
Abstract
Background:
Injury to the ulnar collateral ligament (UCL) leading to medial elbow instability and possible ulnar neuritis is common in overhead-throwing athletes. Treatment may require UCL reconstruction (UCLR) and concomitant ulnar nerve transposition (UNT) for those with preoperative ulnar neuritis.
Purpose:
To evaluate the return-to-play (RTP) rates, clinical outcomes, and rates of persistent ulnar neuritis after concomitant UCLR and UNT in a cohort of baseball players with confirmed preoperative ulnar neuritis.
Study Design:
Case series; Level of evidence, 4.
Methods:
Eligible patients were those who underwent concomitant UCLR and UNT at a single institution between January 2008 and June 2018 and who had a minimum of 2 years of follow-up. Additional inclusion criteria were athletes who identified as baseball players and who had a confirmed history of ulnar neuritis. Patients were contacted at a minimum of 2 years from surgery and assessed with the Kerlan-Jobe Orthopaedic Clinic (KJOC) Shoulder and Elbow Score, Andrew-Timmerman (A-T) Elbow Score, Mayo Elbow Performance Score (MEPS), Single Assessment Numeric Evaluation (SANE) score, and a custom RTP questionnaire.
Results:
Included were 22 male baseball players with a mean age of 18.9 ± 2.1 years (range, 16-25 years). The mean follow-up was 6.1 ± 2.4 years (range, 2.5-11.7 years). Preoperatively, all 22 patients reported ulnar nerve sensory symptoms, while 4 (18.2%) patients reported ulnar nerve motor symptoms. At the final follow-up, 7 (31.8%) patients reported persistent ulnar nerve sensory symptoms, while none of the patients reported persistent ulnar nerve motor symptoms. Overall, 16 (72.7%) players were able to return to competitive play at an average of 11.2 months. The mean postoperative patient-reported outcome scores for the KJOC Shoulder and Elbow Score, MEPS, A-T Elbow Score, and SANE score were 77.9 ± 20.9 (range, 14-100), 92.7 ± 12.7 (range, 45-100), 86.1 ± 17.1 (range, 30-100), and 85.5 ± 14.8 (range, 50-100), respectively.
Conclusion:
This study demonstrated that after concomitant UCLR and UNT for UCL insufficiency and associated ulnar neuritis, baseball players can expect reasonably high RTP rates and subjective outcomes; however, rates of persistent sensory ulnar neuritis can be as high as 30%.
Injury to the ulnar nerve has been identified in the overhead-throwing athlete, owing to the repetitive valgus stress that these athletes place on their elbow joint during the throwing motion. 6,9 As the ulnar nerve traverses from the upper arm into the cubital tunnel (CT) just posterior to the medial epicondyle of the elbow, it is at its most vulnerable position for compression or traction. 21 At this point, extreme valgus stresses exhibited during the throwing motion can cause direct compression and/or traction of the nerve, resulting in characteristic neurologic symptoms including numbness, paresthesia, and potentially weakness in the medial forearm and hand. While these symptoms are often transient and may only initially present with the throwing motion, the tremendous valgus stresses dealt to the elbow joint may inflict damage to surrounding stabilizing structures in the elbow and CT, putting the ulnar nerve at a greater risk for injury and damage.
A number of different structures contribute to the CT, principally the CT retinaculum (arcuate ligament), the olecranon, the posteromedial elbow capsule, and the posterior bundle of the ulnar collateral ligament (UCL). 21 Meanwhile, the anterior bundle of the UCL is perhaps the most commonly injured structure, and a large body of literature 1,3,8 has been devoted to assessing damage to the UCL in overhead-throwing athletes and various reparative/reconstructive strategies to treat UCL pathology. Repetitive valgus stress has been shown to result in an overuse-type injury and microtrauma to the UCL, which can lead to partial or complete UCL tears and subsequent medial elbow pain and instability. 4,10 One notable biomechanical study 15 demonstrated that in the setting of UCL insufficiency, the neurovascular structures of the elbow, especially the ulnar nerve, are at an increased risk for compression, traction, and injury. For this reason, overhead-throwing athletes who are evaluated with UCL insufficiency may have concurrent ulnar neuritis.
Operative handling of the ulnar nerve in the setting of UCL insufficiency has remained controversial. While the earliest reports of UCL reconstruction (UCLR) for overhead-throwing athletes performed “routine” or “obligatory” ulnar nerve transposition (UNT), high rates of postoperative ulnar nerve complications have led subsequent researchers to reconsider this strategy. 7,13 As such, more recent studies 14,17 have suggested that UNT be selectively performed and reserved for only those who demonstrate preoperative ulnar neuritis. Nevertheless, many surgeons routinely perform UNT simultaneously with UCLR regardless of ulnar neuritis. 3,23
Although UCLR has been shown to be a highly successful independent surgery, there exists very little dedicated literature assessing the clinical outcomes of overhead-throwing athletes who undergo UCLR and concomitant UNT for a UCL tear with concurrent preoperative ulnar neuritis symptoms. The purpose of this study was to evaluate the return-to-play (RTP) rates, clinical outcomes, and more specifically rates of persistent ulnar neuritis after concomitant UCLR and UNT in a cohort of baseball players with confirmed preoperative ulnar neuritis. The authors hypothesized that patients would experience high RTP rates and patient-reported outcomes (PROs) as well as low postoperative persistent ulnar neuropathy rates after concomitant UCLR and UNT.
Methods
Institutional review board approval was received for this study, and all patients provided verbal consent per the conditions of the approval. Patients who were baseball players and underwent concomitant UCLR and UNT performed by the senior author (M.G.C.) between January 2008 and June 2018 were retrospectively identified from an institutional database. During this time period, 30 patients who identified as baseball players preoperatively met the inclusion criteria, and 22 (73.3%) were available to complete surveys at a minimum of 2 years after their surgery.
Patients who were able to be contacted via telephone and assessed with the Kerlan-Jobe Orthopaedic Clinic (KJOC) Shoulder and Elbow Score, Andrew-Timmerman (A-T) Elbow Score, Mayo Elbow Performance Score (MEPS), Single Assessment Numeric Evaluation (SANE) score, and a custom RTP survey. The custom survey elicited details including the current functional status of their elbow, level of competitive play before and after surgery, time to RTP, and the presence of ulnar neuritis. Evidence of preoperative and postoperative ulnar neuritis was elicited within the custom survey administered by trained interviewers and corroborated with the provider’s clinical notes. The interviewers were medical students who were uniformly trained by a sports medicine clinical fellow (R.A.J.) and the sports medicine–trained senior surgeon (M.G.C.) to precisely elicit a standardized, accurate assessment of the patients so as to minimize variability and bias. Sensory ulnar nerve symptoms were defined as numbness and/or paresthesia in the fifth and ulnar half of the fourth digits. Motor ulnar nerve symptoms were defined as exhibiting (1) first dorsal interosseous muscle weakness by the inability to maintain finger abduction against resistance, (2) ulnar-sided hand grip weakness, or (3) the inability to control precise movement of the fifth digit. The full surveys are provided as supplemental material to this article.
A thorough chart review of each patient’s clinical notes and imaging reports was performed to gather information on patient characteristics, injury history, surgical details, and postoperative status. UCL tears were categorized as either acute or chronic in nature. Tears were considered acute if there was a history of a confirmed traumatic event and the patient received operative treatment within 12 weeks. Tears were considered chronic in patients with no history of a traumatic incident, patients operatively treated ≥ 12 weeks after a traumatic event, or in the event of a traumatic incident in a player with a history of prior medial elbow pain for >1 year. Comparisons between players with acute versus chronic injuries as well as pitchers versus position players were conducted.
All patients underwent a preoperative physical examination in which they demonstrated medial elbow valgus instability as well as clinical symptoms of ulnar neuritis. The standard of care of our practice involves the use of magnetic resonance imaging to confirm the presence of a UCL tear as well as dynamic stress ultrasound imaging to evaluate for elbow instability. Patients with partial UCL tears (grades 1 and 2) were initially offered a trial of nonoperative treatment that included activity modification, a period of throwing cessation, physical therapy, and non-steroidal anti-inflammatory medication. If symptoms persisted, surgical treatment was thereafter offered. Those with complete UCL tears were offered prompt surgical reconstruction.
The UCLR technique was determined by the operating surgeon; either a standard modified Jobe technique or docking technique was used. All reconstructions regardless of technique were performed using a muscle-splitting approach via the common flexor-pronator tendon raphe. UNTs are performed for all patients with subluxating nerves or the presence of ulnar nerve symptoms; however, patients with a subluxating ulnar nerve but no symptoms were not included in this study. Ulnar nerves were transposed utilizing a fascial sling from the flexor-pronator fascia.
After surgery, the patient used a posterior-based splint for 7 to 10 days. After the initial splinting period, wounds were evaluated, and sutures were removed if necessary. The patient then used a hinged elbow brace with progressive advancement of motion over the next 4 to 6 weeks until full range of motion was achieved in the brace. Postoperative weeks 6 to 12 were focused on entire kinetic chain optimization, including scapular positioning, core, low back and lower extremity strengthening, and overall flexibility and coordination. After week 12, the patient began a baseball-specific RTP protocol, including a progressive hitting program. After week 20, the patient started an interval tossing program to return to competitive throwing. Ultimately, the athlete was allowed to RTP after full range of motion and strength were achieved, with no limitations or pain during baseball activities.
Statistical Analysis
Data that were continuous were reported as means with standard deviations, while categorical data were reported as frequencies with percentages. The Shapiro-Wilk test was used to assess the normality of the data. The Mann-Whitney U test was used to compare nonparametric continuous variables between 2 groups. Statistical significance was set at P < .05. All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) Statistics software Version 26 (IBM Corp).
Results
Patient Characteristics
As noted in Table 1, all patients were male with a mean age of 18.9 ± 2.1 years (range, 16-25 years). The mean follow-up time for the cohort was 6.1 ± 2.4 years (range, 2.5-11.7 years). On preoperative physical examination, 18 (81.8%) players had a positive Tinel sign, and 12 (54.5%) were found to have a subluxated ulnar nerve. There were 7 acute tears and 15 chronic tears. The cohort included 17 (77.3%) right-hand dominant players and consisted of 15 pitchers and 7 position players. All injuries involved the dominant throwing elbow. Overall, 7 players competed in high school, and 15 competed in college. The modified Jobe technique was performed in 18 (81.8%) patients, and the docking technique was performed in 4 (18.2%) patients.
Patient Characteristics (N = 22)a

aData are reported as mean ± SD or n (%).
Clinical Outcomes, RTP Rates, and PROs
At final follow-up, 16 (72.7%) players were able to return to competitive play at an average of 11.2 ± 2.6 months (range, 6-16 months). For those who were able to RTP, 12 (75%) players reported returning to the same or better level of performance as compared with before their injury, while 4 (25%) reported returning to a lower level of performance. Of the 6 (27%) players who did not RTP after surgery, 3 reported that persistent elbow symptoms were the reason for not returning to play, while the other 3 reported losing the desire to RTP. Preoperatively, all 22 players reported ulnar nerve sensory symptoms, while only 4 (18.2%) players reported ulnar nerve motor symptoms. At final follow-up, 7 (31.8%) patients reported persistent ulnar nerve sensory symptoms. Of these 7 patients, 5 reported improvement, 1 reported no change, and 1 reported worsening of the sensory symptoms. Meanwhile, all patients who were evaluated with preoperative ulnar nerve motor symptoms reported resolution of their symptoms. Notably, 1 patient who did not demonstrate preoperative motor symptoms reported that he developed difficulty moving his fifth digit during the postoperative period; this was persistent 6.5 years postoperatively.
Overall, the mean postoperative KJOC Shoulder and Elbow Score, MEPS, A-T Elbow Score, and SANE score were 77.9 ± 20.9 (range, 14-100), 92.7 ± 12.7 (range, 45-100), 86.1 ± 17.1 (range, 30-100), and 85.5 ± 14.8 (range, 50-100), respectively. There was no difference between PRO surveys with respect to pitcher versus position status (Table 2). Similarly, players with acute tears did not demonstrate statistically different PROs compared with those with chronic tears (Table 3).
Comparison of Subjective Patient-Reported Outcomes Between Pitchers and Position Players a

a Data are reported as mean ± SD. A-T, Andrew-Timmerman; KJOC, Kerlan-Jobe Orthopaedic Clinic; MEPS, Mayo Elbow Performance Score; SANE, Single Assessment Numeric Evaluation.
Comparison of Subjective Patient-Reported Outcomes Between Acute and Chronic UCL Injuries a
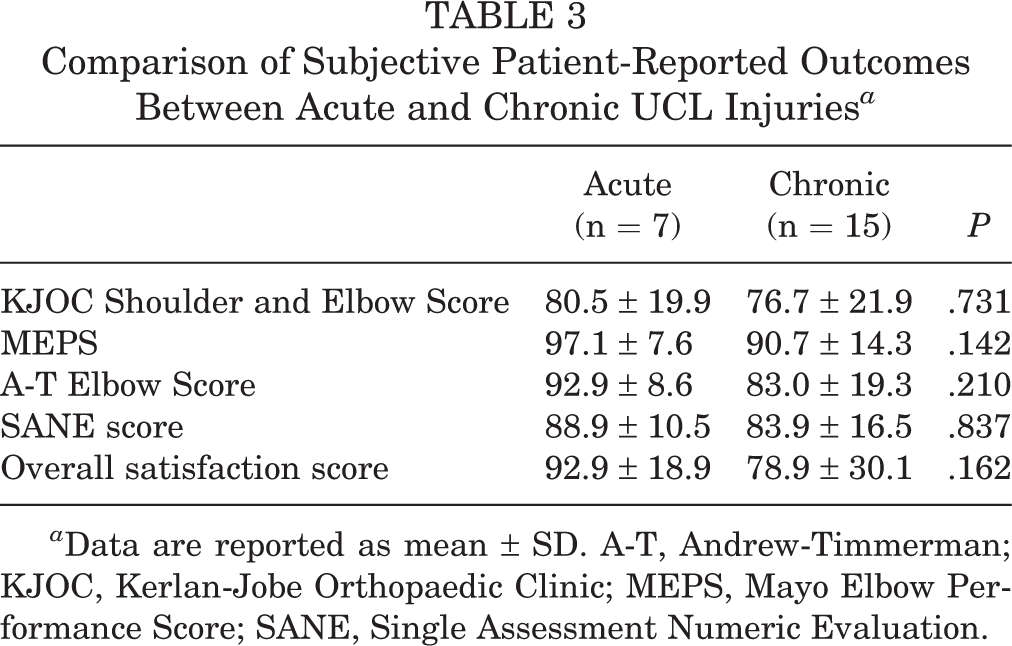
a Data are reported as mean ± SD. A-T, Andrew-Timmerman; KJOC, Kerlan-Jobe Orthopaedic Clinic; MEPS, Mayo Elbow Performance Score; SANE, Single Assessment Numeric Evaluation.
At final follow-up, there were 3 patients who sustained injuries postoperatively to the ipsilateral shoulder as a result of throwing. Two patients reported sustaining a labral injury at a mean of 26 months after their UCLR, of which 1 was treated operatively. Another patient sustained a rotator cuff injury 12 months postoperatively that required surgery. No patients sustained any type of reinjuries to the UCL. One patient had a superficial postoperative infection at the surgical site that was treated with antibiotics in the outpatient setting. Another patient was brought back to the operating room 3 days after his index surgery and was found to have a partial injury to his ulnar nerve, which was repaired. This was the same patient who later developed new-onset postoperative ulnar nerve motor symptoms and had persistent ulnar nerve sensory symptoms.
Discussion
The purpose of our study was to evaluate the RTP rates, clinical outcomes, and rates of persistent postoperative ulnar neuritis after concomitant UCLR and UNT in a cohort of baseball players with confirmed preoperative ulnar neuritis. In this study, clinical outcomes indicated that 72% of athletes returned to any level of competitive play. Contrary to the hypothesis, however, >30% of patients reported experiencing persistent ulnar neuritis symptoms at final follow-up.
Some of the earliest work 7,13 on UCLR described routine submuscular UNT and release of the flexor-pronator mass during reconstruction of the UCL. While groundbreaking, outcomes of these early studies demonstrated exceptionally high rates of postoperative ulnar nerve complications, and concerns lingered over potential healing issues and subsequent increased risk of injury to the flexor-pronator mass, especially in throwing athletes. Eventually, a shift toward the broad use of subcutaneous UNT and a muscle-splitting approach gained favor, as it potentially provided a number of benefits to throwing athletes, such as less surgical morbidity and much lower postoperative ulnar nerve complication rates. 2,18 One study 2 in which patients received routine subcutaneous UNT along with UCLR found that 90% of patients with preoperative ulnar neuritis symptoms achieved resolution at final follow-up and only 1 patient developed postoperative transient ulnar neuritis, which resolved at 10 months.
More recently, the role of routine UNT has been questioned, and some studies 14,19 have suggested that UNT be performed only when patients have preoperative ulnar neuritis or when “indicated” to reduce inadvertent iatrogenic injury to the nerve. Paletta and Wright 17 echoed similar sentiments in their study of 25 high-level baseball players, in which they transposed the ulnar nerve in only 2 patients because the nerve was hypermobile and subluxating. They went on to report only a single case of postoperative transient ulnar nerve sensory neurapraxia. 17 Another prevailing rationale against routine UNT is based on the idea that the development of ulnar neuritis is more likely secondary to medial elbow laxity from UCL insufficiency that results in undue ulnar nerve strain; hence, reconstructing the ligament alone may be sufficient to resolve any ulnar nerve symptoms. In support of this notion, Thompson et al 22 reported on a cohort of 83 athletes after UCLR without UNT and found that of the 20 athletes who reported preoperative ulnar neuritis, only 1 had postoperative transient ulnar neuritis, which went on to resolve at final follow-up.
In comparison, the current study of 22 baseball players with preoperative ulnar neuritis who received concomitant UNT found that 7 (31.8%) specified persistent ulnar nerve sensory symptoms at final follow-up; however, 5 (23%) reported improvement from their preoperative baseline, and only 2 (9%) reported no change or worsening of their symptoms. While the retrospective nature and small sample size of this study preclude us from making any substantiative recommendations on the role and efficacy of selective UNT, it does call for further investigation to define which patients are most likely to truly benefit from—and to what degree—concomitant UNT.
Ultimately, the paramount concerns of athletes after surgery are whether they are able to return to their sport and what their postoperative level of performance will be. The current study demonstrated that 72.7% of athletes returned to play, although only 55% reported returning to the same or better level of performance. However, only 3 (50%) of the athletes who did not RTP reported that their elbow was the source of the issue, suggesting reasonably reliable surgical outcomes. Nonetheless, the RTP rate among this cohort falls below the RTP rate of 86.2% reported by a systematic review on athletes after UCLR. 12 Furthermore, the mean KJOC Shoulder and Elbow Score of our cohort fell toward the lower end of the spectrum with respect to overhead-throwing athletes after UCLR, which ranges broadly from 77.0 to 90.4. 11,16,20 Considering that this cohort consisted only of athletes who were evaluated with preoperative ulnar neuritis and underwent concomitant UNT, it is possible that this may have influenced lower postoperative outcomes.
These findings may also indicate that players who have concomitant ulnar nerve injury with a UCL tear have a more significant injury to their elbow and perhaps patient expectations should be tempered. Previous studies, however, have alluded to a possible negative association of ulnar nerve handling and postoperative outcomes. In another systematic review on UCLR, Vitale and Ahmad 23 reported that obligatory/routine ulnar nerve handling as compared with no ulnar nerve handling resulted in lower rates of “excellent” ratings on the Conway-Jobe scale and higher postoperative ulnar neuropathy rates (75% vs 89% and 9% vs 4%, respectively). Furthermore, Clain et al, 5 in their systematic review on ulnar nerve complications after UCLR, found that routine UNT was associated with higher rates of postoperative ulnar neuropathy compared with the group without any ulnar nerve handling (P < .001). Again, while it is possible that ulnar nerve handling, whether warranted or not, influences postoperative outcomes, its value is still undetermined, and further investigation into when and how the ulnar nerve should be transposed in the setting of UCL insufficiency is necessary.
Limitations
While this study represents the first to exclusively evaluate the outcomes of concomitant UCLR and UNT in a cohort of overhead-throwing athletes with preoperative ulnar neuritis, there are a number of limitations that exist. Principally, this was a retrospective investigation and was therefore subject to recall bias and selection bias, as in any other study of this nature. Furthermore, this study lacked preoperative data, making it difficult to estimate the true benefit received from this surgical intervention. Beyond this, there was no comparative group of athletes who did not have UNT, which precluded us from determining the true value of the concomitant procedure. Nonetheless, these findings highlight the need for additional investigation dedicated to determining the optimal implementation of concomitant UNT and which population may truly benefit from it. Finally, while this type of cohort is the largest reported to date, the sample size was still limited.
Conclusion
This study demonstrated that after concomitant UCLR and UNT for UCL insufficiency and associated ulnar neuropathy, baseball players can expect reasonably high RTP rates and subjective outcomes; however, rates of persistent sensory ulnar neuritis can be as high as 30%. Handling of the ulnar nerve in the setting of UCL insufficiency is currently being debated; thus, further investigation is warranted to define precise indications and optimize outcomes for this group of patients. Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671211055428.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211055428 - Return-to-Play Rates and Clinical Outcomes of Baseball Players After Concomitant Ulnar Collateral Ligament Reconstruction and Selective Ulnar Nerve Transposition
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211055428 for Return-to-Play Rates and Clinical Outcomes of Baseball Players After Concomitant Ulnar Collateral Ligament Reconstruction and Selective Ulnar Nerve Transposition by Somnath Rao, Taylor D’Amore, Donald P. Willier, Richard Gawel, Robert A. Jack, Steven B. Cohen and Michael G. Ciccotti in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted June 18, 2021; accepted July 14, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.D. has received education payments from Liberty Surgical. S.B.C. has received research support from Arthrex and Major League Baseball; education payments from Liberty Surgical; consulting fees from ConMed Linvatec and Zimmer; speaking fees from Zimmer; royalties from SLACK and Zimmer; and hospitality payments from AstraZeneca, Boston Scientific, DePuy, Integra, ERMI, DJO, Ferring, Horizon Pharma, and Stryker. M.G.C. has received grant support from DJO; education payments from Liberty Surgical; and hospitality payments from Arthrex, Cayenne Medical, DePuy, Stryker, Tornier, and Zimmer. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Thomas Jefferson University.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.