
Abstract
Background:
Mentorship is a key aspect of leadership development for orthopaedic surgeons, but there are few formalized mentorship programs in medical training. The individualized development plan (IDP) is a tool that potentially improves mentorship opportunities through identifying specific competency deficiencies and facilitating communication with mentors.
Purpose:
To assess the views of prospective orthopaedic surgery sports medicine fellows on the skills necessary for career development and the utility of an IDP for longitudinal career mentorship during a sports medicine fellowship.
Study Design:
Cross-sectional study.
Methods:
Candidates who interviewed for an orthopaedic surgery sports medicine fellowship voluntarily completed an anonymous IDP as well as a survey to assess their perceptions of the IDP tool to define their career goals and its use for longitudinal mentorship. The IDP included quantitative and qualitative responses for the self-assessment of multiple skill domains (general research, teaching, professional, interpersonal, leadership, and management) using a 5-point Likert scale (1 = needs improvement, 5 = highly proficient). Quantitative results were analyzed using analysis of variance and Student t test.
Results:
A total of 25 candidates completed the IDP and survey. The mean ± standard deviation composite score of all skill domains was 3.62 ± 0.91. The candidates’ greatest deficit was in grant writing (2.28 ± 0.94; P < .01), while their greatest strength was getting along with others (4.52 ± 0.65; P < .01). Candidates identified, as short-term goals, obtaining a fellowship training position, completion of research/academic projects, and improvement of surgical skills; their common long-term goals included having a role in an academic institution, professional society, and/or research and innovation environment. The majority of participants agreed that the IDP is a valuable tool to characterize career and personal goals (74%) and facilitate longitudinal fellowship mentorship (83.3%).
Conclusion:
The majority of candidates valued the IDP for their short- and long-term goals. Program implementation of an IDP could be beneficial in allowing trainees to effectively identify areas of weakness and strengths while facilitating efficient communication of these needs to mentors.
Orthopaedic surgeons are the heads of their teams inside and outside the operating room. 33 Well-developed leadership skills are important because they are associated with improved patient outcomes, enhanced learning, and increased team performance. 7,9,17 Additionally, leadership has been identified as a skill that can be developed, as shown in >1000 cadets each year at the United States Military Academy at West Point. 16,20 Modifiable skills, such as initiation of team structure and consideration of team members, have been found to have a greater effect on a leader’s effectiveness, emphasizing that leadership can be developed via training. 5 In today’s current framework of health care, leadership development is essential for the successful management of teams but is sometimes neglected in complex and time-constrained environments. 18 Previously, the assumption was that leadership may be more innate than learned and that superior clinical knowledge is sufficient for a physician to succeed as a leader even with limited leadership training. 27 As such, physicians are often thrust into leadership situations for which they have not been adequately prepared. 11 Previous literature has suggested that mentorship, or relationships with role models who can provide guidance through these difficult situations, is an effective method to develop needed leadership skills. 19,28,29 Not only can such a relationship help medical trainees develop the necessary skills to lead in critical situations but mentorship can also be used to enhance personal and professional development throughout training.
While mentorship has varying definitions throughout the literature, most converge on several recurrent themes. Mentorship generally involves someone who not only will teach, provide support, and supervise a mentee but also serve as an advocate. 12,21 Advocacy is often accomplished via relationships with multiple mentors owing to the various aspects of personal and professional life. 22 Mentorship has been found to have a positive association with markers of academic success, such as number of publications, time allotted for research, and job satisfaction. Mentorship has additionally been associated with a reduction in stress, burnout, and attrition rate in minority groups, such as women. 4,22,24
Despite these positive associations with mentorship, there is a lack of formal and informal mentorship programs for medical and surgical training residencies within the United States. Kibbe et al 13 found that only half of the departments of surgery in the United States have an established mentorship program and just 3% of these mentorship programs receive economic support from their institutions. This disparity of established mentorship programs extends into orthopaedic residencies. Oladeji et al 24 noted that two-thirds of orthopaedic resident physicians had access to some form of mentorship program, despite 95.8% reporting that they believed that mentorship played an important role in their development as residents. Hart et al 10 in 2019 indicated that 61.9% of residents surveyed were satisfied with their mentorship opportunities, a number that has not changed over the past decade from the 61.0% cited by Flint et al 8 in 2009. In addition to increasing the number of mentorship programs, there is an opportunity to use different tools and strategies to formalize and structure mentorship.
Individual development plans (IDPs) have been identified as tools to improve mentorship. 15 IDPs were introduced in 2002, and in 2014 they were required by the US National Institutes of Health (NIH) for all graduate students and postdoctoral fellows with NIH funding. 23,30 The IDP is an instrument that can be used to assess specific competencies, identify skill and knowledge gaps, develop learning strategies, and plan for the pursuit of specific career paths. 26,30,32 IDPs have been associated with an increase in confidence in the knowledge of how to achieve career goals, how to implement a plan to develop strengths, and how to strengthen mentor/mentee relationships. Furthermore, IDPs can be used as a tool to identify and appreciate mentees’ needs and desires early in the mentoring process. However, there is some question whether the IDP has actual utility in career development. 30 Thus, there is a need to further evaluate the use and effectiveness of an IDP to maximize its utility.
The objective of this study was to assess the views of prospective orthopaedic surgery sports medicine fellows on the skills necessary for career development, the utility of an IDP completed before fellowship, and the utility of using an IDP for longitudinal career development during sports medicine fellowship. Our hypothesis was that prospective fellows would view the tool as valuable in defining short- and long-term career goals and facilitating mentorship during fellowship.
Methods
This work was determined exempt from institutional review board approval. Prospective candidates who were being interviewed for an orthopaedic sports medicine fellowship at a tertiary care university center were provided with a voluntary and anonymous IDP. After completion of the IDP, the candidates completed a survey to assess their perceptions and value of the tool. All candidates were informed that participation in this survey was voluntary and the data would not be used in their evaluation for fellowship candidacy. The fellowship admissions committee did not have access to the IDP or the post-IDP survey for fellowship candidacy evaluations, and both of these were completed anonymously.
The IDP from the University of California–San Francisco 31 was adapted for our target study group (Appendix A, available as supplemental material). The IDP contained a quantitative self-assessment based on a 5-point Likert scale (1 = needs improvement, 5 = highly proficient) in the domains of general research skills, teaching skills, professional skills, interpersonal skills, and leadership and management skills. The IDP also included an assessment of the candidates’ current time management in percentile (all activities summing to 100%) for time spent on the following: teaching, training, and mentoring others; research or creative work; patient care; administration and other duties; and personal development. This was followed by qualitative open-ended questions to self-reflect on current career and professional goals and perceived needs and barriers for the development of the following skills: general research, teaching, professional, interpersonal, and leadership and management. These qualitative responses underwent review and thematic analysis by 3 reviewers (D.C.T., N.A.B., and J.W.C.) for interobserver agreement. 14 Any discrepancies were then reconciled among the 3 reviewers.
After the candidates completed their IDPs, they completed a voluntary survey created for this study to assess for history of IDP use and the candidates’ value of the IDP as tool (Appendix B, available as supplemental material). Survey responses were categorized on a 5-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree).
Responses were collected and analyzed via Stata Version 15.1 (StataCorp). A 1-way analysis of variance test was used to assess for differences among the mean scores of all skills on the IDP. The Student t test was then used to compare scores of the individual skill types with the summary composite of all the scores. An alpha of .05 was used to test for statistical significance. A Bonferroni correction was applied to reduce the likelihood of false positives attributed to the number of t tests performed, resulting in an adjusted significance level of .0026. 3,25
Results
Of 26 eligible study participants, 25 (96%) completed the IDP and survey and had their responses analyzed. The candidate who did not participate in this study was unable to attend an in-person interview and instead underwent a video interview. There were 19 men (76%) and 7 women (28%); 6 (25%) had an additional degree other than an MD (PhD, MBA, MS, 31 MPH 5 ). One (4%) completed an IDP during medical school before beginning residency training.
IDP: Candidate Self-assessment and Analysis of Skill Domains
Table 1 shows the results of the self-assessment portion of the IDP. The composite mean ± standard deviation of all 5 domains of skills was 3.62 ± 0.91. Based on our analysis of variance testing (P < .01), there was a statistically significant difference in the mean value for each individual score as seen on Table 1 and the composite skill rating (Table 2). Creativity and developing new research directions (3.32 ± 0.99; P = .11), large group teaching (3.24 ± 0.78; P = .04), and grant writing (2.28 ± 0.94) were identified as the lowest-rated skills, with grant writing being the only one that was statistically significant (P < .01). The highest-rated skills were getting along with others (4.52 ± 0.65; P < .01) and communicating clearly in conversation (4.29 ± 0.62; P < .01).
Individualized Development Plan: Candidate Self-assessment of Skills a

a Graded on a 5-point Likert scale: 1 = needs improvement, 5 = highly proficient. Dash indicates there is no value.
b Bold P values indicate statistically significant difference vs composite score (P < .01, Student t test with Bonferroni correction).
One-way Analysis of Variance Comparing the Mean Values of Each Skill Measured Using the Individualized Development Plan a

a MS, mean square; SS, sum of squares.
General Research Skills
Candidates rated their research skills with a mean of 3.5 (Figure 1), with the highest-rated competency in problem-solving and troubleshooting (3.72 ± 0.76; P = .6). The lowest-rated skill was creativity and developing new research directions (3.32 ± 0.99; P = .11). In the thematic analysis of the qualitative portion of the IDP, the candidates identified that they required improvements in statistics knowledge, team building and management for research endeavors, and grant and manuscript writing to be successful in their careers. To address this deficiency, the majority recommended the following: dedicated time to learning about statistics, dedicated time for networking and mentorship with their senior faculty members, and increased participation in grant and manuscript preparation.

Candidates’ self-assessment of their general research skills.
Teaching Skills
Candidates rated their teaching skills with a mean of 3.55 (Figure 2). The highest-rated skill was one-on-one teaching (3.84 ± 0.9; P = .24), while large group presentation was the lowest-rated skill (3.24 ± 0.78; P = .04). Despite the high rating of competency in one-on-one teaching, candidates indicated in the open-ended questionnaires that they needed improvements in one-on-one teaching in the operating room. Following this theme, they identified needs for greater degrees of feedback and discussion of learning styles and goals, as well as increased experience in large group presentation and teaching. To address these deficiencies, the respondents recommended increased levels of feedback, a greater degree of modeling from senior trainees and faculty members, and greater participation in lectureships for large group teaching.

Candidates’ self-assessment of their teaching skills.
Leadership and Management Skills
Candidates rated their leadership and management skills with a mean of 3.65 (Figure 3). The highest-rated skill was leading and motivating others (3.8 ± 0.71; P = .34), while the lowest-rated skill was budgeting (3.52 ± 0.92; P = .59). In the open-ended responses, the respondents identified deficiencies in time management, budgeting resources, and team/project management. To improve these domains, the respondents recommended improved time management organization and increased mentorship from their senior faculty to gain feedback and advice to model their leadership and management activities.
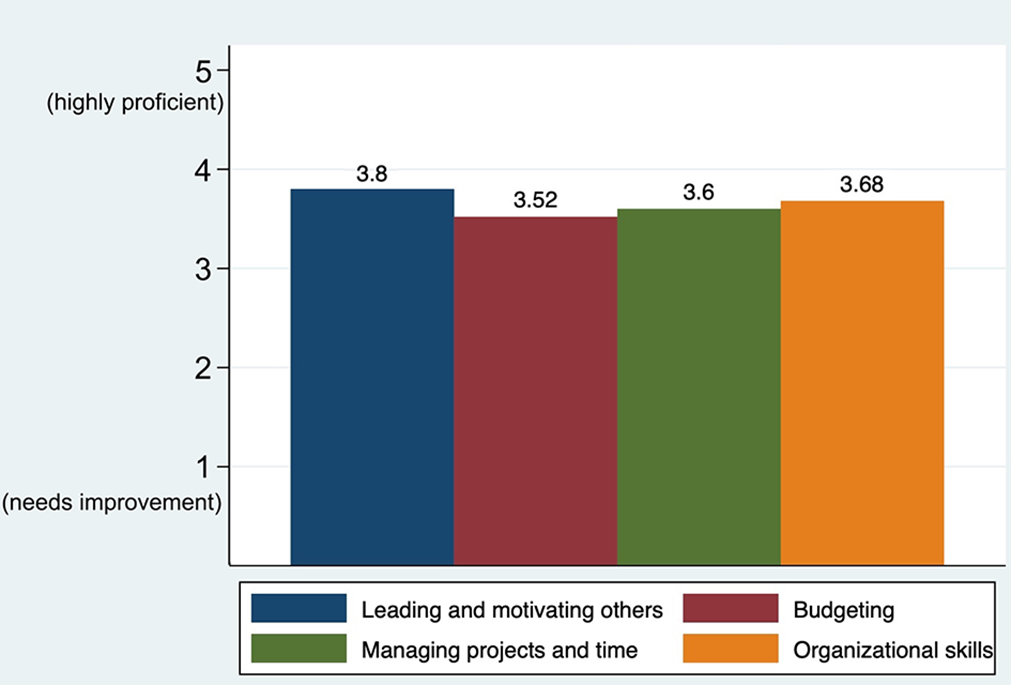
Candidates’ self-assessment of their leadership and management skills.
Professional Skills
Candidates rated their professional skills with a mean of 3.35 (Figure 4). The highest-rated skill in this group was oral presentations (3.72 ± 0.74; P = .6). The lowest-rated skill in this group and in all other skill domains was grant writing (2.28 ± 0.94; P < .01). In the qualitative questionnaires, respondents also identified grant writing as a significant deficiency, followed by public speaking and mentoring others. To improve in this domain, respondents recommended increased participation in grant writing, a greater degree of mentorship from senior faculty, and a greater degree of time preparing for public speaking and oral presentations.
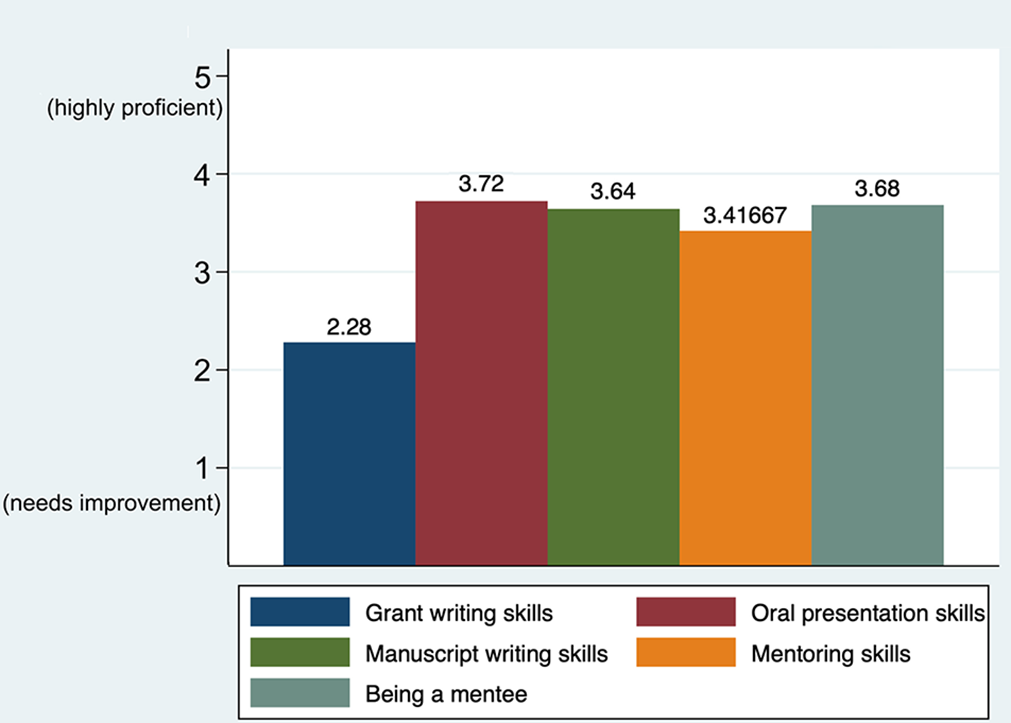
Candidates’ self-assessment of their professional skills.
Interpersonal Skills
Candidates rated their interpersonal skills with a mean of 4.28, which was the highest-rated skill set among all domains (Figure 5). The highest-rated individual skill was getting along with others (4.52 ± 0.65; P < .01), while the lowest-rated skill was communicating clearly in writing (4.04 ± 0.79; P = .03). In the qualitative section, they identified deficiencies in networking and professional social interactions, emotional intelligence for team building, and conflict management. To address these deficiencies, they recommended improvements in communication skills, increased introspection with feedback, and a greater degree of participation in large society/organizational conferences.

Candidates’ self-assessment of their interpersonal skills.
IDP: Assessment of Time Management
The candidates reported that the majority of their time was spent in patient care (62.7%), followed by research and creative work (12.3%) and teaching (9.58%). Administration/other duties and personal development were given the least amount of time (7.36% and 7.42%, respectively).
IDP: Career Goals for Future Focus and Motivations
In the thematic analysis of the open questionnaire, the candidates identified their upcoming goals (in 1 year) as obtaining the next level of training position (fellowship), completion of research and academic projects, and improvement of surgical skills. In terms of long-term career goals (3-5 years), the respondents identified having a role in an academic institution or professional society, having a role with research and innovation, and having successfully completed their fellowship training with proficient surgical skills. The candidates identified the motivators for these goals as follows: interest in self-improvement, desire to contribute to the field of orthopaedics and sports medicine, and dedication to high-level patient care.
Survey: Assessment of the Candidates’ Perceptions and Value of the IDP
Of the 25 candidates, 17 (74%) responded that they agree/strongly agree that the IDP was helpful in characterizing their career and personal goals (6 [26.1%] undecided, 2 nonresponses not included in the analysis). In addition, 16 (66.7%) responded that they agree/strongly agree that it was helpful to complete the IDP before their fellowship interviews (6 [25%] neutral, 2 [8.3%] disagree, 1 nonresponse not included in the analysis). A larger proportion, 20 (83.3%), responded that they agree/strongly agree that the IDP would be helpful to use longitudinally during fellowship to develop their future careers (4 [16.7%] neutral, 0% disagree, 1 nonresponse not included in analysis) (Figure 6).

Candidates’ perceptions of the utility of the individual development plan (IDP) to characterize their career and personal goals and as a tool before their fellowship interview and during fellowship training.
Discussion
The purpose of this study was to evaluate the perceptions and perceived value of an IDP for the self-assessment of professional skills, the characterization of personal deficits, and the identification of future goals and for its role in facilitating longitudinal mentorship during future orthopaedic sports medicine fellowship. Our most important finding was that the majority of fellowship candidates (83.3%) agreed that the IDP was helpful to characterize their personal and career goals and that it would be valuable for longitudinal mentorship during the fellowship year. Given these results, we believe that an IDP could be a useful tool for each institution to understand the needs of a trainee class and identify these needs early in the mentorship process.
The majority of candidates (96%) were deficient in having an experience or exercise similar to our IDP to develop formal career goals and plans, with the exception of 1 candidate completing an IDP in medical school. This result is likely associated with the current lack of funding and with the existence of formal mentorship programs within 30% to 50% of surgical and orthopaedic residency programs. 13,24 The use of this IDP longitudinally would be advantageous to trainees, as it would provide a framework for mentors to understand and promote the trainees’ characterization of personal and career goals and it would help guide subsequent action plans to achieve these short- and long-term goals. As fellowship is a transitional point in career development, mentorship can guide mentees through transitional states in personal development and help them maximize their potential to become successful clinicians. 21 As trainees continue their development, their roles and goals change, highlighting the need for maintaining longitudinal mentorship. 6
Based on the candidates’ self-assessment of skills, creativity and developing new research directions, large group teaching, and grant writing were identified as the lowest-rated skills. The lack of competency in grant writing and large group teaching is important to address, as it may have implications on the identified long-term goals of having a role in an academic institution or professional society and/or a role in research and innovation.
While the specific domains that the participants identified for improvement may not be applicable to all trainees applying for an orthopaedic sports medicine fellowship, the study of the IDP illustrates that it can be utilized as an effective tool to identify areas of weakness for potential intervention during mentorship. Bernstein et al 2 showed that the combination of a clinician-scholar career timeline, mentorship, and successful grant-writing application in the Clinician Scholar Career Development Program can have a positive effect on increased scholarly and career-affecting activities. We believe that the IDP can achieve similar objectives: helping to establish short- and long-term professional and personal goals, providing a longitudinal tool for mentorship during the fellowship training, and including a guided educational experience (eg, completion of a grant or increasing experience in large group teaching formats for our study cohort). Furthermore, the IDP can be a useful tool to identify skills for which trainees believe that their competency is high; thus, mentors can devote less time to these areas and spend more time on the domains in which trainees believe they need the most development.
While each fellowship program is tasked with providing a well-rounded surgical training experience, we would like to emphasize that each incoming class of fellows has its own particular strengths, weaknesses, and personal and professional aspirations. These characteristics of the fellowship class can be described using the IDP and communicated to the fellowship faculty members. With this knowledge, the faculty members can supplement their existing curriculum and tailor the educational experience for the fellowship year to maximize mentorship and growth that go beyond the traditional requirements from the Accreditation Council for Graduate Medical Education, American Orthopaedic Society for Sports Medicine, and Arthroscopic Association of North America. Given that the candidates indicated that the majority of their time was spent on patient care and that the barrier to achieve many of their goals was a lack of dedicated time, it would be reasonable to consider including the IDP and its subsequent action plans into the core curriculum and objectives of a fellowship training experience.
We acknowledge that our sample size was relatively small (N = 25) and may not represent the entire population of sports medicine fellowship candidates; thus, the specific competencies that the participants identified as areas for improvement may not be applicable to all fellowship programs. However, we believe that the most important takeaway from this study is the process of completing an IDP and its utility to medical training programs; this is less affected by sample size than the domains pertaining to areas of improvement. The study was also limited by the inherent sampling bias of surveying candidates who were interviewing for a sports medicine fellowship at an academic tertiary center and may not reflect applicants seeking out alternative experiences, such as private practice, community practice, and rural experiences. However, the candidates in our survey were from a reasonably diverse sex group (28% female) in comparison with active orthopaedic surgery residents (14.7% female). 1
There was the potential for response bias, as candidates may have aligned their responses with the perceived objectives of the fellowship. We acknowledge that applicants may have been more inclined to respond positively to the survey despite its anonymity because they were being interviewed for a position in the fellowship program. We attempted to reduce this response bias by explicitly informing all candidates that the participation in and completion of the IDP and survey were voluntary and not a factor in their potential candidacy at the fellowship interview and that all responses were anonymous. Future studies could mitigate this source of bias by surveying applicants after the sports medicine match to obtain truly voluntary and honest answers. We acknowledge that while the IDP appears to be valued by candidates as a useful tool and endorsed by the NIH, it has not been formally validated in the literature. We currently do not have prospective results from its use and instead look forward to future prospective studies to evaluate its long-term efficacy and develop data to support its validation.
Conclusion
In this study, we identified that sports medicine fellowship candidates value the IDP as a positive tool for mentorship and career/personal development. From our results, we recommend the process of administering an IDP as a useful method for trainees to identify domains of low competency; in our cohort, these included grant writing, large group teaching and public speaking, and creativity and developing new research directions. Via the IDP, these domains may be recognized earlier and communicated to mentors to strengthen the experience of the trainee and increase the value of the mentorship relationship.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211059125 - Use of an Individualized Development Plan to Identify Career Development Needs in Prospective Orthopaedic Sports Medicine Fellows
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211059125 for Use of an Individualized Development Plan to Identify Career Development Needs in Prospective Orthopaedic Sports Medicine Fellows by Jonathan W. Cheah, Grant H. Cabell, Nicholas A. Bonazza and Dean C. Taylor in Orthopaedic Journal of Sports Medicine
Supplemental Material
Supplemental Material, sj-pdf-2-ojs-10.1177_23259671211059125 - Use of an Individualized Development Plan to Identify Career Development Needs in Prospective Orthopaedic Sports Medicine Fellows
Supplemental Material, sj-pdf-2-ojs-10.1177_23259671211059125 for Use of an Individualized Development Plan to Identify Career Development Needs in Prospective Orthopaedic Sports Medicine Fellows by Jonathan W. Cheah, Grant H. Cabell, Nicholas A. Bonazza and Dean C. Taylor in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted June 24, 2021; accepted August 4, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.W.C. has received education payments from Arthrex, DJO, Smith & Nephew, and Wright Medical. N.A.B. has received a grant from Arthrex and education payments from SouthTech Orthopedics. D.C.T. has received consulting fees from DePuy/Medical Device Business Services, royalties from DePuy, and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Duke University (Pro00104600).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.