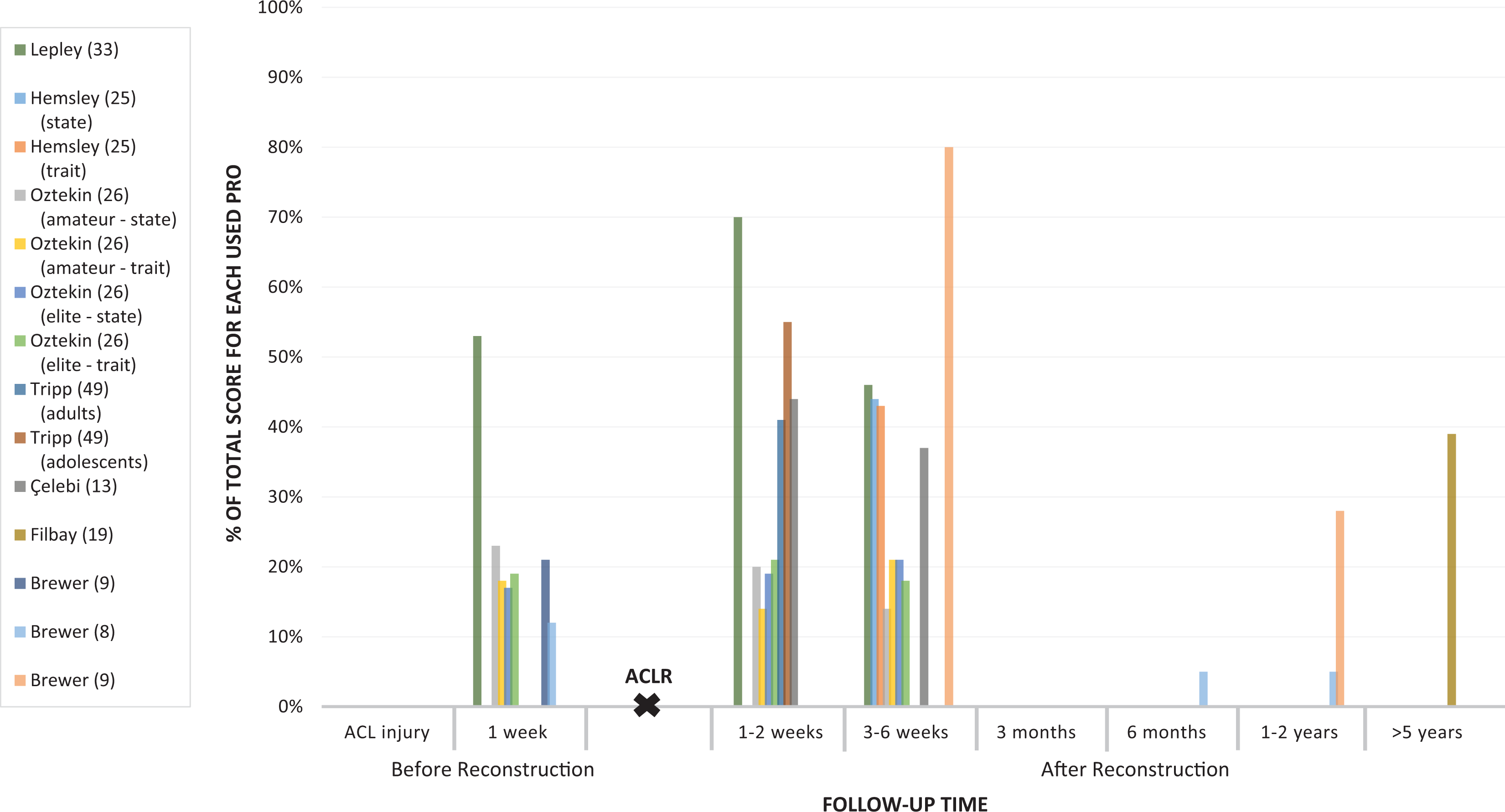
A proposed “severity grade” for symptoms of depression is presented on a timeline comprising follow-ups after an ACL injury (Figure 2). The severity grade was calculated by dividing the mean score provided in the study by the highest possible score in the used outcome measurement, to create a rating of outcomes from 0% to 100%.

Severity of symptoms of depression. Percentages were calculated by dividing the mean patient-reported outcome (PRO) value provided in the study by the highest possible score for that measurement. ACL, anterior cruciate ligament; ACLR, ACL reconstruction.
Symptoms of depression appeared to be more severe in elite athletes, and they decreased in all patient categories over time, from time of ACL reconstruction to 2 years after ACL reconstruction. 13,18,41
Prevalence of depression
When analyzing the prevalence of depression symptoms that result in a depressive disorder as based on cutoffs of self-reported PROs among patients with an ACL injury, 1 study 21 reported that 42% of the included patients (n = 27) had major depressive disorder (MDD) before ACL reconstruction. The patients in the MDD group had lower self-reported knee function 1 year after ACL reconstruction. 21 Further, Filbay et al 19 assessed depressive symptoms 5 to 20 years after an ACL reconstruction. In a total of 162 patients, 6% had possible depression and 1% were likely to have depression. Lower rates of symptoms of depression have been associated with a higher return-to-sport rate. 19
Depression over time
There were 7 studies 5,8,13,18,21,32,37 that compared the severity of symptoms of depression over time. A decrease in symptoms of depression over time was reported in 4 of these studies. 8,13,18,21 Two studies analyzing symptoms of depression over time inferred that the severity of symptoms may vary from ACL reconstruction to within 6 months of follow-up, as 1 study 13 (38 professional athletes) did not find any differences from immediately after ACL reconstruction to 6 weeks later, and 1 study 5 (44 patients) detected an increase in symptoms of depression from 2 weeks after ACL reconstruction to 6 months later. There were no reported differences in symptoms of depression between adults (>18 years old) or adolescents (16-18 years old) in the 24 hours after ACL reconstruction. 49 However, symptoms of depression were detected 2 weeks after ACL injury, before ACL reconstruction and late in the rehabilitation before return to sport in 1 professional rugby player. 12
Symptoms of depression and rehabilitation adherence
Three studies 7 –9 investigated the association between psychological factors and rehabilitation adherence after ACL reconstruction and reported that more negative mood and stress were associated with a lower adherence to rehabilitation. However, no values above the cutoffs for depression, that is, values indicating depression in the outcome measurement in the studies, were reported.
Anxiety
Measurement of anxiety symptoms
Of the 16 included studies, 8 studies 7 –9,13,19,25,41,49 assessed symptoms of anxiety after ACL injury and/or reconstruction. Three studies 25,41,49 assessed symptoms of anxiety using the State-Trait Anxiety Inventory, 46 2 studies 13,19 used the HADS, 1 study 7 used the BSI, 1 study 8 the POMS, and 1 study 33 used the European Quality Five Dimension. 30 In addition, the 2 qualitative studies 11,12 were included. In studies assessing state and trait anxiety, state anxiety was defined as anxiety about an event, and trait anxiety was defined as anxiety level as a personal characteristic.
A proposed severity grade for symptoms of anxiety is presented on a timeline comprising follow-ups after an ACL injury (Figure 3). The severity grade was calculated by dividing the mean score provided in the study by the highest possible score of the used outcome measurement, to create a rating of outcome from 0% to 100%.
Severity of anxiety symptoms. Percentages were calculated by dividing the mean patient-reported outcome (PRO) value provided in the study by the highest possible score for that measurement. ACL, anterior cruciate ligament; ACLR, ACL reconstruction; state, state anxiety (anxiety level about an event); trait, trait anxiety (anxiety level as a personal characteristic).
Severity of anxiety symptoms
There were no reported differences in the levels of symptoms of anxiety between adults (>18 years old) and adolescents (16-18 years old), between patients who recover knee range of motion quickly (<6 weeks to recover 125° of knee flexion) and patients who recover knee range of motion slowly (>6 weeks to recover 125° of knee flexion) after ACL reconstruction. There was also no difference in the presence of anxiety symptoms between professional and recreational athletes. 18,25,49 However, professional rugby players were identified as having feelings of anxiety before return to sport. 11 A case study 12 of 1 rugby player reported perceived symptoms of anxiety directly after ACL reconstruction. A summary of included studies on anxiety after ACL injury is presented in Appendix Table A2.
Anxiety over time
Concerning changes in symptoms of anxiety over time, levels of symptoms of anxiety decreased from time of ACL reconstruction to 6 weeks and up to 6 months after surgery. 13,33 A decrease in the levels of symptoms of anxiety was detected, although the values, that is, values indicating anxiety in the outcome measurement used in the studies, were not over the cutoff for anxiety as a diagnosis at any time. At long-term follow-up, 1 study 19 described 73% of patients reporting no anxiety, 19% reporting possible anxiety, and 2% reporting a likelihood of having anxiety 5 to 20 years after ACL reconstruction.
Discussion
The main finding in this systematic review was that the severity of symptoms of depression and anxiety in patients with an ACL injury is higher at an early stage (1-6 weeks) after ACL reconstruction and that symptoms of depression, but not anxiety, are more severe in elite athletes compared with recreational athletes.
A recent study analyzing level 1 athletes 2 years after ACL reconstruction highlighted that most patients who have not returned to play reported that was because of external life and psychological factors associated with their injury, including fear of reinjury and lack of confidence in performance. 48 These reasons could perhaps underline symptoms of depression or anxiety. Moreover, many clinical studies that describe players not returning to sport do not investigate depression when, in reality, psychological issues may be present as well, since an inferior psychological outcome has been linked with poorer rehabilitation outcomes after ACL reconstruction 23,39,42 and may persist for many years. 7 Psychological support was not provided in any of the studies included in this review, and a systematic review from 2018 found only 4 randomized controlled trials that had limited evidence and inconsistent results. 15 For this reason, the next step is a call for interventional studies designed to improve ACL outcomes with psychological interventions.
Depression
The results of this study are in line with the previous literature, 16 indicating that depression symptoms are present after orthopaedic trauma. The results in this systematic review are limited and of low quality, but they are consistent in indicating that the prevalence and severity of depressive symptoms after an ACL injury are higher in professional athletes than in nonprofessional and recreational athletes. 18,41 This is in accordance with studies investigating the general responses of athletes to sport injuries, where elite athletes have been reported to have a slower psychosocial recovery and to experience greater mood changes than recreational athletes. 38 Taken together, elite athletes appear to experience more severe depressive symptoms following an ACL injury than recreational athletes. In a clinical setting, athletes experiencing more severe depressive symptoms suggest the need to create awareness of screening for depression. Depression screening can be performed using validated questionnaires and, if symptoms are present, there should be an opportunity for a treatment referral to qualified health care professionals trained in treating depressive symptoms.
The severity of symptoms of depression appears to peak soon after (1-6 weeks) the ACL reconstruction. The severity of symptoms of depression then appears to decrease during the first 6 weeks of rehabilitation. 12,18,21,32 It is, however, possible that individuals suffering from psychological distress run a higher risk of suffering an orthopaedic injury. 50 The question arises of whether patients’ previous mood state contributes to the injury and the high incidence of symptoms of depression following an ACL injury, or whether the high incidence of symptoms of depression is an effect of the ACL injury itself. Unfortunately, the data summarized in this systematic review are unable to address this question, but it should be mentioned that psychological variables are able to predict sport-related injuries. 29
Regarding the prevalence of depression as a disorder, in a population of patients with ACL injury and/or reconstruction, based on published cutoffs of the PRO used, 2 studies reported prevalence of depression as a disorder. Close to the time of ACL reconstruction, up to 40% of patients received a diagnosis of depression, while 5 to 20 years after ACL reconstruction, 6% of patients reported depression. The prevalence of depression in a worldwide meta-analysis of studies between 1994 and 2014 was 12.9%. 34 The prevalence of depression in a population of patients with ACL injury and/or reconstruction therefore appears to be higher than in the general population at the time of reconstruction but appears to decrease to a level lower than that of the general population up to 20 years after reconstruction. However, only 2 studies in the present review reported the prevalence of depression, and the results should therefore be assessed with caution.
Anxiety
The evidence relating to symptoms of anxiety after an ACL injury was heterogenic, scarce, and of low quality, concluding that the values were not above the cutoff for anxiety as a diagnosis at any time and that there were no differences in the symptoms of anxiety between professional and amateur athletes, or between adolescents and adults, following an ACL injury. However, anxiety was reported as a major theme in the 2 qualitative studies, 11,12 which identified an increase in perceived symptoms of anxiety before a return to sport. A systematic review reported that a common reason for patients not returning to sport is a fear of reinjury, also described as reinjury anxiety. 3 As a result, anxiety could affect patients after an ACL injury and reconstruction, but further studies are warranted to obtain a better knowledge of when and to what extent patients suffer from anxiety after an ACL injury.
Study Strengths and Limitations
The limitations in the present systematic review include the small number of studies and patients included, with different methods of assessing depression and anxiety. In overall terms, the included studies were of low to very low quality. The lack of sample size calculations in the studies was a limitation, given that there may be type 2 errors. Furthermore, when evidence from the included studies was summarized as narrative expressions, it was graded as being of low quality, with 2 studies scoring very low quality. The low grade of evidence was mainly due to the nature of the studies, as no randomized controlled trials were included. The initial GRADE for all the included studies was low.
The patient populations in the included studies were heterogenic, including age differences, level of sport, and type of sport, and a variety of different outcome measurements to assess depression and/or anxiety were used, thus leading to difficulties synthesizing results.
It is also important to note that results in this review summarized self-reported symptoms of depression and/or anxiety and not the presence of actual clinical diagnosis of depression or anxiety. Further, in the studies included in this systematic review, 6 different outcome measurements were used to assess depression, while 5 different outcome measurements were used to assess anxiety, leading to several limitations. One limitation is that in the outcome measurements used to determine depression/anxiety, some measured symptoms and some measured depression/anxiety according to the Diagnostic and Statistical Manual of Mental Disorder, fifth edition, section 2 criteria for depression or generalized anxiety disorder. Scales not based on a predefined description of an outcome of interest may have different definitions for either depression or anxiety, leading to less reliable conclusions concerning the severity of diagnosis. It is not known whether “moderate” depression on one scale is comparable with “moderate” depression on another.
Most of the included patients were male (60%). However, there is a higher risk of sustaining an ACL injury among female patients, 20 and the actual incidence of ACL injuries is approximately 50-50 between the sexes. 24 This is a limitation because there might be differences in the symptoms of depression and anxiety related to sex. All the included qualitative research was conducted on male patients, excluding the opportunity for comparisons between sexes or direct conclusions related to female patients. Another limitation regarding the qualitative research was that there were few (n = 6) included patients.
Despite few studies and heterogeneity in data, no study with a follow-up later than 6 weeks after ACL reconstruction reported symptoms of anxiety and depression above the cutoffs for the diagnosis of anxiety or depression. The evidence in the included studies was graded as low quality, with 2 studies scoring very low quality, which affects the strength of the results from this systematic review, implying that readers should assess our results with caution.
Conclusion
Patients who sustain an ACL injury can suffer from symptoms of depression, especially during the first 6 weeks after ACL reconstruction. Symptoms of depression are more common among professional athletes with an ACL injury compared with nonprofessional athletes. Levels of symptoms of anxiety were not above the cutoffs for a diagnosis of anxiety following an ACL injury.
Footnotes
Acknowledgment
The authors acknowledge Kajsa Magnusson at Sahlgrenska University Library for the professional help with the literature-searching process.
Final revision submitted September 2, 2021; accepted September 27, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
APPENDIX
Summary of Included Studies on Anxiety After ACL Injury a

| Lead Author (Year) | Population | Outcome Measure b | Baseline Measurement | Follow-up | Time of Follow-up, Type of Patient, Outcome Values, Mean ± SD | |
|---|---|---|---|---|---|---|
| Baseline | Follow-up | |||||
| Oztekin (2008) 41 | 30 (20 elite and 10 amateur athletes) | STAI | Day before ACLR | Wk 1 and 3 after ACLR | State/trait: Amateurs, 18.4/14.5 Elite, 14/15.9 |
State/trait: Wk 1: amateurs, 16.3/11.4; elite, 15.8/16.8 Wk 3: amateurs, 11.4/16.8; elite, 16.8/14.8 |
| Hemsley (2010) 25 | 22 patients | STAI | 6 wk after ACLR | NR |
State: 34.8 ± 10.6 Trait: 35.7 ± 10.1 |
NR |
| Tripp (2003) 49 | 20 patients (10 adults and 10 adolescents) | STAI (S) | 24 h after ACLR | NR | State: Adolescents, 44.4 ± 12.4 Adults, 33.8 ± 8.7 |
NR |
| Çelebi (2015) 13 | 38 elite athletes | HADS | Immediately after ACLR | 6 wk after ACLR | 6.2 ± 3.5 | 5.3 ± 3.3 |
| Filbay (2017) 19 | 162 patients | HADS | 5-20 y after ACLR | NR | 5.5 ± 3.7 | NR |
| Brewer (2003) 7 | 61 patients | BSI | Before ACLR | NR | 46.3 | NR |
| Lepley (2018) 33 | 20 patients | EQ5D | Before ACLR | 2 wk and 6 mo after ACLR | 1.6 |
2 wk: 2.1 6 mo: 1.4 |
| Brewer (2013) 8 | 91 patients | POMS | Before ACLR | 6, 12, and 24 mo after ACLR | 3.1 ± 2.5 |
6 mo: 1.4 ± 1.5 12 mo: 1.2 ± 1.6 24 mo: 1.5 ± 1.6 |
a ACLR, anterior cruciate ligament reconstruction; BSI, Brief Symptom Inventory; EQ5D, European Quality Five Dimensions; HADS, Hospital Anxiety and Depression Scale; NR, not recorded; POMS, Profile of Mood States; S, state subscale; STAI, State and Trait Anxiety Inventory.