
Abstract
Background:
There is increased interest in quadriceps autograft anterior cruciate ligament (ACL) reconstruction in the pediatric population.
Purpose:
To evaluate children and adolescents who underwent ACL reconstruction using a quadriceps autograft to determine the properties of the harvested graft and to assess the value of demographic, anthropometric, and magnetic resonance imaging (MRI) measurements in predicting the graft size preoperatively.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A retrospective database search was performed from January 2018 through October 2020 for patients undergoing ACL reconstruction. Patients <18 years old at the time of surgery in whom a quadriceps tendon autograft was used were selected. Demographic data and anthropometric measurements were recorded, and graft measurements were abstracted from the operative notes. Knee MRI scans were reviewed to measure the quadriceps tendon thickness on sagittal cuts. Graft length and diameter were then correlated with anthropometric and radiographic data.
Results:
A total of 169 patients (98 male) were included in the final analysis, with a median age of 15 years (range, 9-17 years). A tendon length ≥65 mm was harvested in 159 (94%) patients. The final graft diameter was 8.4 ± 0.7 mm (mean ± SD; range, 7-11 mm). All patients had a graft diameter ≥7 mm, and 139 (82%) had a diameter ≥8 mm. Preconditioning decreased the graft diameter by a mean 0.67 ± 0.23 mm. Age (P = .04) and quadriceps thickness on MRI (P = .003) were significant predictors of the final graft diameter. An MRI sagittal thickness >6.7 mm was 97.4% sensitive for obtaining a graft ≥8 mm in diameter.
Conclusion:
Our findings suggest that tendon-only quadriceps autograft is a reliable graft source in pediatric ACL reconstruction, yielding a graft diameter ≥8 mm in 82% of pediatric patients. Furthermore, preoperative MRI measurements can be reliably used to predict a graft of adequate diameter in children and adolescents undergoing ACL reconstruction, with a sagittal thickness >6.7 mm being highly predictive of a final graft size ≥8 mm.
Keywords
The incidence of anterior cruciate ligament (ACL) injuries has steadily increased in the pediatric population, which has been postulated to be the result of increased participation in youth sports, sports specialization, and year-round training. 3,15 Controversy still exists regarding the optimal management of pediatric ACL reconstruction. However, innovations in surgical techniques and poor outcomes of nonoperative management, including the high risk of early chondral damage, have resulted in a substantial increase in the rate of ACL reconstruction in this population. 12,21 Currently, patients <20 years old are the largest emerging subset of patients undergoing ACL reconstruction. 15
Despite the generally favorable outcomes, complications after ACL reconstruction in children and adolescents are more common than in adults. ACL retear is the most common complication, with an incidence of 10% to 15%, much higher than the 4.4% rate seen in adults. 9,10,21,29 Several contributing factors have been postulated and explored, such as tunnel position, fixation type, rehabilitation techniques, and time to return to sports. However, graft properties seem to be significant predictors of ACL retear, with a graft diameter <8 mm making retear more likely when using a hamstring autograft. 14,16,22
While there are several available graft sources in adults, the options are limited in children. Allograft has been shown to yield inferior results and is thus thought to be a less-than-ideal choice in the active young athlete. 28 Bone–patellar tendon–bone grafts are also discouraged because of the risk of physeal injury at the donor site, as well as the risks associated with placement of a bone plug across an open physis. Therefore, hamstring autografts have been the mainstay graft choice in the pediatric population. However, hamstrings occasionally yield a small graft, which may result in an increased risk of retear. Although allograft augmentation has been proposed to address the deficiency in these cases, augmentation does not necessarily decrease the risk for reinjury, 18,27,28 and there are studies showing an increased risk of graft failure with allograft augmentation. 19 Attempts have been made to predict the hamstring graft size based on demographic, anthropometric, and radiologic measurements (mainly magnetic resonance imaging [MRI] and ultrasound). 1,4,5,7,24 Preoperative prediction of the graft size allows the surgeon to plan for a potentially inadequate graft, by choosing an alternative graft source or augmenting the available graft.
At our institution, quadriceps autograft has increasingly been used as a graft source for pediatric ACL reconstruction. The goal of this study was to evaluate children and adolescents who underwent ACL reconstruction using a quadriceps autograft at a single institution over the past 3 years to determine the properties of the harvested graft and to assess the value of demographic, anthropometric, and MRI measurements in predicting the graft size preoperatively.
Methods
This study was approved by our institutional review board and was performed in compliance with HIPAA (Health Insurance Portability and Accountability Act) regulations and with a waiver of informed consent. A retrospective review was conducted of all patients who underwent ACL reconstruction at our tertiary care children’s hospital between January 1, 2018, and October 31, 2020, through a database query with Current Procedural Terminology code 29888. Patients aged ≥18 years at the time of surgery were excluded, as well as patients with no available preoperative MRI or with operative notes that failed to report graft characteristics. Charts were reviewed by a fellowship trained pediatric orthopaedic surgeon (S.B.) to determine the type of graft utilized for ACL reconstruction. Patients who underwent ACL reconstruction with a quadriceps autograft were then selected. Demographic and anthropometric data (weight, height, body mass index) on the day of surgery were extracted from the electronic medical record.
Operative notes were reviewed to abstract graft harvest technique and graft dimensions. The length of the harvested graft, the graft diameter after stitching but before conditioning, and the graft diameter after tensioning and circumferential preconditioning were recorded. Graft diameter was defined by the mean value of each end of the graft after preconditioning. The ACL reconstruction technique and the fixation method were also extracted. Operative notes were thoroughly reviewed to look for any complications related to graft harvesting or if the surgeon had to resort to another graft source intraoperatively. Preoperative MRI scans were reviewed, and the sagittal thickness of the quadriceps tendon was measured on sagittal T1-weighted or proton density sequences 1 cm above the patella. Midpatellar cuts were selected to measure the tendon’s sagittal thickness where it was the largest (Figure 1). After standardization of the measurement technique, 2 authors (S.B., D.P.V.) performed all the measurements independently to evaluate the interrater reliability, and the mean measurement was used for the subsequent statistical analyses.

Preoperative knee sagittal proton density–weighted magnetic resonance image of a 13-year-old boy with anterior cruciate ligament tear. Quadriceps tendon sagittal thickness was measured 1 cm above the patella (red line). The 3 layers of the quadriceps tendon (vastus medialis/lateralis, rectus, intermedius) are also visible in this image.
Surgical Technique: Quadriceps Tendon Graft Harvest and Preparation
All surgeons utilized a similar quadriceps graft-harvesting technique. A 3- to 4-cm longitudinal incision was made starting just above the proximal pole of the patellar. Dissection continued through the subcutaneous tissues overlying the quadriceps tendon. The paratenon was incised longitudinally. The distal extent of the quadriceps tendon was identified, and the tendon length was provisionally assessed. A 10-mm double-blade tendon stripper (Arthrex) was used to incise the central third of the quadriceps over the planned harvesting trajectory. The distal end of the tendon was elevated from the superior pole of the patella and whipstitched. If tendon length was of concern, a 1-cm sleeve of the periosteum of the proximal pole of the patella could be included in the harvest to yield a longer graft. The underside of the graft harvest was completed with a curved osteotome or a quadriceps tendon stripper-cutter (Arthrex). Depending on the surgeon’s preference, a thin partial-thickness portion of the undersurface of the tendon was left intact to preserve the deep quadriceps fibers and integrity of the capsule, although only full-thickness grafts were included in this study for evaluating the correlation between imaging and intraoperative findings.
The stripper-cutter was advanced to the proximal aspect of the planned graft, which was measured and cut to an appropriate length. A 65- to 70-mm graft is ideal for transphyseal and hybrid reconstruction techniques, while 55 to 60 mm is preferred for all-epiphyseal techniques. Violations of the joint capsule are not uncommon and can be repaired with absorbable sutures. Reapproximating the medial and lateral portions of the quadriceps is not necessary and is not performed at our institution regardless of the technique (partial vs full-thickness graft), but the paratenon was closed with sutures. The incision was kept open to monitor for fluid extravasation during the rest of the procedure, with additional capsular closure performed as necessary. Graft preparation and the attachment of cortical suspensory fixation were performed on both ends with no sutures or augments in the middle portion (Figure 2). (A video of the technique is available on the Pediatric Orthopaedic Society of North America website. 20 )
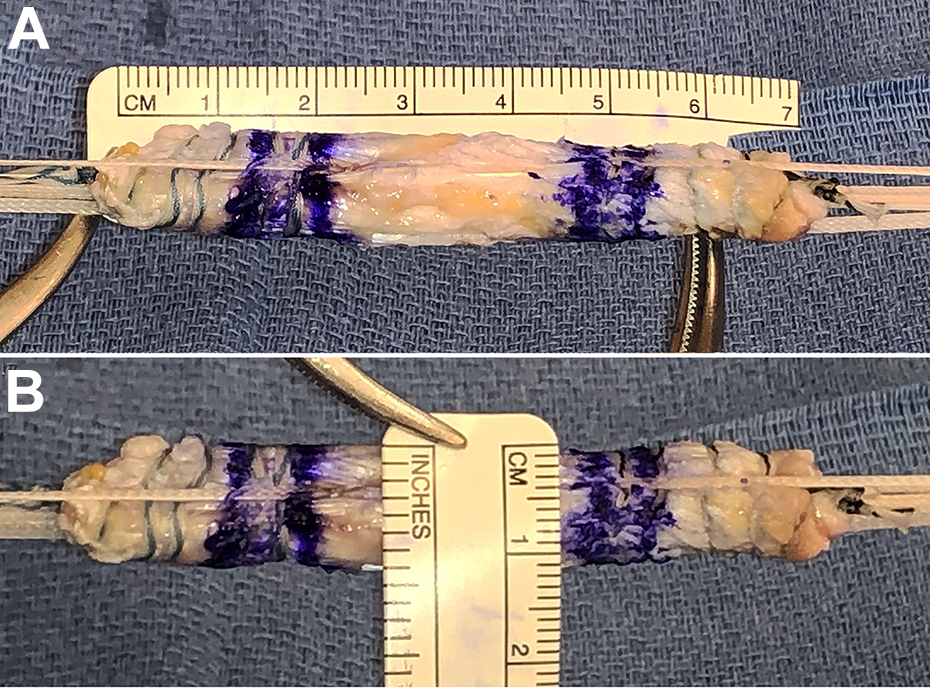
Quadriceps autograft prepared with suspensory fixation on both ends. Typical quadriceps graft (A) length and (B) thickness. A surgical marker indicates the intra-articular and intratunnel portions of the graft.
After graft preparation and mounting on the standard board, grafts were held under 20 lb (89 N) of tension. Furthermore, circumferential compression was applied using the sizing block with the smallest size that would accommodate the graft. Graft size was measured before and after graft tensioning and compression. The mean diameter ([proximal + distal]/2) was used in cases where the proximal and distal ends of the graft differed in diameter.
Statistical Analysis
Intraclass correlation coefficient (ICC) analysis was performed to determine the interrater reliability of MRI measurements. ICC estimates were calculated using a 2-way random-effects model and were interpreted and reported according to Cicchetti 6 : <0.40, poor reliability; 0.40-0.59, fair; 0.60-0.74, good, and >0.75, excellent. Continuous variables are presented as mean and standard deviation or median and interquartile range, and categorical variables are presented as counts and percentages.
The Student t test was used to compare means when data were normally distributed, and the Mann-Whitney U test was used with nonparametric data. Pairwise Student t tests were used to compare pre- to postoperative changes in graft size. Univariable and multivariable logistic regression models were used to determine the predictors of an adequately sized graft. Also, a multivariable linear regression model was used to detect the correlation between graft size and demographic, anthropometric, and imaging variables. Statistical analysis was performed using SPSS Statistics for Windows (Version 26.0; IBM Corp), with a 2-tailed P < .05 considered statistically significant.
Results
During the study period, 406 patients underwent ACL reconstruction at our institution (Figure 3). A total of 169 patients (98 male; 58%) received a quadriceps autograft and satisfied our inclusion criteria, with a median age of 15 years (range, 9-17). The patients weighed 68.4 ± 18.2 kg (mean ± SD; range, 28.8-134.6) with a height of 168.7 ± 10.5 cm (range, 133.9-198.8) and body mass index of 23.8 ± 4.9 kg/m2 (range, 14.5-42.5). While none of the patients were underweight, 30 (18%) were overweight, and 35 (21%) were obese.

Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) diagram illustrating the patient selection process. ACL, anterior cruciate ligament; BPTB, bone–patellar tendon–bone; ITB, iliotibial band; MRI, magnetic resonance imaging.
A graft length ≥65 mm was obtained in 159 (94%) patients. Only 1 patient—the youngest in this series, a 9-year-old male—had a graft <60 mm in length. The majority of grafts were 70 mm in length (125 patients; 74%). A linear regression model established that age and height were significant predictors of graft length and accounted for 18.3% of explained variability in graft length (F 2,166 = 18.6; P < .001).
Regression equation: graft length = 47.01 + (age × 0.36) + (height × 0.10).
The initial diameter of the prepared graft before circumferential preconditioning was reported for 114 cases: 8.9 ± 0.6 mm (range, 8-10.5 mm). The diameter of the graft decreased significantly (P < .001) by 0.67 ± 0.23 mm (range, 0.25-1 mm) after circumferential preconditioning. The final graft diameter was 8.4 ± 0.7 mm (range, 7-11 mm; interquartile range, 8-9 mm), with 139 patients (82%) having a graft diameter ≥8 mm.
The majority of patients receiving quadriceps tendon autograft underwent a transphyseal ACL reconstruction technique (141 patients; 84%), followed by a hybrid ACL reconstruction technique using a transphyseal tibial tunnel and intraepiphyseal femoral tunnel (19 patients; 11%) and finally an all-epiphyseal ACL reconstruction (9 patients; 5%). Patients who had an all-epiphyseal or hybrid technique were significantly younger (12.5 vs 15.2 years; P < .001) and had a shorter graft length (66.25 ± 4.39 vs 69.87 ± 2.97 mm; P < .001). However, the final graft diameter was not significantly different between groups (8.30 ± 0.65 vs 8.47 ± 0.73; P = .23).
We found excellent interrater reliability for MRI measurements, with an ICC of 0.85 (95% CI, 0.80-0.89). The mean quadriceps tendon sagittal thickness on MRI was 7.2 ± 1.0 mm (range, 4.3-10 mm). In a stepwise linear regression model, among the demographic, anthropometric, and radiographic parameters, just the patient’s height was significantly correlated with the graft length (P < .001). In a multivariate logistic regression model, quadriceps tendon thickness on sagittal images (P = .003) and age (P = .04) were significant predictors of a final graft diameter ≥8 mm (Table 1, Figures 4 and 5). Furthermore, a quadriceps tendon sagittal thickness >6.7 mm on MRI was 97.4% sensitive and 46.6% specific in predicting a final graft diameter ≥8 mm.
Univariate and Multivariate Logistic Regression Models Predicting a Final Graft Diameter ≥8 mm a

a Significant predictors are indicated in bold. BMI, body mass index; MRI, magnetic resonance imaging.
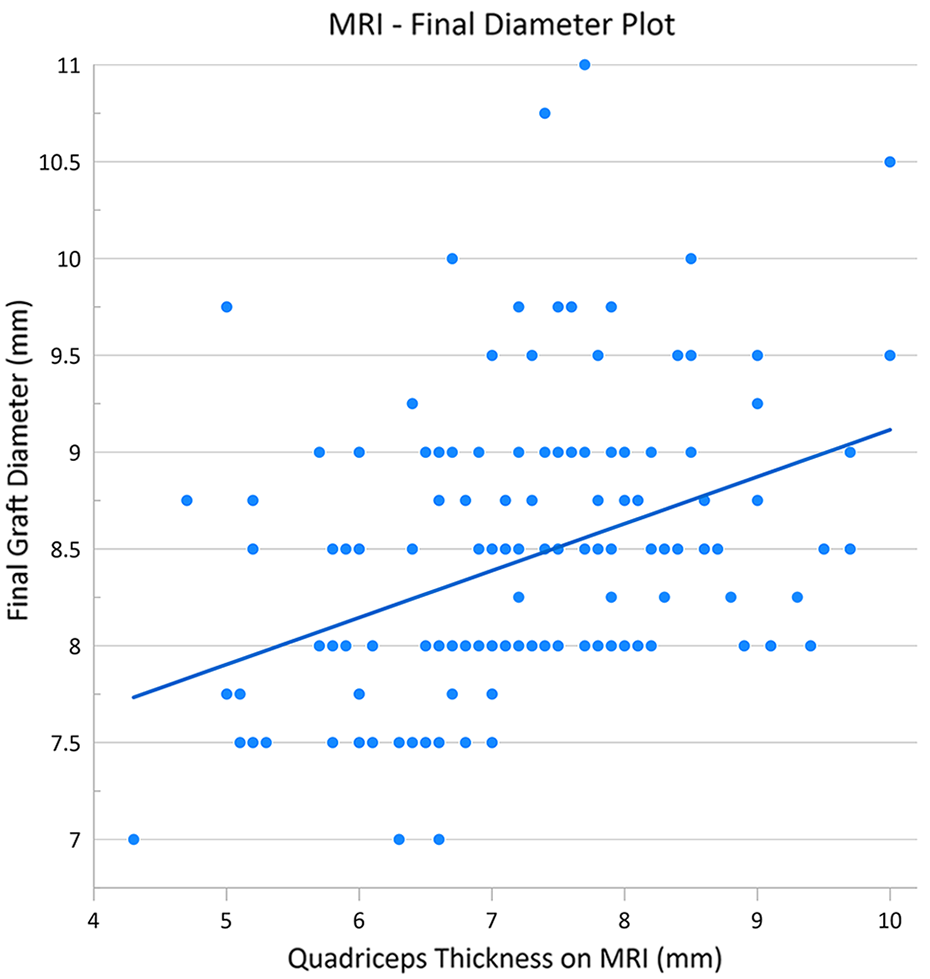
Scatter plot illustrating the correlation between quadriceps thickness as measured on magnetic resonance imaging (MRI) and final graft diameter, with the line of best fit.

Scatter plot illustrating the correlation between age and final graft diameter, with the line of best fit.
No intraoperative complications were recorded during quadriceps graft harvest. Additionally, surgeons did not resort to an alternative graft source because of inadequate quadriceps graft size in any of the patients.
Discussion
The aim of this study was to evaluate children and adolescents undergoing ACL reconstruction at a single children’s hospital to determine the properties of the obtained graft and to evaluate the predictive value of demographic, anthropometric, and MRI measurements. We found that in patients <18 years old, a graft diameter ≥7 mm was achieved in all patients, and 82% of the harvested grafts had a diameter ≥8 mm. Furthermore, 97.4% of the patients with a sagittal quadriceps tendon thickness >6.7 mm on preoperative MRI had a final graft diameter ≥8 mm.
Hamstring autograft has traditionally been the most common graft source for ACL reconstruction in the pediatric population. In a systematic review, 64.4% of the ACL reconstructions in patients <18 years old were performed using a hamstring tendon autograft. 13 A major drawback to hamstring tendon autografts is their significant variability in size, which often results in grafts of insufficient size. Hamstrings might also be transected prematurely during graft harvest. Facing a smaller-than-anticipated graft, the surgeon has 2 options: increase the number of graft strands by folding the graft more 11,17,26 or augment the graft with an allograft; however, both options have disadvantages. Increasing graft strands is not always feasible while retaining adequate graft length for bony integration, and allograft augmentation is still associated with a greater risk of rerupture, even though it yields a larger graft. 18
Considering the growing evidence that autograft size is significantly correlated with the risk of graft failure, 7,9,10,14,16 several studies have investigated the prediction of hamstring tendon autograft size using demographic, anthropometric, and imaging variables. 1,2,5,7,24,25,31 Imaging, in the form of preoperative ultrasound or MRI, has been correlated with the intraoperative graft size, with varying performance, although available studies are largely restricted to the adult population. 32 Todd et al 23 measured quadriceps tendon length and thickness on ultrasound in children aged 4 to 16 years with an intact ACL and found that all had tendons of sufficient size for ACL reconstruction. We sought to evaluate the performance of demographic, anthropometric, and MRI measurements in the prediction of quadriceps tendon autograft size in pediatric patients undergoing ACL reconstruction at our institution. We found that a graft >7 mm was available in all patients, even as young as 9 years. Furthermore, in 82% of patients, a graft ≥8 mm was obtained.
Much of the existing literature on hamstring autografts suggests that patients with grafts <8 mm have an increased risk of retear. 7,16 Our findings suggest that preoperatively, MRI could be reliably used to predict the final quadriceps graft diameter, with a sagittal tendon thickness >6.7 mm being 97.4% sensitive for obtaining a graft size ≥8 mm. Furthermore, while we used a 10-mm graft harvester for all patients, a wider harvester could be used to achieve a larger graft if preoperative MRI is predictive of a graft of insufficient size. It should be emphasized that the 8-mm cutoff for the risk of ACL graft retear is derived from hamstring data exclusively. Data are scarce on quadriceps autograft given the recency of its use, and future studies might determine a different graft diameter cutoff for the risk of retear for quadriceps autograft.
Previous studies have found significant correlations between the patient’s age and anthropometric measures (height and weight) and the final graft size. 5,24 Preoperative prediction of graft adequacy is more important in patients who are scheduled to undergo an all-epiphyseal or hybrid ACL reconstruction, as they are younger and may conceivably not have an autograft of sufficient size. Interestingly, we found that the final graft diameter was similar in patients who received all-epiphyseal/hybrid techniques as compared with the adult-type transphyseal technique, and the mean graft length was 3 mm shorter, which, although statistically significant, is not a clinically important finding. Therefore, quadriceps autograft may even be more desirable in this younger subset of patients in whom hamstring autografts are more likely to be of insufficient size.
We demonstrated that the graft diameter decreases by a mean 0.67 mm after circumferential preconditioning and tensioning. While this is not commonly reported in the literature, it is important, as it may relate to the biomechanical properties of the graft. In a cadaveric study, Cruz et al 8 found that hamstring graft diameter decreased by almost 1 mm after application of tensioning and circumferential compression. A similar effect was recently observed in a multicenter study of hamstring graft preparation during ACL reconstruction. 30 In our study, we observed a smaller change in graft size, which suggests different compressibility of the quadriceps autografts as compared with hamstrings. Future studies may elucidate the tissue creep and tensile strength in quadriceps autografts and their clinical implications in patient outcomes and the risk of graft failure.
We acknowledge several limitations to this study. First, unlike hamstring grafts, which can be folded over a fixation point, quadriceps grafts have to be stitched to apply the fixation points, and the stitching may affect the graft size irrespective of the cross-sectional volume of the graft. Slight variability in stitching technique may also affect the final prepared graft size. While this is a theoretical concern, all of the surgeons had similar preparation techniques. Another potential weakness is that we included only patients <18 years old, so these data may not necessarily apply to older patients. Finally, we did not evaluate the graft failure rate in this patient cohort or include patient-reported outcomes, as they were not the goals of the study. Future studies are under investigation to elucidate the long-term function of patients treated with quadriceps autograft and their comparison with autograft hamstrings.
Conclusion
The findings of this study suggest that tendon-only quadriceps autograft is a reliable graft source in pediatric ACL reconstruction, providing a graft of adequate size in patients as young as 9 years old and yielding a graft diameter ≥8 mm in 82% of pediatric patients. Our data suggest that on preoperative sagittal MRI, a quadriceps tendon thickness >6.7 mm is highly predictive of a final graft diameter ≥8 mm.
Footnotes
Final revision submitted August 19, 2021; accepted August 25, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.A.W. has received education payments from Arthrex and hospitality payments from K2 M. J.T.R.L. has received education payments from Arthrex and royalties from Sawbones/Pacific Research Laboratories. K.J.M. has received education payments from Arthrex and Smith & Nephew. L.W. has received speaking fees from Synthes GmbH. T.J.G. has received research support from AlloSource, Arthrex, and Vericel and education payments from Arthrex and is a paid associate editor for The American Journal of Sports Medicine. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Children’s Hospital of Philadelphia (reference 15-012614).