
Abstract
Background:
Shoulder and elbow overuse injuries are the most common problems in baseball players. No scoping review has compared the findings from different types of evidence.
Purpose:
To map the broad evidence from 3 types of evidence (epidemiological, biomechanical, and narrative) on potential risk factors for shoulder and elbow injuries in baseball and identify gaps in the existing literature to guide future research.
Study Design:
Scoping review.
Methods:
Eight electronic databases were searched from inception to May 14, 2020. Any peer-reviewed papers that investigated or discussed potential risk factors for shoulder and elbow injuries in baseball were included.
Results:
A total of 302 studies (107 epidemiological studies, 85 biomechanical studies, and 110 narrative reviews) were included. Risk factors were categorized into 9 domains: sports profiles, physical characteristics/functions, pitching mechanics, performance, behavioral, psychosocial, biological and developmental, injury/sports profiles, and environmental factors. Studies were consistent in supporting limited shoulder range of motion (ROM) and player positions (pitchers or catchers) as risk factors for shoulder injuries. For elbow injuries, the majority of the included studies suggested that being pitchers or catchers and working with higher ball velocity can be risk factors.
Conclusion:
Findings were consistent in some risk factors, such as limited shoulder ROM and positions. However, findings were inconsistent or limited for most factors, and substantial research gaps were identified. Research assessing those factors with inconsistent or limited evidence in the current literature were recognized to be priorities for future studies.
Overuse injuries in the shoulder and elbow are the most common problems in baseball players. 15 One study 6 reported that shoulder pain was the most common complaint, accounting for 14.1% to 20.6% of all injuries in adult amateur players. Another study 10 found that 275 of 2055 (13.4%) youth players reported episodes of pain in the throwing shoulder. Elbow injuries represent between 16% and 22% of all injuries in a professional baseball league. 4,21 At the youth level, the frequency of elbow pain among pitchers was reported to be 26%. 13 Pitchers have been reported to experience a greater proportion of shoulder and elbow pain as compared with the other position players due to the greater physical demands on the upper limb. 21,23 Furthermore, shoulder injuries among pitchers tend to be more severe compared with injuries of position players. 12 Despite more scientific information on preventive care and the advance of medical management, shoulder and elbow injury rates in baseball appear to be rising. 4,8 Potential consequences of shoulder and elbow injuries include time lost from the sport, lower performance, surgical interventions, and early retirement. These can have detrimental impacts on future careers of baseball players.
Recent systematic reviews 1,2,5,22 suggest that increased mechanical load (measured by pitch count or training hours), higher pitching velocity, and decreased shoulder range of motion (ROM), especially in flexion, internal rotation, and horizontal adduction, are potential risk factors for both shoulder and elbow injuries. While there are concerns with respect to the safety of the curveball in pitchers, there is limited evidence, and this suggests no difference to the risk of shoulder or elbow injuries compared with the fastball. 7,18 Some evidence 3,24,26 suggests that weakness of shoulder abductors and external rotators can contribute to shoulder pain. However, this evidence seems to be contradictory and inconclusive in terms of the contribution of humeral retrotorsion as a predictor of shoulder and elbow injuries. 17,20 Limited evidence implies scapular dysfunction is not associated with subsequent upper extremity injuries in baseball. 16 Despite the clinical emphasis on lower limb, trunk function, and related kinematics for injury prevention and rehabilitation, research evidence is very limited. 11
Although there have been systematic reviews that synthesize the evidence on this topic, some limitations are to be acknowledged. Some previous reviews 1,2 used the term “arm pain” and did not strictly differentiate shoulder pain from elbow pain. This might be misleading for clinicians and researchers. Additionally, previous systematic reviews tended to include only epidemiological studies, such as cohort studies, case-control studies, and cross-sectional studies, excluding biomechanical studies with kinematic or kinetic parameters or narrative reviews with expert opinions. Considering these challenges, the purpose of this scoping review is aimed at mapping the broad evidence from 3 types of evidence (epidemiological, biomechanical, and narrative) on potential risk factors of shoulder and elbow injuries in baseball and identifying current research gaps.
Methods
This scoping review was written in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). 25 A study protocol was developed before the commencement of this review. A protocol was registered with the Open Science Framework (https://osf.io/gvrty/). The clinical question of this review was the following: What are the known risk factors for shoulder and elbow injury in baseball?
Data Sources and Search Strategy
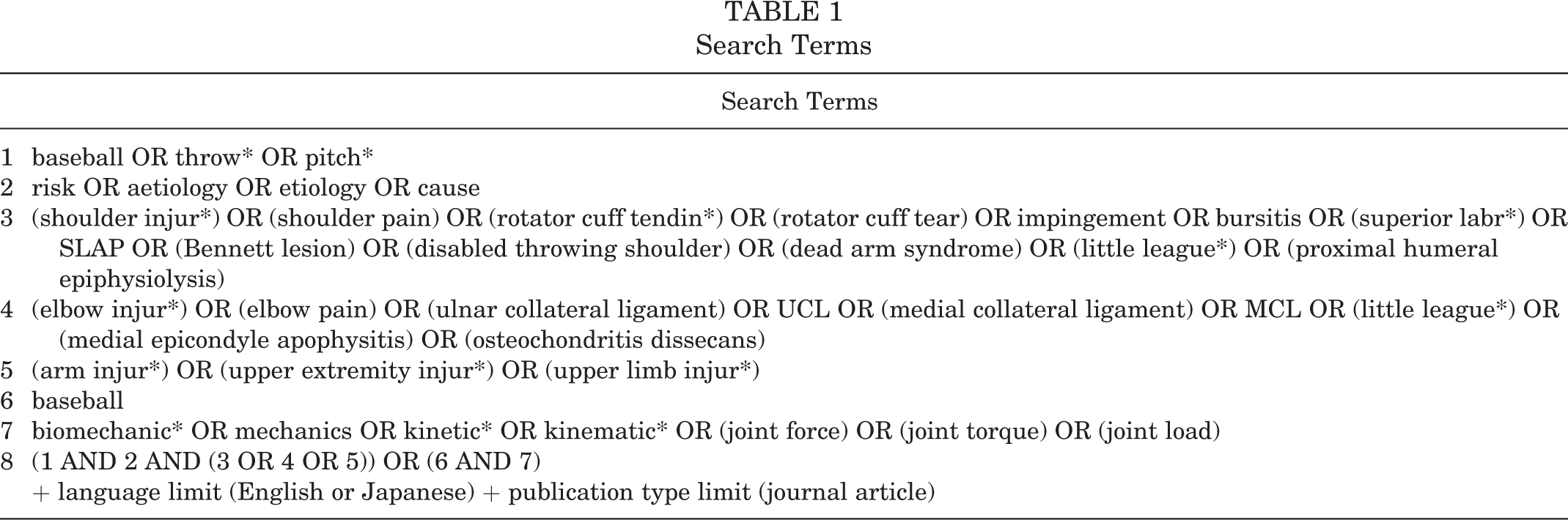
A total of 8 electronic databases were used for a systematic search in order to identify relevant studies from inception to May 14, 2020. MEDLINE, Embase, Ovid Emcare, Cochrane Library, SPORTDiscus, and Scopus were searched using English words. Ichushi and CiNii were searched in the Japanese language. A search strategy was developed through a preliminary search of relevant systematic reviews. 1,2,5,18,22 General search terms are provided in Table 1 and were modified depending on technical restraints and language differences in each database. Searches were limited to English or Japanese languages of papers published in peer-reviewed journals and conducted by 1 author (K.M.). A search was also performed to find relevant papers in reference lists of identified systematic reviews. The first 200 references, found through a complementary search using Google Scholar, were also screened. Searches were managed using the reference software EndNote X9 (Clarivate Analytics).
Search Terms
Eligibility Criteria and Study Selection
Eligibility criteria are shown in Table 2. Eligible studies were categorized into 3 types: epidemiological, biomechanical, and expert opinions. Epidemiological studies attempt to correlate physical, technical, or environmental factors to shoulder or elbow injuries and may adopt various study designs, such as cohort studies, case-control studies, cross-sectional studies, and case-series study designs. Biomechanical studies analyze associations between shoulder and elbow kinetic and kinematic parameters and potential risk factors. Kinetic and kinematic values are used as surrogate outcome measures of risk because of the associated mechanical stress on the shoulder and elbow joints they create. Greater kinetic or kinematic values are thought to indicate greater mechanical stress for the joints to resist external forces and torques. 2,19 This approach to the study of risk factors for shoulder and elbow injuries will primarily involve cross-sectional laboratory studies. Narrative reviews were included when expert opinions were explicit on specific risk factors without necessarily citing previous studies. Studies were excluded when participants included athletes of other overhead sports or athletes with traumatic upper limb injuries.
Screening of titles and abstracts and assessment of full texts were performed by 2 independent reviewers (K.M. and N.T.). Both reviewers were physical therapists, fluent in both English and Japanese. Disagreements in study selection were resolved by consensus-based discussion. Searches and the following screening were managed using the reference software EndNote X9 and Microsoft Excel. Duplicates were identified in the search functions in EndNote and excluded.
Eligibility Criteria

Data Extraction
One independent reviewer (K.M.) extracted data, which were then verified by another independent reviewer (N.T.) to ensure accuracy. Data were processed using Microsoft Excel. Data were extracted on the following items: authors, title, year of publication, study design, language used, country of origin (based on where sample population came from), study population characteristics (age, sex, positions, handedness, and eligibility criteria), outcome measures for dependent variables (injury occurrence or upper limb kinetics/kinematics), outcome measures for independent variables (examined risk factors), kinematic/kinetic measurement methods, and key findings with statistical analyses related to the review question. Two age categories were used based on the mean age of each participant group: youth (17 years of age or younger) and adult (18 years of age or older). If the reporting of important data (research designs, sample sizes, participants’ mean ages, positions, definitions of injuries, and experimental conditions for pitching) was incomplete, corresponding authors were contacted via email to obtain additional information. Data were treated as missing when there was no reply within 1 month of email contact.
Data Synthesis
A descriptive analysis and mapping of the data were conducted. Data were summarized according to research methods/types and specific risk factors. Since some epidemiological studies analyzed cases with shoulder and elbow injuries collectively, the term “arm injuries” was defined and used as “shoulder or elbow injuries” in this paper. Synthesized findings were categorized as consistent, inconsistent, or limited with research gap on each specific factor. For the convenient purposes of this review, the synthesized findings were regarded as consistent when there were 5 or more epidemiological studies and 75% of the studies supported or negated a certain risk factor. Findings were considered to be inconsistent (1) when there were 5 or more epidemiological studies and there was no agreement in at least 75% of the studies for a certain factor or (2) when there were 5 or more epidemiological and biomechanical studies, respectively, and the majority of epidemiological studies showed the opposite results as the majority of biomechanical studies. Findings were regarded to assume a research gap (1) when there were 5 or more biomechanical studies and at least 75% of them supported or negated 1 factor and there were fewer than 5 relevant epidemiological studies or (2) when there were 5 or more narrative reviews and fewer than 5 epidemiological studies.
Results
Study Selection
A flowchart of the study selection is illustrated in Figure 1. The initial search in the 8 databases yielded 6054 papers, of which 467 were eligible for full-text assessment. Of these, 173 studies were excluded for the following reasons: narrative reviews without original expert opinions on risk factors (n = 127), no relevant analysis (n = 21), no relevant outcome measure (n = 17), and heterogeneous participants including other overhead athletes (n = 8). Five studies were retrieved from the references of 14 identified systematic reviews, and 3 papers were identified through Google Scholar searches. As a result, a total of 302 papers were ultimately included for this review (a full list of the included studies is available as supplemental material). Agreement rates between the 2 reviewers were 97.6% and 92.8% in the first and second screenings, respectively.

Flowchart of study selection.
Characteristics of the Included Studies
Of the 302 included studies, 107 were epidemiological studies (35%), 85 biomechanical studies (28%), and 110 narrative reviews (36%) (Figure 2). Two hundred seventy papers were written in English (89%), while the other 32 papers were in Japanese (11%). Most studies were from the United States (n = 231; 76.5%), and the rest were from Japan (n = 59; 19.5%), Taiwan (n = 4; 1.3%), Australia (n = 3; 1.0%), South Korea (n = 2; 0.7%), and the United Kingdom (n = 1; 0.3%). Two studies (0.7%) compared pitchers from different countries (the United States and Japan/South Korea). Of 59 studies that came from Japan, 32 papers (55%) were written in Japanese, and the other 27 papers (45%) were written in English. Throughout the last 40 years, the number of published papers on this topic increased substantially: 6 papers published in 1981-1990, 23 papers in 1991-2000, 89 papers in 2001-2010, and 184 papers in 2011-2020 (Figure 3). This rising trend was particularly notable in epidemiological and biomechanical studies during the last 2 decades. As a result, the majority (61%) of the included papers were published from 2011 to 2020.

Number of articles by study design.

Number of articles by publication year.
In terms of participants’ ages, 53 epidemiological and 35 biomechanical studies investigated only youth baseball players (<18 years of age). The mean ages for youth players ranged from 10.0 to 17.6 years. On the other hand, adult players (≥18 years of age) were exclusively recruited in 50 epidemiological and 42 biomechanical studies. The mean ages ranged from 19.5 to 30.0 years. Of 92 papers with adult players, most studies examined either professional players (n = 45) or collegiate players (n = 25).
Total player sample sizes were 64,197 and 4956 for 107 epidemiological and 85 biomechanical studies, respectively. The figure for epidemiological studies included duplicate participants in longitudinal studies. From a total of 69,153 players, the majority were male (n = 68,669; 99.3%), and the rest were female (n = 484; 0.7%) players. Of the 192 primary studies, 7 papers (4%) did not provide data regarding player positions. Half of the total players were pitchers (35,353 players; 51%), followed by 1845 infielders (3%), 1652 outfielders (2%), and 465 catchers (1%). A total of 18,762 players (27%) were unspecified position players (nonpitchers), and positions were unclear for 11,076 players (16%). Of the 192 primary studies, 126 papers (66%) did not report the information regarding player handedness, which makes the handedness of 63,373 players unknown. The other 66 papers (35%) recruited 5780 players, most of whom were right-handed (n = 4510; 78%); the rest were left-handed (n = 1270; 22%).
Examined or proposed risk factors were classified into the 9 domains, each of which was either modifiable or nonmodifiable. There were 6 domains categorized as modifiable (sports profiles, physical functions/characteristics, pitching mechanics, pitching performance, behavioral, and psychosocial), and 3 domains categorized as nonmodifiable (biological and developmental, injury/sports profiles, and behavioral and environmental factors). A conceptual model on examined or proposed risk factors is shown in Figure 4. As mound height and pitching distances are determined by age-specific regulations, these environmental factors were regarded as nonmodifiable (injury/sports profiles).

Examined or proposed risk factors of shoulder and elbow injuries. BMI, body mass index; ROM, range of motion.
In epidemiological studies, the most examined domain of risk factors was physical functions. Of 53 specific independent variables, the most common variables were age (n = 36); shoulder ROM (n = 31); defense positions (n = 28); workload (n = 28); height, weight, or body mass index (BMI, n = 25); shoulder strength (n = 15); length of baseball experiences (n = 15); ball velocity (n = 11); pitch type (n = 11); and hip mobility (n = 10) (Figure 5).

Independent variables in epidemiological studies. Blue bars indicate modifiable factors and red bars nonmodifiable factors. BMI, body mass index; EMG, electromyography; RC, rotator cuff; ROM, range of motion; RTP, return to play; S/E, shoulder/elbow.
In 86 biomechanical studies, dependent variables (kinematic/kinetic parameters as surrogate outcomes for injury risk) included the following: elbow varus torque (n = 63), shoulder internal rotation torque (n = 47), shoulder proximal force (n = 31), maximum external rotation (MER) (n = 31), shoulder horizontal adduction torque (n = 21), and shoulder anterior force (n = 17). The most investigated domain of risk factors in biomechanical studies was pitching mechanics, followed by pitching performance. Of 29 specific examined risk factors, common factors were as follows: trunk kinematics (n = 16), ball velocity (n = 15), shoulder kinematics and kinetics (n = 12), pitch types (n = 11), fatigue or workload (n = 9), and age or competition level (n = 6) (Figure 6).

Examined independent variables in biomechanical studies. BMI, body mass index; COG, center of gravity; ROM, range of motion.
A total of 86 narrative reviews proposed 18 potential risk factors for shoulder injuries without citing primary studies. The most common proposed risk factors were suboptimal scapular kinematics during throwing (n = 19), glenohumeral internal rotation deficit (GIRD) or decreased total ROM (n = 19), capsuloligamentous laxity (n = 16), poor throwing mechanics (n = 13), excessive workload (n = 11), decreased rotator cuff strength (n = 10), inefficient kinetic chain from lower limbs and trunk (n = 8), decreased scapular muscle strength (n = 8), decreased lower limb muscle strength (n = 7), decreased trunk strength (n = 6), decreased hip mobility (n = 5), and immature skeletons for specific osteochondral problems among youth players (n = 5). A total of 48 narrative reviews proposed 21 potential risk factors for elbow injuries without presenting empirical data. The most common proposed risk factors were immature skeletons for specific osteochondral issues among youth players (n = 15), excessive workload (n = 14), poor throwing mechanics (n = 12), decreased wrist flexor strength (n = 6), capsuloligamentous laxity (n = 5), and pitcher or catcher position (n = 5).
Consistent Findings From the Current Literature
Consistent findings across the included studies are summarized in Table 3. Studies were consistent in supporting shoulder ROM (GIRD, posterior shoulder tightness, and limited flexion/external rotation) and being pitchers or catchers as risk factors of shoulder injuries. Limited shoulder ROM was suggested to be a risk factor of elbow injuries by most epidemiological studies as well; however, findings were inconsistent for arm injuries. When data were analyzed based on age groups (youth vs adults) to mediate this discrepancy, it became clear that all the epidemiological studies recruiting adult players led to positive results, and all negative findings came from studies with youth players. The odds ratios were 5.1, 1.3, and 1.7 for shoulder, elbow, and arm injuries, respectively. 27 This suggests that limited shoulder ROM can be a risk factor of shoulder and elbow injuries among adult players. Most studies agreed that older age may not affect the risk for shoulder injuries among youth players. However, it should be mentioned that the ranges of participant ages were relatively small (3-5 years) across the 6 studies, and those narrow age ranges might have contributed to the negative findings. In addition, none of the 6 papers considered the effects of dropouts.
For elbow injuries, the majority of the included studies suggested that being pitchers or catchers and as well as dealing with higher ball velocity can be risk factors. Most studies also suggested that shoulder strength, handedness, and pitching role are not risk factors of elbow injuries. Consistent findings were available for increased workload and being pitchers or catchers as risk factors of arm injuries. As presented in Table 3, findings were consistent for workload as a risk factor of shoulder and elbow injuries. Further analysis based on age groups found that studies with youth players were more likely to lead to positive results. The odds ratios were 2.4, 1.9, and 1.9 for shoulder, elbow, and arm injuries, respectively. 27 This indicated that increased workload may be a risk factor of shoulder and elbow injuries in youth players. Overall, being a pitcher or catcher was the only common risk factor for shoulder and elbow injuries with consistent findings.
Summary of Consistent Findings a

a Numbers in parentheses are shown as the number of studies investigating youth players to the number of studies investigating adult players. BS, biomechanical studies; ES, epidemiological studies; NR, narrative reviews; ROM, range of motion.
b Number of studies that showed significantly greater forces/torques in the shoulder/elbow joints in later innings.
c Number of studies that showed no significant change in forces/torques in the shoulder/elbow joints in later innings.
Inconsistent Findings From the Current Literature
Findings were inconsistent in terms of hip mobility, workload, and length of baseball experiences as risk factors of shoulder injuries (Table 4). Findings for age, workload, length of baseball experiences, pitch type, weight or BMI, hip mobility, and elbow ROM as risk factors of elbow injuries were inconsistent across the included epidemiological studies. The ratios of youth and adult players were reasonably comparable between supporting and negating papers, except for workload and hip mobility. When studies were performed among youth populations, the findings were more likely to be positive. The findings on workload were discussed previously. In terms of hip mobility, the odds ratio was 3.0, implying that restricted hip mobility may contribute to elbow injuries in youth players. 27 When shoulder and elbow injury data were analyzed collectively as arm injury, findings were inconsistent in humeral retrotorsion. Further analysis did not identify any characteristic tendency by different age groups.
Summary of Inconsistent Findings a

a Numbers in parentheses are shown as the number of studies investigating youth players to the number of studies investigating adult players. BE, baseball experiences; BMI, body mass index; BS, biomechanical studies; ES, epidemiological studies; NR, narrative reviews; ROM, range of motion.
b Number of studies that showed significantly greater forces/torques in the shoulder/elbow joints in later innings.
c Number of studies that showed no significant change in forces/torques in the shoulder/elbow joint in later innings.
Research Gaps in the Current Literature
A summary of evidence gaps is shown in Table 5. Although the majority of biomechanical studies found that trunk kinematics, shoulder kinematics and kinetics, pitch type (fastball), and higher ball velocity were associated with significantly higher shoulder forces or torques, there were only 3 epidemiological studies investigating these factors. Although there is strong biomechanical evidence suggesting that those factors can affect shoulder forces or torques, it is still unclear whether they are risk factors of injuries. Many narrative reviews proposed that scapular kinematics during pitching, shoulder laxity, scapular alignment, lower limb muscle strength, trunk strength/endurance, and young age are risk factors of shoulder injuries. However, there were limited numbers of studies to judge their clinical opinions.
Findings from biomechanical studies were consistent in suggesting that shoulder kinematics and kinetics, trunk kinematics, and arm anthropometric features were associated with higher elbow varus torque. However, there were small numbers of epidemiological studies testing those factors (Table 5). Although being a youth player, lower grip strength, and elbow joint laxity were suggested to be risk factors of elbow injuries by many narrative reviews, very few epidemiological studies examined these hypotheses.
Most biomechanical studies agreed that trunk kinematics, shoulder kinematics and kinetics, arm slot, weight, and BMI can affect mechanical stress in the shoulder and elbow joints; however, very few epidemiological studies were available for those factors (Table 5). Although many narrative reviews supported scapular kinematics in pitching, being a youth player, shoulder and scapular strength, and hip mobility as potential risk factors of arm injuries, only a small number of epidemiological studies were identified.
Summary of Limited Findings With Research Gaps a

a BMI, body mass index; BS, biomechanical studies; ES, epidemiological studies; NR, narrative reviews; S/E = shoulder/elbow.
Discussion
Summary of Main Results
The objective of this scoping review was to map the broad evidence on potential risk factors of shoulder and elbow injuries in baseball and identify current research gaps. This review found 302 English- and Japanese-language studies, including epidemiological studies, biomechanical studies, and narrative reviews with original expert opinions. Overall, there was a variety of studies exploring different potential risk factors. Examined factors were categorized into the 9 areas, each of which was either modifiable (sports profiles, physical functions/characteristics, pitching mechanics, pitching performance, behavioral, and psychosocial) or nonmodifiable (biological and developmental, injury/sports profiles, and behavioral and environmental). Some examined factors had consistent findings across the included studies, while others had inconsistent or limited findings with significant research gaps.
Studies were consistent in supporting shoulder ROM (GIRD, posterior shoulder tightness, and limited flexion/external rotation) and certain positions (pitchers or catchers) as risk factors of shoulder injuries. Limited shoulder ROM, positions (pitchers or catchers), and higher ball velocity were reported to be risk factors for elbow injuries by most studies. Included studies consistently suggested that shoulder strength, handedness, and pitching role are not risk factors of elbow injuries. Consistent findings were available for increased workload and positions (pitchers or catchers) as risk factors for arm injuries. Moreover, consistent findings were also available to suggest that shoulder strength, handedness, and pitching roles may not be risk factors of elbow injuries.
Findings were inconsistent in terms of hip mobility, workload, and length of baseball experiences as risk factors of shoulder injuries. Findings for age, workload, length of baseball experiences, pitch type, weight or BMI, hip mobility, and elbow ROM as risk factors of elbow injuries were inconsistent across the included studies. Since age, workload, and length of baseball experiences can also be affected by inclusion criteria in each study, this finding should be interpreted carefully. We also compared the numbers of epidemiological studies recruiting youth and adult players within supporting and negating study groups (Table 4). For instance, most of the studies recruiting youth players suggested workload as a risk factor of shoulder and elbow injuries, whereas the majority of studies with adult samples concluded that workload was not a risk factor. Thus, potential confounding factors, such as player age, may exist in those inconsistent findings. Although the majority of biomechanical studies found that trunk kinematics, shoulder kinematics and kinetics, pitch type (fastball), and higher ball velocity were associated with significantly higher shoulder forces or torques, there were only a few epidemiological studies investigating these factors. Many narrative reviews proposed that scapular kinematics during pitching, shoulder laxity, scapular alignment, lower limb muscle strength, trunk strength/endurance, and being a youth player are risk factors of shoulder injuries. However, there were very few clinical studies to judge those expert opinions. The absence of primary studies on scapular kinematics may be due to technical difficulties to precisely track the scapular movements in high-speed baseball pitching motions.
Strengths and Limitations
This scoping review is the first comprehensive review to collate findings from different types of studies, such as epidemiological studies, biomechanical studies, and narrative reviews on risk factors of shoulder and elbow injuries in baseball players. Most existing systematic reviews have focused on specific epidemiological studies and specific factors. 2,5,9 The extensive search strategy in this review enabled us to map the broad evidence with a bird’s-eye view and localize the research gaps existing in the current literature. Additionally, this review is the first study attempting to synthesize Japanese-language studies as well as English-language papers on this topic. The inclusion of 32 papers written in Japanese was thought to be a reasonable success to lessen the language barrier and minimize the publication bias. 14
There are some limitations to be acknowledged and reflected on in this review. First, although language bias was decreased to some extent because of the inclusion of Japanese-language papers, the bias may still remain because we did not consider other languages. Considering that we found some papers from Taiwan (n = 4) and South Korea (n = 2), it is possible that we might have missed published papers written in Mandarin or Korean. Second, findings were synthesized in an unweighted manner without a careful consideration of levels of evidence or the methodological quality of each study. This simplified method to evaluate the findings as consistent, inconsistent, or limited might have led to imprecise assessments of the evidence. Third, the participants in the included studies were biased to American male players. Thus, the findings may not be generalizable to different groups of players, such as female or male players in different countries. Lastly, we did not consider potential heterogeneity in the methods to analyze motion data in biomechanical studies (eg, optoelectronic devices vs wearable gyroscopic sensors).
Implications for Future Research
This scoping review identified potential risk factors with inconsistent or limited findings that require further research to achieve stronger evidence. Particularly, future research needs to investigate shoulder ROM among youth players and workload and hip mobility in adult players. Factors supported by biomechanical studies, such as trunk kinematics, shoulder and elbow kinematics and kinetics, pitch type, ball velocity, and arm anthropometric parameters, need to be examined by future epidemiological studies. Factors that appeared predominantly in narrative reviews (eg, scapular kinematics and shoulder and elbow joint laxity) need to be investigated in primary studies to test those hypotheses. Research priorities and rationales are outlined in Table 6.
Research Priorities a

a BMI, body mass index; ROM, range of motion.
Considering the abundance of biomechanical literature (n = 85) measuring various kinematic and/or kinetic parameters as surrogate outcome measures for injury risks, there is an urgent need for future epidemiological studies assessing those parameters as potential risk factors of injuries. We hope that the findings in this review will be integrated into the broader evidence by future reviews with papers written in other languages, such as Korean and Mandarin. As participants were heavily biased to American male players, studies on female or male players from other countries are also necessary.
Findings were considered to be inconsistent (1) when there were 5 or more epidemiological studies and there was no agreement in at least 75% of the studies for a certain factor or (2) when there were 5 or more epidemiological and biomechanical studies, respectively, and the majority of epidemiological studies showed the opposite results as the majority of biomechanical studies. Findings were regarded to assume a research gap (1) when there were 5 or more biomechanical studies and at least 75% of them supported or negated 1 factor and there were fewer than 5 relevant epidemiological studies or (2) when there were 5 or more narrative reviews and fewer than 5 epidemiological studies.
Conclusion
This scoping review identified 302 relevant studies (107 epidemiological, 85 biomechanical, and 110 narrative papers), investigating a variety of potential risk factors of shoulder and elbow injuries in baseball players. Findings were consistent in some risk factors, such as being pitchers or catchers and limited shoulder ROM. However, findings were inconsistent or limited for most factors and substantial research gaps were identified. Research assessing those factors with inconsistent or limited evidence in the current literature was recognized to be a priority for future studies.
Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671211003521.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211064645 - Risk Factors of Shoulder and Elbow Injuries in Baseball: A Scoping Review of 3 Types of Evidence
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211064645 for Risk Factors of Shoulder and Elbow Injuries in Baseball: A Scoping Review of 3 Types of Evidence by Koya Mine, Steve Milanese, Mark A. Jones, Steve Saunders and Ben Onofrio in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgment
The authors thank Mr. Nobuhito Tanpo for contributing to the study-selection process and data extraction.
Final revision submitted August 29, 2021; accepted September 16, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.M.’s work was supported through an Australian Government Research Degrees and Research Training Program (RTP) Scholarship through the University of South Australia. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.