
Abstract
Background:
In cases of multiple ligaments or medial collateral ligament (MCL) reconstruction, restoring the native anatomy of the posterior oblique ligament (POL) to address chronic valgus instability has been attracting increased attention.
Purpose:
To review the current literature on postoperative outcomes, complications, and return to sports after superficial MCL-POL (sMCL-POL) reconstruction to restore medial knee integrity.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was conducted based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Two independent reviewers searched the PubMed, Scopus, Embase, and Cochrane Library databases using the terms “posterior oblique ligament,” “posteromedial corner of the knee,” and “reconstruction.” Included were studies that reported postoperative clinical and functional outcomes in patients who had undergone a combined sMCL-POL reconstruction for medial knee instability. The authors evaluated surgical technique, rehabilitation protocol, postoperative outcomes (Lysholm, International Knee Documentation Committee [IKDC], and Tegner scores and valgus stress radiograph), and return to sports and complication rates across the included studies.
Results:
A total of 6 studies were reviewed. The cohort consisted of 199 patients (121 men and 78 women), with a mean age of 32.7 ± 3.9 years (range, 27.4-36.6 years). The Lysholm and IKDC scores improved from pre- to postoperatively (Lysholm, from 67.2 ± 20.4 to 89.4 ± 3; IKDC, from 45.8 ± 2.1 to 84.8 ± 7.5). The Tegner score produced satisfactory results, from a preoperative mean of 3.3 ± 2.4 to 6.3 ± 0.9 postoperatively. The medial joint opening on valgus stress radiographs ranged from 7.5 ± 1.1 mm preoperatively to 3 ± 3.1 mm postoperatively. After passing activity-specific functional and clinical tests, 88% to 91.3% of the patients were reported to have returned to recreational sports within 6 to 12 months postoperatively, whereas 10% of the patients developed postoperative complications.
Conclusion:
Satisfactory clinical and functional outcomes, a high rate of return to recreational sports, and a low rate of postoperative complications were reported after an sMCL-POL reconstruction to restore medial knee integrity.
Injuries to the posterior oblique ligament (POL) of the knee are common among high-energy multiligament knee injuries. 18 It was reported that in a cohort of patients treated surgically for grade 3 medial collateral ligament (MCL) injuries, 22 an associated POL injury occurred in 99% of the cases. 22
Biomechanical studies 3 demonstrate that the POL is the primary restraint to internal rotation and prevents valgus and external rotation when knee flexion is between 0° and 30°. On the other hand, the superficial MCL (sMCL) contributes 78% of the stability in valgus and external rotation at 25° of knee flexion. 3 Therefore, a combined injury of the POL and sMCL could result in a clinically significant valgus and anteromedial rotational instability (AMRI). Although the sMCL has high healing potential in grade 1 and 2 injuries, 8,11 in grade 3, when the POL and/or cruciate ligament are compromised and the capacity to heal is poor, repairing the sMCL and POL simultaneously can efficiently restore native valgus and rotatory stability of the knee joint. 1,2 Surgical treatment of the sMCL without any repair or reconstruction of the POL has been reported to lead to inferior outcomes in terms of failing to achieve valgus and rotational stability. 2,10,22 A combined cruciate ligament and sMCL-POL reconstruction reduces late AMRI and chronic valgus instability of the knee and stress on the cruciate ligament graft. 9,14,25
Several surgical techniques have been described to restore the anatomy of the sMCL-POL. 4,7,16 Several studies have evaluated the efficacy of sMCL-POL reconstruction, 12 –15,24,25 reporting satisfactory results in terms of the clinical outcomes associated with a decreased laxity. 12 –14
This study aimed to systematically evaluate the existing literature to account for the clinical, functional, and radiological outcomes, complications, and rate of return to sports among patients treated with a combined sMCL-POL reconstruction after grade 3 MCL injuries that are isolated or associated with knee ligament injuries. We hypothesized that this procedure yields good results in terms of valgus laxity, functional patient-reported outcomes, and the rate of return to sports when used to treat medial knee laxity.
Methods
The current systematic review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 17 and was registered in the Research Registry (reviewregistry1031; www.researchregistry.com).
Eligibility Criteria
The literature selected for this study was based on the criteria detailed below.
Study Designs
Studies conducted using randomized controlled trials, controlled (nonrandomized) clinical trials, prospective and retrospective comparative cohort studies, case-control studies, and case series were included in the current study. Case reports and case series that did not report data on clinical and functional results were excluded.
Participants
Studies conducted on skeletally mature patients who underwent sMCL-POL reconstruction to treat grade 3 MCL and/or associated multiligamentous injuries and who were evaluated for a minimum follow-up of 1 year were considered eligible for the current study.
Interventions
Studies that reported data on clinical, functional, and radiological outcomes after the sMCL-POL reconstruction, isolated or associated with a knee ligamentous surgery, to treat medial knee laxity were considered eligible for the current study.
Types of Outcome Measures
The outcome measures extracted from the studies were the Lysholm score, International Knee Documentation Committee (IKDC) subjective and objective scores, Tegner activity score, rate of return to sports, and rate of complications. The data from studies using stress radiographs to perform a quantitative assessment of the preoperative and postoperative medial stability were also extracted.
Information Sources and Search
A systematic search for relevant literature was performed on the PubMed (MEDLINE), Scopus, Embase, and Cochrane Library databases in October 2020. The publication date was not considered an inclusion criterion. Two independent reviewers (R.D. and K.C.) assisted in conducting and validating the search. The following search terms were entered in the title, abstract, and keyword fields: “posterior oblique ligament” OR “posteromedial corner of the knee” AND “reconstruction.” Only papers published in English were included.
Data Collection and Analysis
Study Selection
The retrieved articles were first screened by title and, if found relevant, then screened further by reading the abstract. After excluding studies not meeting the eligibility criteria, the entire content of the remaining articles was evaluated for eligibility. To minimize the risk of bias, the authors reviewed and discussed all the selected articles, references, and articles excluded from the study. In case of any disagreement between the reviewers, the senior investigator (S.C.) made the final decision. At the end of the process, further studies that might have been missed were manually searched for by going through the reference lists of the included studies and relevant systematic reviews.
Data Collection Process
The data were extracted from the selected articles by the first 2 authors using a computerized tool created with Microsoft Access (Version 2010; Microsoft). Every article was validated again by the first author before analysis. For each study, we extracted the data regarding the patients (age, sex, duration between injury and surgery, and follow-up evaluation), their injuries (type, origin, and associated injuries), surgical technique (type of graft used, number of bundles, fixation technique, number of femoral and tibial tunnels, and tensioning protocol of the POL), rehabilitation protocol, postoperative outcomes (Lysholm, IKDC, and Tegner scores and valgus stress radiographs), rate of complications, and rate of return to sports.
Level of Evidence
The Oxford Levels of Evidence set by the Oxford Centre for Evidence-Based Medicine were used to categorize the level of evidence. 19
Evaluation of the Quality of Studies
The quality of the selected studies was evaluated using the Methodological Index for Non-Randomized Studies (MINORS) score. 23 The checklist included 12 items, of which the last 4 were specific to comparative studies. Each item was given a score of 0 to 2 points. The ideal score was set at 16 points for noncomparative studies and 24 for comparative studies.
Results
Search Results
The electronic search yielded 4654 studies. After 4463 duplications were removed, 191 studies remained, of which 156 were excluded after reviewing the abstracts, bringing the number down to 35. An additional 29 articles were excluded based on the aforementioned inclusion and exclusion criteria. No additional studies were found by manually searching the reference lists of the selected articles. This left 6 studies for analysis. Figure 1 shows the flowchart depicting the selection process for studies. The studies analyzed had a mean MINORS score of 13.1 (range, 12-14), which confirmed the methodological quality of the available literature (Table 1).

PRISMA flowchart showing the selection process for studies included. POL, posterior oblique ligament.
Characteristics of the Selected Studies a
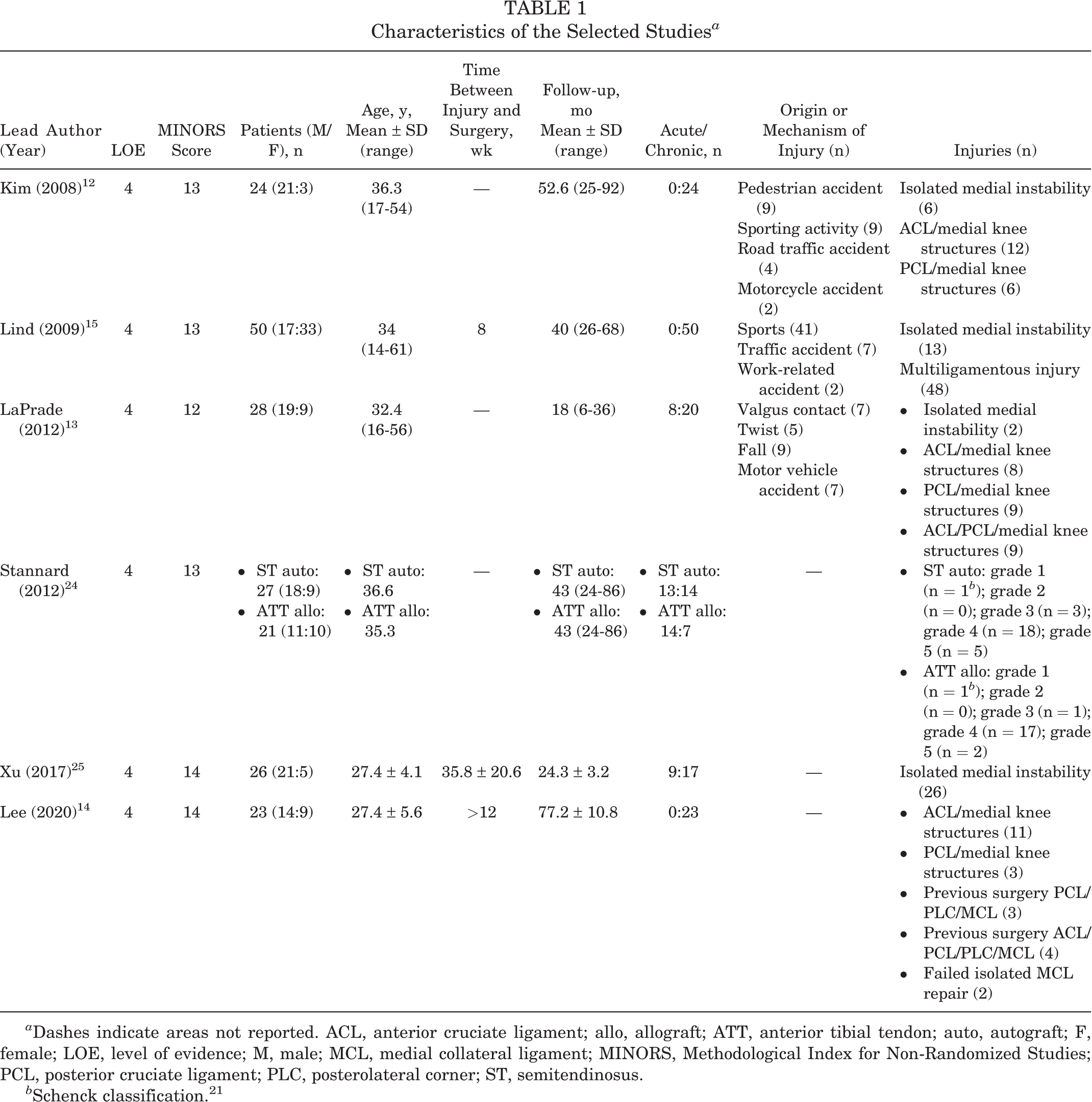
a Dashes indicate areas not reported. ACL, anterior cruciate ligament; allo, allograft; ATT, anterior tibial tendon; auto, autograft; F, female; LOE, level of evidence; M, male; MCL, medial collateral ligament; MINORS, Methodological Index for Non-Randomized Studies; PCL, posterior cruciate ligament; PLC, posterolateral corner; ST, semitendinosus.
b Schenck classification. 21
Patient and Study Characteristics
Table 1 shows the characteristics of the cohorts involved in the 6 selected studies and a summary of their data. The cohort of patients consisted of 199 participants (121 men and 78 women) with a mean age of 32.7 ± 3.9 years (range, 27.4-36.6 years). The mean postoperative follow-up was 42.5 ± 19.3 months (range, 6-92 months).
Origin
Three studies 12,13,15 reported the origin of the trauma. Of 102 patients, 60% (n = 61) were injured as a result of sporting activities, 20% (n = 20) had traffic accidents, and the remaining 20% (n = 20) sustained falling accidents.
Surgical Protocol
The data regarding the surgical technique followed in each of the examined studies are displayed in Table 2. All studies reported the type of graft used. A semitendinosus (ST) autograft was used in 3 studies, 12,13,24 an ST allograft in 1, 13 and an anterior tibial tendon (ATT) allograft in 2 studies. 14,24 A single femoral tunnel was utilized in 5 studies, 12 –14,24,25 and only 1 study 13 utilized 2 separate femoral tunnels. All studies used a double-bundle (sMCL and POL) reconstruction.
The femoral graft-fixation construct was performed with an interference screw (IFS) in 4 studies 13 –15,25 and a screw washer (SW) in 2 studies. 12,24 Tibial graft fixation was performed using an IFS in 2 studies 13,15 and a suture in 4. 12,14,24,25 All papers used 2 different tibial tunnels.
The tensioning of the POL reconstruction in limbs varied in terms of knee flexion, with positionings of 20° (1 study 13 ), 30° (4 studies 12,14,24,25 ), and 60° (1 study 15 ), in slight varus stress (2 studies 24,25 ) and neutral axial rotation (3 studies 13,15,25 ).
Surgical and Rehabilitation Protocol a

a allo, allograft; ATT, anterior tibial tendon; auto, autograft; DB, double bundle; IFS, interference screw; POL, posterior oblique ligament; ROM, range of motion; SB, single bundle; ST, semitendinosus; SW, screw washer; WB, weightbearing.
Rehabilitation Protocol
The rehabilitation protocol was different in each study, depending on whether the patient underwent an isolated MCL-POL reconstruction or if it was in combination with a cruciate ligament reconstruction.
A hinged brace and a block to extension were prescribed in all studies. Partial weightbearing was permitted, with timing ranging from day 0 to 6 weeks. Initial range of motion (ROM) exercises (from 0° to 30° and progressing toward tolerable levels) were allowed immediately after surgery or from 2 to 6 weeks thereafter. Similarly, passive and active exercises were recommended, with timing among the 6 studies ranging from 2 to 6 weeks.
Clinical and Functional Outcomes
Lysholm scores were reported in 4 studies, 12,14,24,25 with mean results improving from 67.2 ± 20.4 preoperatively to 89.4 ± 3 postoperatively. IKDC evaluation was applied to determine objective outcomes in 3 studies. 12,15,24 On the final follow-up, 85% of patients (n = 100) had “normal (A)” and “nearly normal (B)” knees, while 15% of the patients were reported to have “abnormal (C)” and “severely abnormal (D)” knees. Three studies 13,14,25 reported IKDC subjective scores, with mean scores improving from 45.8 ± 2.1 preoperatively to 84.8 ± 7.5 postoperatively. Three studies 14,15,24 used the Tegner score to evaluate the level of activity; 2 of these studies 14,24 reported pre- to postoperative improvement from a mean of 3.3 ± 2.4 to 6.3 ± 0.9.
Radiological Outcomes
Valgus stress radiographs were used in 3 studies 12 –14 to assess the extent of medial joint opening. A medial opening of 3 to 5 mm indicated an sMCL injury, which increased to 5 to 7 mm with a concomitant POL injury. In these 3 studies, the results decreased from a mean of 7.5 ± 1.1 mm preoperatively to 3 ± 3.1 mm postoperatively.
Return to Sports
The rate of return to sports was reported in 2 studies. Lind et al 15 furnished only postoperative data: 6 of 50 patients (12%) returned to high-level sports, and 44 (88%) returned to recreational sports after 12 months of postoperative follow-up. Lee and Kim 14 reported that 21 of 23 patients (91.3%) were able to engage in various sports activities, and 15 (65.2%) continued the same level of sports activities after 6.4 years of follow-up.
On the other hand, Stannard et al, 24 evaluating their patients’ rate of return to full activity, found that of the 71 patients, 35 (49%) returned to their prior level of functioning and 34 (48%) to a decreased level of functioning. Other studies have suggested 3 months as the time taken by patients to return to controlled activities 25 and 6-12 months as the time to taken to return to contact sports. 12,25 LaPrade and Wijdicks 13 reported that patients returned to sports and full activities after passing activity-specific functional and clinical tests.
Complications
All studies showed complication rates. Of 199 patients, 19 (10%) had complications: 8 (4%) wound infections; 4 (2%) instances of arthrofibrosis; 2 (1%) cases of heterotopic ossification; and single instances of septic arthritis, unsatisfactory ROM, pain and inflammation, cyclops lesion, and severe cartilage degeneration (Table 3).
Clinical and Functional Outcomes, Complications, and Return to Sports and Activity a

a Dashes indicate areas not reported. allo, allograft; ATT, anterior tibial tendon; auto, autograft; IKDC, International Knee Documentation Committee; Pre, preoperative; Post, postoperative; Rx, radiograph; ST, semitendinosus.
Discussion
The most important finding from the current systematic review is that most patients who have undergone sMCL-POL reconstruction to treat a grade 3 MCL injury, either in isolation or associated with knee ligamentous injuries, achieve satisfactory clinical and functional outcomes, a low rate of postoperative complications, and a high rate of return to recreational sports.
Our findings reveal that medial knee laxity due to grade 3 MCL injuries isolated or associated with cruciate ligament tears often occur because of sports activities (61%). A common injury is a valgus stress, combined with tibial external rotation, which can occur because of sporting activities such as football and skiing. 20 In general, the sMCL plays a primary role in providing valgus stability in the knee joint and a secondary role in providing internal and external rotational stability. In comparison, the POL serves a primary role in providing rotational stability and a secondary role in ensuring valgus and external rotation stability. Therefore, reconstructing the sMCL and POL simultaneously can improve the stability and biomechanics of the knee joint. However, these procedures are typically highly invasive and technically demanding.
Most patients (77.8%) underwent surgical reconstruction because of the chronic instability of the medial knee. However, 3 studies 13,24,25 also included patients (22.2%) with acute medial knee instability. In general, the surgical reconstruction of the injured sMCL is not recommended for acute cases, as the sMCL has the capacity to heal. In these circumstances, a selected group of surgeons advocated surgical reconstruction even for acute grade 3 cases with associated ligamentous injuries, as a nonoperative treatment can cause scarring and inadequate healing, leading to unsatisfactory clinical outcomes. 1,5
The technique for sMCL-POL reconstruction to treat grade 3 MCL injuries isolated or associated with ligamentous knee injuries has continued to evolve over the years and is increasingly effective in restoring significant valgus and rotatory stability. Kim et al, 12 Lind et al, 15 and Stannard et al 24 performed an anatomic double-bundle reconstruction using an autograft ST tendon 12,15,24 and a tibial anterior allograft 24 with a single femoral tunnel. LaPrade and Wijdicks 13 considered these 2 similar techniques as being more of a sling type and proposed a new anatomic double-bundle reconstruction procedure using 2 femoral tunnels and 2 tibial tunnels. However, the need for 2 tunnels, one each in the tibia and femur, has limited the uptake of this technique, especially in cases of multiple ligament reconstruction. Further, the tibial fixation of the graft remains a weak link in this technique, compared with the outcomes of surgical repair versus reconstruction using allograft in one group and autograft in the other. 24 Recently, Xu et al 25 and Lee and Kim 14 attempted a more anatomic medial complex reconstruction using a triangular vector with a single femoral tunnel, proximal and posterior to the medial femoral epicondyle. They assumed an anatomic triangular reconstruction to be more like the medial and posteromedial complex, which could provide more rotatory stability than the separated double-bundle reconstruction of the sMCL and POL.
In this systematic review, surgeons used various types of grafts and fixation methods in the mentioned techniques, based on their preference and experience. We found that most of the authors used an allograft tendon rather than an autograft tendon. However, good results have been obtained with both approaches. In general, allograft poses a potential risk for complications such as infection and irradiation-associated biomechanical degradation, entails additional surgical costs, and is unavailable in some countries. Autograft harvesting may intensify local tissue damage, pose the risk of donor site morbidity, and potentially weaken the dynamic medial stabilizers when using ST and/or gracilis tendons. 6
Limitations
This study has several limitations. The analysis of the literature revealed considerable heterogeneity among the analyzed studies in terms of the variety of injuries treated, time from injury to surgery, and difference in techniques (type of graft and fixation methods). In particular, the patients included in each study had medial knee laxity caused by a variety injuries, such as isolated grade 3 MCL injuries, LCA and/or LCP tears, and failed previous surgery of multiligament injuries. This heterogeneity may confound the results.
Another limitation is the methodological quality of the selected studies. All the studies were retrospective case series of a mixed cohort, without a control group and without using a combined POL reconstruction. This important methodological limitation highlights the need for additional well-designed prospective studies and further investigation of the issue.
The clinical relevance of this systematic review is that a combined cruciate ligament and sMCL-POL reconstruction is increasingly being recognized as useful for treating high-energy multiligamentous injuries associated with grade 3 MCL injuries, in general as well as among the athletic population. Based on the current review, this procedure appears to be safe and reproducible with satisfactory clinical and functional outcomes on the midterm follow-up. However, further high-quality studies are needed to confirm the validity of the present findings.
Conclusion
Although the technique of sMCL-POL reconstruction to restore medial knee integrity may differ based on the surgeons’ experience, it provides satisfactory clinical and functional outcomes, a high rate of return to sports, and a low rate of postoperative complications, as reported by the examined literature.
Footnotes
Final revision submitted August 5, 2021; accepted August 24, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.C. and B.S.C. are consultants for Arthrex. B.S.C. receives royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.