
Abstract
Background:
Achilles tendinopathy is a painful disorder, and various treatment options are available. Bipolar radiofrequency microtenotomy (RFM) has shown promising results in treating tendinosis.
Purpose/Hypothesis:
The purpose was to compare the results between treatment with bipolar RFM and physical therapy (PT) for patients with midportion Achilles tendinopathy. It was hypothesized that RFM would be equivalent or superior to PT.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
A total of 38 patients with midportion Achilles tendinopathy were evaluated for 2 years. The patients were randomized to receive either RFM or PT. There were 20 patients in the RFM group and 18 patients in the PT group. Clinical outcomes were assessed using the visual analog scale (VAS) for pain and the Foot and Ankle Outcome Score (FAOS). The degree of tendinosis was evaluated with magnetic resonance imaging (MRI) of the affected ankle performed before intervention and 2 years after intervention.
Results:
In both groups, the VAS scores at the 2-year follow-up were significantly improved compared with preintervention: from 7.2 ± 1.5 to 1.0 ± 1.4 for the RFM group and from 5.9 ± 1.3 to 3.1 ± 1.8 for the PT group (P < .01 for both). Compared with the PT group, the RFM group had significantly better VAS scores at both the 1- and 2-year follow-ups (P < .01 for both) and better scores on 4 of the 5 FAOS subscales at the 2-year follow-up (P < .01 for all). MRI revealed an improvement in the tendinosis score in both groups, without any significant difference between the groups.
Conclusion:
In this randomized study, the clinical assessments revealed significant improvements in the VAS, FAOS, and tendinosis score as seen on MRI 2 years after intervention with either RFM or PT in patients with midportion Achilles tendinopathy. The improvement was significantly better in the RFM group with regard to VAS and FAOS, but not in the MRI appearance.
Registration:
NCT03274557 (ClinicalTrials.gov identifier).
Chronic midportion Achilles tendinopathy (AT), a painful condition with swelling at the affected site and impaired function, is a common overuse injury in sports involving running and jumping. The incidence of AT in top-level runners is estimated to be 7% to 9%. 27,33 In recreational runners, the lifetime incidence has been reported to be approximately 52% 17 ; however, 30% of patients have a sedentary lifestyle. 39 AT is a nonrupture injury with a multifactorial cause. 23 The pathophysiology is mainly unknown, but the tissue changes seen in histological specimens confirm degenerative changes known as tendinosis. 5 Sensory nerve ingrowth has been observed as a reaction to repetitive loading of the tendon, and with this nerve ingrowth, an increase in the levels of glutamate, calcitonin gene–related peptides, and other substances is also seen. 18,32 It is argued that neovascularization accompanied by sensory neonerves is the pain source. 14 This vasculoneuronal ingrowth causes an increase in pain signaling by producing nociceptive substances such as substance P and the aforementioned glutamate and calcitonin gene–related peptides. 3
Recently, there has been some controversy about the optimal treatment of chronic midportion AT. There are several methods for the treatment of AT, but no particular one is recognized as being superior. In a randomized study, Dedes et al 11 found that extracorporeal shockwave therapy (ESWT) was an effective method for treating various tendinopathies in the plantar fascia, elbow, Achilles tendon, and rotator cuff at a 4-week follow-up. In 90 of 101 patients with AT, Fahlström et al 13 found a significant difference in visual analog scale (VAS) pain scores before and after treatment using eccentric calf-muscle training for 12 weeks. This is in line with Roos et al, 28 who found significant pain reduction after eccentric training in the same type of patients. Sayana and Maffulli 31 studied the effects of physical therapy (PT) with eccentric exercises in sedentary, nonathletic patients; interestingly, they found that 44% of the 34 patients with a clinical diagnosis of AT did not improve with the eccentric exercise regimen.
In a randomized controlled trial (RCT), Alfredson and Ohberg 3 compared injection with either a sclerosing substance or local anesthesia. At 6 months after injection with the sclerosing substance, 8 of 10 tendons were pain-free and without neovascularization as confirmed by ultrasonography. The same improvement was not found in the local anesthesia group. Lind et al, 19 using the same sclerosing method, found that at 2 years there was a significant reduction in VAS and midportion Achilles tendon thickness as seen on ultrasonography.
In general, nonsurgical treatment is not successful in 24% to 44.5% of patients with AT, and surgical treatment is recommended in these patients. 2,27 A systematic review 7 studying the surgical treatment of midportion AT revealed a large variation in surgical techniques. However, each technique consisted of release of the tendon (via adhesiolysis or release or excision of the paratenon), debridement of degenerative tissue, longitudinal tenotomies, or a combination of these. Minimally invasive and endoscopic procedures were found to yield lower complication rates and equivalent patient satisfaction rates when compared with open procedures. None of the included studies compared surgical treatment with nonsurgical treatment or placebo intervention. 7
Bipolar radiofrequency microtenotomy (RFM) is thought to incite a healing response mediated by growth factors 36 and an early inflammatory response with new vessel formation. 35 Takahashi et al 34 have suggested that radiofrequency (RF) induces acute degeneration and/or ablation of sensory nerve fibers, which might explain the early pain relief after RFM for patients with tendinopathy. Bipolar RFM has shown promising results in treating tendinosis of the lateral epicondyle, 24 plantar fascia, patellar and Achilles tendons, 6,21 and shoulder tendons. 1,37 In a nonrandomized study using RFM, Arnal-Burro et al 6 treated 17 Achilles tendons in 13 patients who were active runners and obtained a 94% improvement in symptoms and a return to previous performance in 70% of cases at the 12-month follow-up. In a retrospective study, Yeap et al 40 treated tendinosis in the Achilles, tibialis, and peroneal tendons using RF coblation and found a significant reduction in pain and a significant improvement in function 3 months after surgery.
The aim of the present study was to investigate and compare the clinical and radiological outcomes in patients with chronic midportion AT after treatment with either RFM or PT in an RCT. The hypothesis was that RFM is equivalent or superior to PT for the treatment of patients with AT.
Methods
Study Design
The study was approved by an ethics committee, and all the participants signed informed consent forms before inclusion. The participants in the study were recruited between June 2016 and May 2018 from the University Hospital of North Norway, the largest hospital in northern Norway. Initially, 47 patients were enrolled in the study. The inclusion criteria were pain in the Achilles tendon with a duration of at least 6 months, impaired daily and sports activities, and evidence of tendinosis in the midportion of the Achilles tendon on magnetic resonance imaging (MRI). Patients with previous surgery to the Achilles tendon or severe active organic diseases were excluded. The study was registered at ClinicalTrials.gov (identifier NCT 03274557).
The patients were randomized into 2 groups where they received either RFM or PT, as illustrated in Figure 1. The randomization was administered by the clinical research department at our institution. After the patients signed the consent statement, the senior author (K.M.) called the research department and gave the first 2 letters of the first name and first 2 letters of the surname for anonymous registration of the patients. The randomization was performed using the Microsoft Access program with the Rnd function. Block randomization was used, with a block size varying randomly between 4 and 6.

Flowchart showing the inclusion process in the study. MRI, magnetic resonance imaging.
Four patients in the RFM group declined surgery, while 5 patients allocated to the PT group withdrew from the study and underwent surgery elsewhere (Figure 1). As a result, a total of 38 patients, 21 men and 17 women, with tendinosis in the midportion of the Achilles tendon were followed up for a minimum of 2 years. The right side was affected in 14 patients and the left in 24 patients.
All patients had previously been given nonsteroidal anti-inflammatory drugs (NSAIDs) with a short-term effect. No patient had previously been given injections of corticosteroids around the Achilles tendon. All patients had undergone training programs recommended by a physical therapist without supervision.
Treatment Procedures
RFM treatment
All procedures were carried out on an outpatient basis, and all were performed by the same surgeon (K.M.). The patient was placed in a prone position under local anesthesia and sedation. An incision about 4 cm in length was made slightly medially over the midportion of the affected Achilles tendon to expose the involved part of the tendon. If tenosynovitis was present, it was debrided. The paratenon was incised. A Topaz electrode (ArthroCare) connected to a sterile isotonic saline flow system was used for the microtenotomy. RF apparatus provided the energy through the electrode. The ArthroCare recommendations for use of the device were followed during the procedure. The electrode was placed on the tendon perpendicular to its surface. Next, RF was applied to the tendon in a grid-like pattern, where each stimulated spot was placed 5 mm away from the adjacent spot. Four to 6 light touches were first applied, followed by penetration of the whole depth of the tendon to perform the actual micro-neuroablation. The activation time for the electrode is fixed by the manufacturer at 0.5 seconds. The affected tendon usually required 12 to 20 microablations (Figure 2). The method has previously been described by Meknas et al. 24
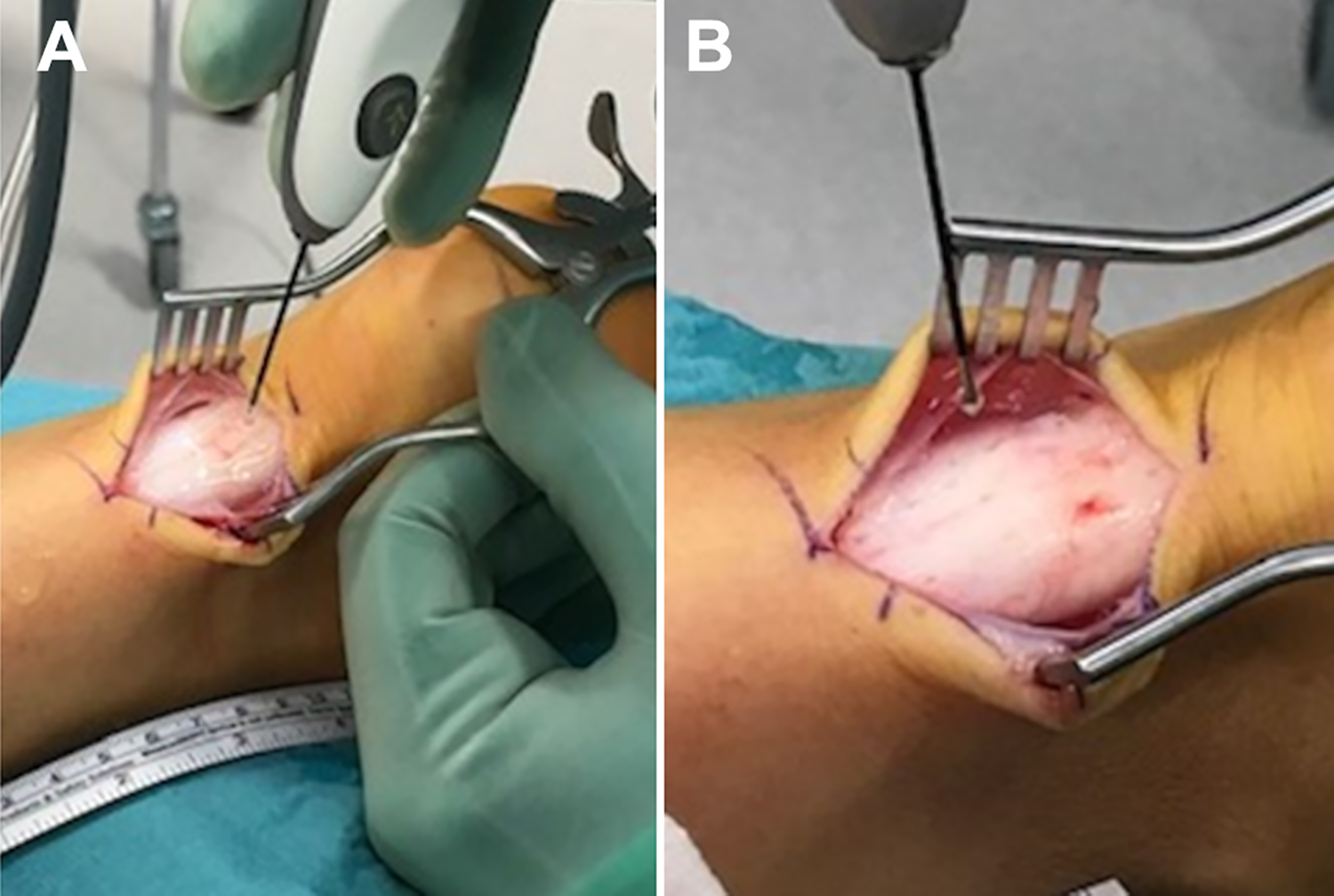
(A) Intraoperative photograph showing the Achilles tendon during microablation using a Topaz microdebrider. (B) Appearance of the tendon after the microtenotomy procedure.
Postoperative rehabilitation
The postoperative rehabilitation protocol included the use of crutches for 2 weeks with a limited weight load. Active-assisted range of motion exercises within the patient’s tolerance were initiated on the first postoperative day. The activity was gradually increased for the next 6 weeks, as tolerated by each patient. Return to sports was permitted by protocol after 3 months.
PT treatment
Patients in the PT treatment group received an eccentric exercise program that was performed every day for 12 weeks. The training protocol used in this study was the eccentric calf-muscle training protocol used in a study by Alfredson et al 4 in 1998. Before initiating treatment, all patients were informed about the intervention and instructed by a physical therapist. In addition, they were given a written manual on how to perform the training and how to progress. Strength exercises were performed twice a day and consisted of 2 eccentric exercises for the ankle plantarflexion muscle group. Each exercise was performed in 3 sets of 15 repetitions. To achieve maximum stretch on the Achilles tendon, the exercises had to be performed standing with the forefoot on the nosing of a stair tread or at the edge of a box to enable the heel to be lowered into a position below that of the forefoot (Figure 3).
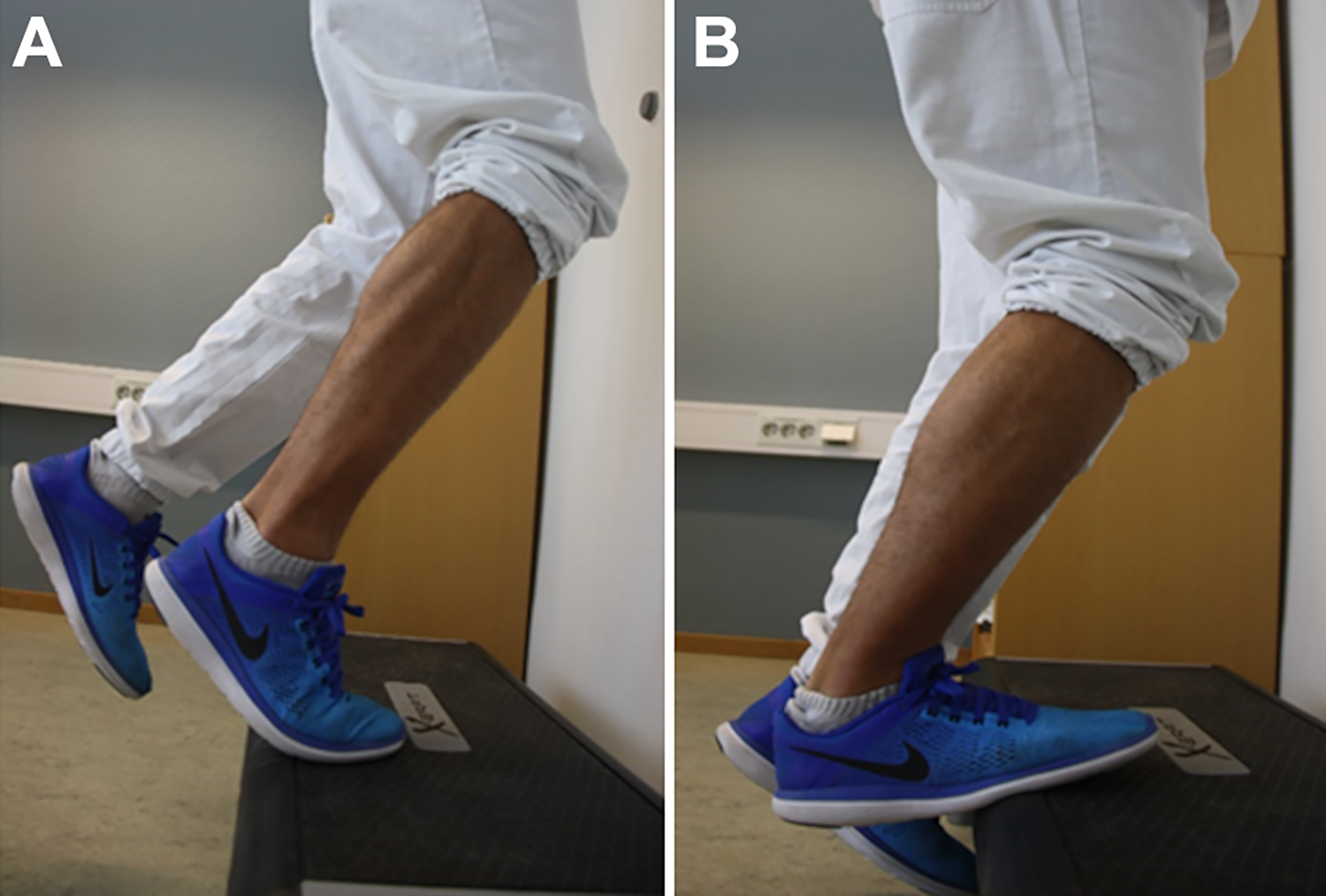
The eccentric exercises in the training program for the ankle plantarflexion muscle group were performed as illustrated: (A) standing on the forefoot with the ankle in plantarflexion and (B) lowering the heel into a position below the forefoot, thus accomplishing an eccentric load on the calf muscles.
The patients were instructed to tolerate some degree of pain during and shortly after training but to avoid loads causing long-standing pain. To begin with, only the body weight was used, alternatively with additional hand support if this was too painful. When the pain during and after training was minimal, the load was increased by wearing a backpack weighing 5 kg. As further progress was made, an increase in the backpack load was made. Patients were instructed to avoid the use of NSAIDs during the training period.
The PT sessions were standardized and supervised by the same physical therapist, and all patients showed good compliance. However, the proceeding of the treatment could vary in time because it was based on the pain experienced by the patients.
Clinical Outcomes
Clinical outcomes were assessed with a physical follow-up at 6 months (data not published), at 1 year after intervention by an independent observer not involved in the study, and at 2 years after intervention. Assessments included the VAS for pain (0-10, where 0 is no pain and 10 maximum pain) and the Foot and Ankle Outcome Score (FAOS) for the evaluation of pain, function, quality of life, and other symptoms. At the 2-year follow-up, all patients received the same 2 rating scales by post to fill out and return. This completed their participation in the study. We used the VAS and FAOS because both are validated as showing acceptable construct validity, reliability, and responsiveness for foot and ankle diseases. 9,15 The primary variable in the study was the VAS for pain.
MRI (Avanto 1.5-T, Siemens) of the affected ankle was carried out on all patients before inclusion to rule out concurrent pathology, such as tumors or osteoarthritis, and to verify the diagnosis of tendinosis in the midportion of the Achilles tendon. At 2-year follow-up, patients underwent MRI assessment using the same machine. Scanning was done using an ankle coil, and the following sequences were utilized: Sagittal T1 turbo spin echo: field of view (FOV) 180 mm, 3-mm slice thickness, pixel size 0.7 × 0.7, repetition time (TR) 494 milliseconds (ms), echo time (TE) 8.2 ms Sagittal proton-density fat-suppressed (PDFS): FOV 180 mm, 3-mm slice thickness, pixel size 0.7 × 0.7, TR 2410 ms, TE 35 ms Axial PDFS: FOV 160 mm, 3-mm slice thickness, pixel size 0.6 × 0.6, TR 2410 ms, TE 35 ms
In total, 34 patients, 17 in each group, underwent MRI examination at the 2-year assessment. The MRI scans were evaluated on both occasions for the presence of tendinosis, rupture, and edema by a blinded radiologist with special interest in musculoskeletal pathology, according to the following scale: 0 = no tendinosis, 1 = minor tendinosis, 2 = moderate tendinosis, and 3 = severe tendinosis. The same scale was used to evaluate edema and rupture. All partial ruptures were classified as intra-tendinous grade 3 tendinosis.
Statistical Analysis
Statistical analyses were carried out using SPSS version 26 (IBM Corp). The data are reported as mean values with standard deviations. The unpaired t test (independent t test) was used to compare the groups, and the paired t test was used to compare the preintervention and the 2-year follow-up within the study groups. The chi-square test was used for a comparison of dichotomous variables. A P value <.05 was considered statistically significant.
In the power analyses, the VAS was the primary variable of the study. A difference of 2 units at 2 years was considered a clinically important difference. 16 If the standard deviation of the variable was 2 units as well, 17 patients would be needed in each group to reach a power of 80%. To increase the power of the study and to tolerate dropouts, the aim was to include 20 patients in each group.
Results
A total of 38 patients were followed up in the study for a minimum of 2 years. Seventeen patients (45%) were active in their spare time; 5 were soccer players, 4 were runners, and 8 performed different kinds of recreational sports activity. The characteristics of the patients are presented in Table 1. No significant differences were found regarding age, sex, or duration of symptoms between the RFM and PT groups before intervention (Table 1).
Characteristics of Patients in the Study Groups a

a Data are presented as mean ± SD or No. of patients. PT, physical therapy; RFM, radiofrequency microtenotomy.
The mean VAS was 7.2 for the RFM group and 5.9 for the PT group before intervention (P < .01). At the 1- and 2-year follow-ups, both groups had achieved a significant improvement in VAS compared with before intervention (Table 2). The RFM group had a significantly lower (ie, better) mean VAS than the PT group at both 1- and 2-year follow-ups.
VAS Pain Scores Between and Within Study Groups Until the 2-Year Follow-up a

a Data are presented as mean ± SD. Bolded P values indicate a statistically significant difference between the variables compared (P < .05). PT, physical therapy; RFM, radiofrequency microtenotomy; VAS, visual analog scale.
There was no significant difference in the FAOS between the RFM and PT groups before intervention. The within-group comparison of the FAOS at the 1- and 2-year follow-ups revealed a significant improvement in the RFM group for all FAOS variables. The corresponding finding was seen only for “symptoms” at 2 years in the PT group (Table 3). At 2 years, a significant difference in FAOS in favor of the RFM group was seen between groups for all variables except sports.
FAOS Between and Within Study Groups a
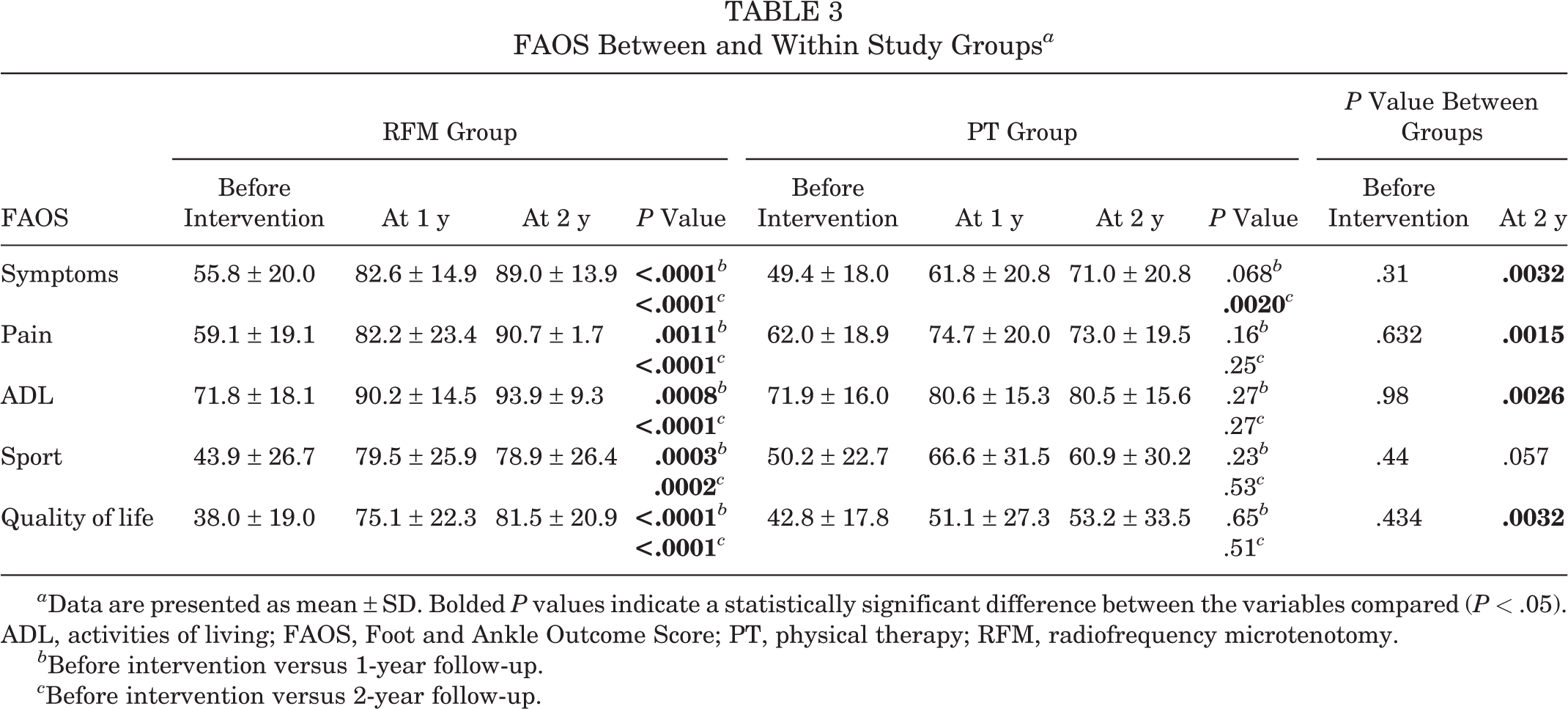
a Data are presented as mean ± SD. Bolded P values indicate a statistically significant difference between the variables compared (P < .05). ADL, activities of living; FAOS, Foot and Ankle Outcome Score; PT, physical therapy; RFM, radiofrequency microtenotomy.
b Before intervention versus 1-year follow-up.
c Before intervention versus 2-year follow-up.
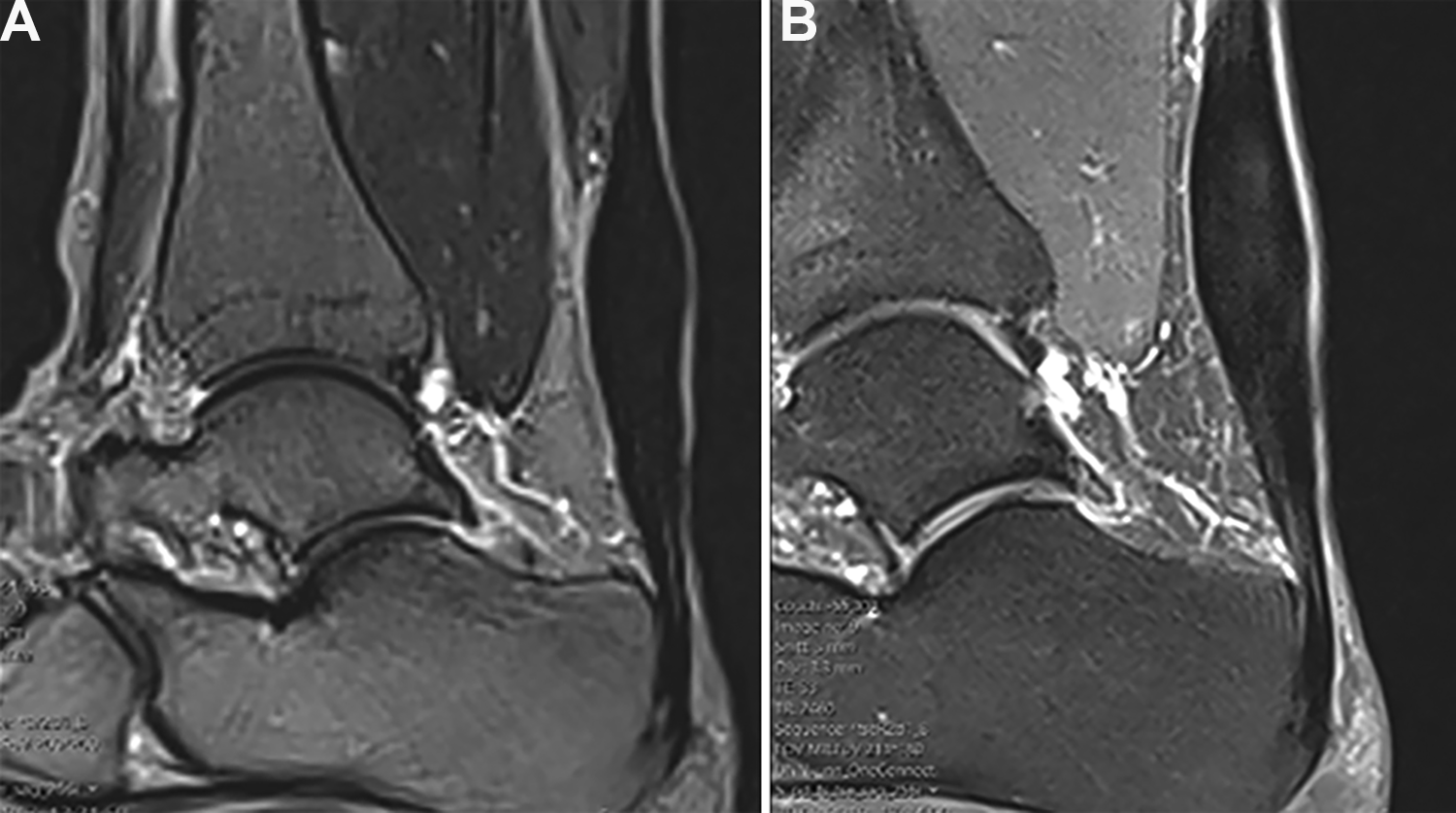
MRI evaluation revealed a significant improvement in tendinosis and edema in the RFM group but not in the PT group. However, no significant difference between the groups could be found, as presented in Table 4. Changes in the occurrence of tendinosis and edema in patients from the RFM and PT groups can be seen on the MRI scans in Figures 4 and 5, respectively.
MRI Evaluation of the Achilles Tendon Before Intervention and After 2 Years a

a Data are presented as mean ± SD. Bolded P values indicate a statistically significant difference between the variables compared (P < .05). PT, physical therapy; RFM, radiofrequency microtenotomy.
b Magnetic resonance imaging (MRI) grading: 0 = no changes, 1 = minor changes, 2 = moderate changes, 3 = severe changes.

Magnetic resonance imaging scans obtained in a 38-year-old male patient in the radiofrequency microtenotomy group (A) before the operation and (B) 2 years after the operation, showing reduced tendinosis from grade 2 to 1 and reduced edema from grade 2 to 0.
Magnetic resonance imaging scans obtained in a 39-year-old female patient in the physical therapy group (A) before intervention and (B) at the 2-year follow-up, showing increased tendinosis and edema from grade 2 to 3.
One patient in the RFM group suffered a postoperative deep vein thrombosis, but no other complications were registered.
Discussion
The most important finding in this study of patients with AT was that at 2 years, there was a significant improvement in the VAS in both the PT and RFM groups. However, there were significantly better results seen in the RFM group compared with the PT group in both the VAS and FAOS.
As mentioned, Dedes et al 11 reported short-term results of ESWT. They found that the method was effective for treating various tendinopathies, including AT, at 4 weeks of follow-up. In another study, Rompe et al 26 found that eccentric loading alone was less effective than a combination of eccentric training and repetitive low-energy shockwave treatment at the 4-month follow-up.
Several studies have investigated platelet-rich plasma (PRP) as a method for treating AT. Among others, de Jonge et al 10 compared PRP with placebo in combination with an eccentric training program. They observed no clinical or ultrasonographic superiority of one treatment over the other after 1 year of follow-up. In another study, 30 60-year-old patients were compared with young and middle-aged patients with AT after treatment with ultrasound-guided PRP injections once a week for 3 weeks. The authors found that PRP treatment produced satisfactory results in young patients with recalcitrant noninsertional AT, reducing pain and improving function, but was less effective in older patients. 30 In a systematic review, Madhi et al 22 suggested promising results from the use of PRP, but they argued that there was a need for more RCTs to produce better, more accurate results. This is in line with the findings of Di Matteo et al, 12 who reported a paucity of high-level literature on the application of PRP in the management of tendinopathy for both the patellar and Achilles tendons. In an RCT, Usuelli et al 38 found that the use of intratendinous, adipose-derived stromal vascular fraction was superior to PRP for the treatment of AT.
Various surgical procedures have been described in the literature, without any evidence to show that one is superior. Ultrasound- and color Doppler–guided tendon scraping and plantaris tendon removal in patients with chronic painful midportion AT showed good clinical outcomes and high satisfaction rates after 5.8 years of follow-up in a recently published study. 29 These findings are in line with those of Calder et al, 8 who found pain reduction and FAOS improvement in 16 patients with AT after plantaris tendon excision. The endoscopic treatment of AT was advocated by Monteagudo et al, 25 who underlined the importance of an appropriate indication and stated that there is still a need for studies with a higher level of evidence.
In a systemic review, Baltes et al 7 argued that minimally invasive and endoscopic procedures have lower complication rates with similar patient satisfaction in comparison with open procedures. However, because of the low methodological quality of the included studies in combination with large heterogeneities in the studied population, the techniques used, and the outcome measurements reported, they refrained from data pooling or recommendations. 7 Using RF coblation, Yeap et al 40 operated on 15 patients for chronic tendinosis of the Achilles, posterior tibial, and peroneal tendons. They achieved good short-term outcomes and pain relief with this method at 6 months of follow-up. The underlying mechanism to explain the effect of RF interventions is that the thermal energy applied to the diseased tendon destroys the newly formed blood vessels together with the sensory nerves that accompany them. 20 Arnal-Burro et al 6 conducted a retrospective case series consisting of 17 Achilles tendon surgical procedures using RFM in 13 patients who were habitual runners with noninsertional AT. The authors found an improvement in 94% of symptoms and a return to the previous activity in 70% of the cases at the 12-month follow-up. This finding is in line with the results of the present study.
In the present randomized study, the treatment options were not mixed, and one group received only PT while the other group received RFM, making the results more coherent. The clinical relevance of the present study is that RFM is a simple, safe, and effective method for treating AT. Our results indicate that although significant improvements were seen with both treatment options, RFM is better than PT for treating midportion AT, and the hypothesis of the study was thus confirmed. We suggest that before considering surgery, patients should undergo supervised PT for at least 6 months. If PT does not yield adequate improvement, treatment with RFM should be considered.
The strengths of this study include the study design, as the RCT is acknowledged as the preferred design for testing treatment options. Upon randomization, there were mostly no significant differences between the RFM and PT groups except for a significantly higher (ie, worse) VAS in the RFM group before intervention. Another strength was that no patients were lost to follow-up. A few patients refused to undergo MRI at the 2-year examination, but they participated in the final scoring evaluation. The fact that the follow-up was made by an independent, blinded observer is an additional strength.
The limitations of the study include the relatively small number of participants and the possibility that it was underpowered despite an appropriate power analysis. A further weakness is that the MRI evaluation that was used lacked a second reviewer evaluation and had not undergone a test-retest procedure. In addition, the significant difference in VAS scores and MRI findings before treatment are other limitations that could introduce bias to the study. A better description on how the patients were able to increase their load during training would also have been useful. For future studies, a longer follow-up time and a larger cohort are recommended.
Conclusion
In this prospective randomized study, the clinical assessments revealed significant improvements in the VAS, FAOS, and tendinosis scores as seen on MRI 2 years after intervention with both RFM and PT in patients with midportion AT. The improvement was significantly better in the RFM group with regard to VAS and FAOS but not in the MRI appearance.
Footnotes
Final revision submitted July 21, 2021; accepted September 3, 2021.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Regional Committee of Research Medical and Health Ethics Sør-Øst (2014/1277).